Article Text

Abstract
Background Musculoskeletal disease is one of the leading clinical and economic burdens of the UK health system, and the resultant demand for orthopaedic care is only set to increase. One commonly used and one of the most expensive hardware in orthopaedic surgery is the surgical drill and saw. Given financial constraints, the National Health Service (NHS) needs an economic way to address this recurring cost. We share evidence of one frugal innovation with potential for contributing to the NHS’ efficiency saving target of £22 billion by 2020.
Methods Exploratory case study methodology was used to develop insights and understanding of the innovations potential for application in the NHS. Following a global search for potential frugal innovations in surgery, the Arbutus Drill Cover System was identified as an innovation with potential to deliver significant cost savings for the NHS in the UK.
Results The Arbutus Drill Cover System is up to 94% cheaper than a standard surgical drill available in the UK. Clinical and laboratory tests show that performance, safety and usability are as good as current offerings in high-income countries and significantly better than hand drills typically used in low-and-middle-income countries. The innovation meets all regulatory requirements to be a medical device in the Europe and North America.
Conclusions The innovation holds promise in reducing upfront and life span costs for core equipment used in orthopaedic surgery without loss of effectiveness or safety benchmarks. However, the innovation needs to navigate complicated and decentralised procurement processes and clinicians and healthcare leaders need to overcome cognitive bias.
- Frugal innovation Reverse innovation Orthopaedic surgery
Statistics from Altmetric.com
Introduction
The primary objective of this paper is to present the Arbutus Drill Cover System, a promising medical device with significant potential for cost saving for the National Health Service (NHS). This work also reflects on the significant challenges faced by entrepreneurs and innovators as they seek to scale up promising ideas in the UK and further afield.
Traumatic injuries are one of the leading causes of disability and death worldwide, accounting for nearly 1 in 10 deaths each year.1 Ninety per cent of injury deaths occur in low-and-middle-income countries (LMICs).2 Injuries in the UK result in a substantial population burden in terms of disability and premature mortality.3 Musculoskeletal disease accounts for >25% of surgical interventions within the NHS.4 One of the critical kits commonly used in orthopaedic surgery is the surgical drill and saw. All orthopaedic trauma cases require a drill except closed reduction of fractures in children. Against a background of an ageing population and rise in non-communicable diseases, there will be an ever-increasing demand for orthopaedic care. As trauma affects a relatively younger population, it accounts for more productive years of work lost than other illness, with an enormous economic and societal impact.
The significant £20–30K cost of current clinical surgical drills has meant that trauma and orthopaedic surgeons in LMICs resort to using imprecise and slow hand drills or unsterile hardware drills, with serious consequences, including disfigurement, severe infection and loss of life.5 In 2012 the lead author undertook an orthopaedic fellowship at Beit-CURE International Hospital in Malawi, where he observed the practice of wrapping a commercially available hardware drill with an unsterile crude cover; a common practice across LMICs. At the same time, in Uganda a group of biomedical engineering students from the University of British Columbia also witnessed the same behaviours and sought to convert this jugaad practice into a frugal innovation through a structured innovation and design process.6 7 Arbutus Medical Inc. was incorporated in 2014 for the purposes of commercialising the company offering.
Through case study development, we sought to understand the conception, development and implementation of the Arbutus Drill Cover System for the purposes of assessing transferability to the NHS, specifically at the West Middlesex University Hospital.
Methods
Over a 2-year period the Institute of Global Health Innovation (IGHI) has conducted an international search for frugal innovations with potential application by healthcare providers in high-income countries (HICs; ie, potential for reverse innovation).8 9 In 2015 we conducted a global search of hundreds of cost-saving innovations including products, processes and policies that addressed all types and domains of healthcare.10 ,11 Key criteria used to evaluate frugality included affordability, adaptability and accessibility. In 2016 we narrowed down this search to shortlist those related specifically to surgery with potential for piloting in the UK’s NHS. One of the most promising offerings we found in surgery is the Arbutus Drill Cover System. An exploratory case study methodology was used to collect information about the Drill Cover System and the company behind its development via a range of data collection techniques comprising observation, interview and documentary analysis for the purpose of developing insights about the applicability of the innovation for the UK NHS. We focused more on the technology and its potential for piloting, though we also came to understand more about the organisation backing this technology as part of assessing prospects for piloting and scaling. Researchers (IA/YB) undertook multiple telephone and face-to-face interviews with the co-founders of Arbutus Medical to understand the conception and development of the Drill Cover System. Concurrently, MP/IA/YB analysed documents related to the innovation including company presentations; laboratory findings; usability feedback; technical instructions and regulatory approval information. Subsequently, researchers (MP/YB/AI) undertook an international field trip to Uganda and Kenya, where three hospitals were visited, to gain perspectives of the Arbutus Drill Cover System from front-line healthcare workers; this included observing the drill in surgeries and at the point of assembly and disassembly.
Results
How was the innovation conceived?
In 2013, as part of the University of British Columbia’s Engineers in Scrubs programme, a team of biomedical engineering researchers, orthopaedic surgeons, registered nurses, reprocessing staff and health administrators from Canada and Uganda looked at pressing clinical needs at Mulago Hospital in Kampala, Uganda. They identified the problems arising from inadequate availability of expensive surgical drills and embarked on developing a solution. The project ideation and lead target market in East Africa is facilitated by urgency of need and lax regulatory enforcement. However, design, engineering, manufacturing, quality management system, as well as strategic and operational control are based in Canada.
What are the key features?
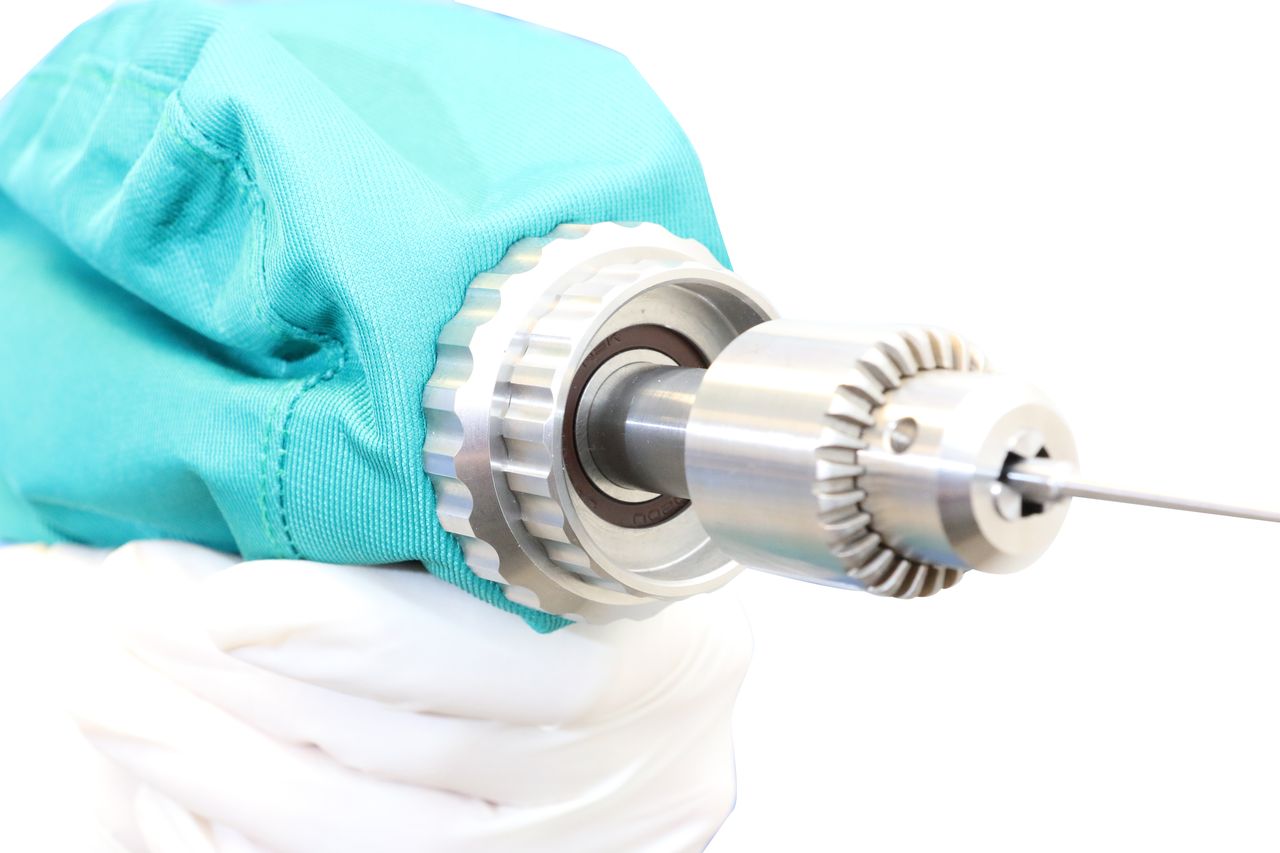
The Arbutus Drill Cover System is a sterilisable and reusable cover that fully encloses a hardware drill, transforming it into a surgical grade drill. The Drill Cover System consists of a robust, double-layered surgical-grade textile which attaches to a drill’s mechanics via a waterproof chuck adapter interface (figures 1–6). This creates a completely sealed barrier between the non-sterile drill on the inside and the sterile surgical field outside. The chuck has a lifetime of at least 600 use cycles when reprocessed appropriately. It can be autoclaved up to 75 times and will be sterile after 30 min exposure of steam autoclave at 121°C, or after 15 min at 131°C, either by using gravity displacement or prevacuum autoclaves.10

Arbutus Medical Drill Cover fully sealed with DeWalt drill beside.

Arbutus Medical Drill Cover System disconnected to show chuck mechanism and linen, with DeWalt drill beside.

Drill Cover System being assembled.

Close-up of the Drill Cover System, specifically highlighting fully sealed waterproof chuck interface.

Oscillating saw launching towards the end of 2017. Product will feature a quick-change cam mechanism for easily switching blades (not shown here).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Cannulated drill and reamer launching early 2018. This features a universal quick-change interface for easy exchange of AO, Jacobs, Hudson and K-wire collet during practice.
Arbutus Medical Inc. provides two versions; the S, which is used with a surgical drill to increase uptime throughout the day and extend its lifetime by eliminating the harsh sterilisation cycles that drills must otherwise undergo, and the Hex, which is used with a standard hardware drill. (For product suite, please see online supplementary video 1). It has been designed for easy assembly following sterile technique, and the cover material is soft enough for the surgeon to control the drill through the fabric without hindrance. The textile and manufacturing techniques follow an AAMI/ANSI PB70 standard for Level 4 medical barriers. The Drill Cover is CE marked as a Class I medical device, registered with the US Food and Drug Administration and approved with Health Canada. Further tests are being conducted to reclassify the whole package of cover plus drill as a CE Class IIa device.
Supplemental material
How does it work?
The Arbutus Drill Cover System is assembled by inserting a non-sterile hardware drill into a sterile cover. The bag edges are rolled down with fingers tucked under during loading, before being rolled back and sealed to encase the hardware drill. (For loading and assembly, please see online supplementary video 2). This is a standard process used in other types of surgery to provide a sterile barrier, most notably arthroscopic procedures, where a cover is placed over a non-sterilisable camera and light source.
Supplemental material
Turnaround time between cases can be as quick as 1 min, by switching out a soiled Drill Cover for a sterile one; permitting front-line staff to treat more patients with faster drill turnaround between cases. The Drill Cover can be used with both inexpensive off-the-shelf hardware drills or with current surgical drills, thereby prolonging their life span by reducing wear and tear from repeated autoclaving and requiring the purchase of fewer clinical drills. Hence, while there is greater potential for cost saving in using the cover along with the commercial hardware drill, there are benefits to using the cover alone.
The benefit in using commercial hardware drills is the significantly lower upfront cost investment and the ability to easily replace the drills in the event of breakdown. The company recommends the Drill Cover System is paired with a DeWalt DCF610S2; an affordable and robust hardware drill carefully selected and tested to closely match the speed, torque and power offered by surgical drills. The DeWalt drill is commercially and widely available in hardware stores around the world. User feedback we collected from surgeons suggests that in many cases they find the commercial hardware drill, specifically the DeWalt, to be ergonomically easy to use, small, compact, light, powerful and overall better than a lot of old-generation surgical drills used in the developing world and also many NHS hospitals.
The DeWalt drill has been electrically tested to ensure there is no interference with other operating room equipment, and tests show that the hardware drill battery lasts much longer and is cheaper to replace. The recommended DeWalt drill costs as little as £100 versus £23–30K for a contemporary surgical drill, replacement batteries cost as little as £30 versus £1500, respectively. As the DeWalt drill is a critical component of the Arbutus Drill Cover System, the company’s regulatory and ISO 14971 Risk Management process takes into account the safety and efficacy of the DeWalt drill when used as part of the system.
How has the company been funded?
Arbutus Medical Inc. was established in 2014 as a for-profit medical devices company funded by Grand Challenges Canada, a non-profit initiative funded by the Government of Canada—with an initial investment of $1 million. Prior to this the company received support from Canada-based Coast Capital Savings Innovation Hub, a social venture accelerator operated by the UBC Sauder School of Business, and the Lean Launch Pad Accelerator programme offered by entrepreneurship@UBC.12 The company has also received funding from impact angel investors with a dual focus on financial and health impact returns. These include physicians, successful former and current entrepreneurs, family offices/foundations (eg, Threshold Impact, D. Keith MacDonald Foundation) and sophisticated healthcare investors (Angel One Network, SWO Angels).
What is the business model?
Arbutus Medical Inc. seeks to sustain and expand its offering by earning a profit from the sale of the Arbutus Drill Cover System. Presently, Arbutus products are available in 15 countries, and the company hopes to expand its reach across Africa, Latin America, India, Turkey and the Philippines in the near future. Most recently it has begun to explore markets in the USA, Canada, South Africa and the UK, with clinical pilots in the planning stages in each country. In the developing world it sells to hospitals through distributors.
A financial and economic model co-developed in partnership with Imperial College Healthcare Partners, a member organisation of the NHS academic health science network, and in conjunction with Arbutus Medical Ltd, evaluated initial capital investment based on recent and real purchasing data, as well as projected the 5-year costs of supplying the NHS.
At the national level, for example, if the NHS were to replace all incumbent drills with similar offerings (approximately 5000 at estimated cost of £23K per drill), this could cost £115 million. However, if all of NHS providers were to move to the Arbutus Drill Cover System (estimated cost per drill £1500), it could cost as little as £7.5 million; an upfront saving of 94% in immediate capital outlay.
At the hospital level, for example, the total costs to equip and maintain surgical drill equipment for two theatres over 5 years would be £3 24 500 (11 drills at £23K per drill with annual battery replacement for years 2–5) while the Arbutus Drill Cover System would be £47 993 (2 drills+2 saws; 22 initial linens; 14 p.a. replacement linens and 4 replacement batteries per drill for years 2–5), a saving of 85%.
What is the operating model?
Design, engineering and manufacturing are based in Canada while sales and marketing is spread globally, primarily in the developing world. Arbutus Medical has nine full-time employees and over half a dozen contractors and interns. The company’s key performance metrics are both sales and revenues as any typical company, but also the impact that they have socially as measured by number of patients treated and disability avoided. The product’s key performance metrics are number of cycles possible for delivering safe surgery and cost savings compared with competitors, as well as the ease of use and integration into existing surgical workflows.
How is the innovation being spread?
The development of the Arbutus Drill Cover System has always been grounded in the needs of front-line clinicians and patients, with a vision to provide increased access to safer surgery. As such they have developed a network of clinical champions, which have helped spread knowledge about the innovation and the company vision.
To date the Drill Cover System has been used to treat 30 000 patients in 50 hospitals across 15 LMICs. In all of their global markets, the company relies on local distributors, with support from local staff on the ground. In addition, the company leverages partnerships with orthopaedic education and humanitarian organisations like the AO Alliance Foundation to create awareness of the product by supporting training activities globally. In order to support the most underserved communities, Arbutus also works with groups like Medecins Sans Frontieres and Canadian Relief for Syria to introduce the Drill Cover System for conflict and disaster relief.
Evidence for use in the HIC markets is currently developing; this includes sales to the Canadian military, where feedback from field use has been very positive and plans are under way to possibly replace all existing surgical drills with the Arbutus products in the field. The company is also hoping to support a pilot use case in the UK, which is being planned by the IGHI and Imperial College Health Partners (ICHP).
What are the future prospects?
While the innovation was initially conceived and developed for the needs of LMICs, it also provides an opportunity for hospitals in HIC to save money while still meeting institutional requirements. Given the financial pressures on healthcare providers in HICs, and the significant cost-saving potential, this may represent a more stable market for growth.
Future product improvements include an oscillating saw, cannulated drill and reamer functionality, and a quick coupling mechanism for numerous attachments. These incremental enhancements have been made to align closer with current surgical drill offerings in HICs. The company hopes to launch the saw at the end of 2017 and the cannulated drill & reamer at the beginning of 2018.
What were/are the big challenges to making this successful?
Initially, the main challenge was in achieving regulatory approval; however, these hurdles have now mostly been overcome through investment in design, engineering and testing of products by third-party evaluators. Beyond product development, for small start-ups like Arbutus, global marketing, securing distribution networks and navigating procurement processes are some of the big challenges they face. Presently, the company is exploring the best sales strategy for increasing market share in LMICs. Procurement processes can be complex and opaque as Arbutus Medical Inc. is restricted to sales through locally registered distributors in some contexts. Unfortunately, these distributors are more interested in selling ‘big-ticket’ items, where sales effort is less and margins can be greater compared with the necessary repeated sales of a low-cost item such as the Arbutus Drill Cover System. Indeed, communication between distributors and hospitals can be poor, and evidence was found of bags being used beyond their life span, a potential patient safety risk, which is contrary to and threatens Arbutus’s vision of increasing access to safer surgery. Furthermore, distributors are also not always interested in selling to the tier 2 and and 3 hospitals, where poorer patients are treated, and which Arbutus wants to reach, and so alignment of vision between the right distributor and the company is key.
In LMICs, Arbutus Medical Inc. faces intense competition from multiple other drilling solutions; these include hand drills, homemade but unsafe imitation drill covers, low-cost Chinese manufactured surgical drills and donated Western surgical drills. In all hospitals visited evidence was found of offerings being used simultaneously and interchangeably. Proving cost-effectiveness versus low-cost Chinese manufactured drills is proving challenging, especially where quality standards for manufacturing processes and longer-term cost savings are lower down the list of procurement prerequisites. Furthermore, once Arbutus becomes more widely known, it would not be surprising to see use of replicas in unprotected developing markets. To further compound the challenges, most recently incumbent manufacturers, such as Stryker, have begun to offer specific solutions for LMIC markets, though these offer a reduction of only about 30%–50% compared with Western offerings, while Arbutus product can offer up to a 94% reduction.
How were the major challenges overcome?
Arbutus is working closely with distributors like Crown Healthcare Africa and leading global orthopaedics education organisation AO Alliance Foundation to develop the best model for scaling. In India, the company founders are working with a range of organisations to develop market access strategies, including Intellecap and Sanrai International. The Arbutus team are supported through mentorship by a number of industry experts such as the senior management team of Edmonton-based medical device company priMED Medical Products and the former Africa Director for Johnson & Johnson surgical sales who sits on the Arbutus Board.
There is also still need to address demand for economic evidence of cost saving especially against Chinese drills. One option could be to offer a subscription model with unlimited number of Drill Covers for a set monthly fee. A Chinese drill may last anywhere from 1 to 3 years based on quality and may cost as little as $1500 (£1200); a subscription model would need to compete both in cost and life span. However, such a model could avoid the danger of bags being overused beyond the recommended number of cycles, resulting in patient safety and brand risk.
How is impact evaluated?
Impact is projected based on estimated number of surgeries performed with the Arbutus Drill Cover System from client hospital facilities. At specific sites the company is trying to measure more complex clinical and socioeconomic indicators; work is ongoing. Laboratory tests have examined drilling time; drilling accuracy; plunge depth, weight and size; drill speed and torque. Reputable external laboratories have undertaken in-depth electrical safety and hydrostatic pressure testing for barrier performance, as well as comprehensive cleaning and sterilisation validation. A full list of tests is shown in table 1.
Evaluations completed on the product
Currently, limited data are available on clinical outcomes compared with alternative drilling methods; however, there have been no reported adverse events over the course of >30 000 cases performed with the Drill Cover System. Nevertheless, the Drill Cover System meets all the required standards for use in the UK, and clinical outcome data are only needed as part of a postmarket analysis.
Discussion
Does the UK need this innovation? With the NHS under pressure to save £22 billion by 2020, any little or significant cost savings can contribute towards that goal. We have explored this one specific frugal innovation to evaluate potential savings it affords. At £10 billion, musculoskeletal disease has the third largest budget and already accounts for >25% of surgical interventions within the NHS.4 The Arbutus Drill Cover System presents a viable, regulatory approved alternative, which is much cheaper than mainstream commercial offerings generally considered in procurement. The UK is estimated to have 5000 surgical drills that each cost around £23 000, which is a major and critical component needed in orthopaedic surgeries. The Arbutus Drill Cover System costs around £1500. As shown above, depending on whether a comparative assessment is done for one hospital or for all of the NHS, and whether it is done for upfront costs or total costs incurred for a period of 5 years, potential savings range from 85% to 94%.
According to anecdotal evidence from surgeons working in the NHS, some of the drills currently being used are not fulfilling their expectations. Drills are often outdated and will soon need replacement. The more likely and only current option is to procure exorbitantly expensive clinical drills. Incumbent offerings involve autoclaving the whole drill along with the battery, a long established practice and one that is only now beginning to be challenged out of necessity of unaffordability in low-income settings and increasing pressures for savings in high-income settings. The alternative practice of only autoclaving the cover could deliver a cost reduction. And quality of care would be unchanged but at a fraction of the cost.
Hospitals are typically equipped with many contemporary and expensive drills because turnaround time can be long for sterilisation of equipment, which is typically done offsite. The Arbutus system requires fewer drills, whether surgical or hardware ones, as only the cover needs to be swapped and sent off for sterilisation after each surgery. Given there are many expensive drills already in use, to make the transition smoother from the old to the new, the life span of existing surgical drills can be prolonged as fewer are needed and the drill and battery itself does not need to be sterilised after each surgery.
Evidence of use in the Western markets is currently developing; this will make it easier to sell the device in the UK, Canada and the USA. This includes sales to the Canadian military, where feedback has been very positive and plans are under way to possibly replace all existing surgical drills with the Arbutus products in the field. As well, Arbutus is currently launching a pilot at the four largest teaching hospitals in Johannesburg, South Africa, with clinical champions bought in. Similar pilots are being planned in Canada and the USA. Finally, the company is also supportive of facilitating a pilot use case in the NHS, which is being planned by the IGHI and ICHP.
IGHI and ICHP are working closely with Arbutus to build the use and business case for NHS to consider adopting this innovation through a pilot study at major London hospitals. Arbutus is supportive of this pilot and is ready to back its product offering with warranty and replacement guarantees. Drills are covered by a 2-year manufacturer’s warranty. Arbutus Drill Cover Linens are covered for 75 cycles given normal use conditions. Arbutus Drill Cover Chucks and Adapters are covered by a 1-year Arbutus warranty. As a positive show of confidence and support, and to help de-risk the initial use case, the company is willing to consider a partial refund, rebate or free replacements if actual use case scenario significantly differs from the predicted model.
The technology offering as an innovation cannot be considered without carrying out due diligence on the type of organisation backing it, its capacity to scale up and meet the requirements of large health systems. The company is backed by impact investors and venture capital funds like Grand Challenges Canada. The company is run by a team of dedicated bioengineers and social entrepreneurs, who are supported by reputable mentors. The company has partnered with the AO Alliance Foundation, one of the leading orthopaedic education institutions and has secured professional champions in several front-line and major public, private and non-governmental organisation-based hospitals who are using it and providing crucial user feedback for further development of the offering. However, most of these are front-line surgeons (see, for instance, article in the Guardian 13), and while they are important to secure buy-in for use in the theatre, Arbutus probably needs to extend its list of innovation champions to procurement decision-makers.
The innovation journey from bench to bedside is fraught with challenges and risks. Some potential challenges to wide-scale adoption that need to be considered by any organisation seeking to pilot this for use in HICs include
In LMICs, incumbent companies are already giving away reconditioned drills in target market areas of the Arbutus drill. They are also coming up with less costly alternative models (eg, Stryker System G). Low-cost Chinese competitors are also available and range from $800 to $3000, but vary significantly in quality.
In the NHS, behavioural reticence and cognitive bias could render uptake of Arbutus Drill Cover a slow process.14 15 But these can be overcome with client education and evidence of safety and efficacy as well as through directives from management in favour of cost-efficiency savings.
As the Drill Cover needs to be replaced after 75 cycles, NHS procurement decision-makers need to be convinced of overall system-wide cost savings beyond just the initial capital outlay. This system analysis is under way between IGHI, ICHP, Arbutus and pilot test sites.
While the parties involved in this study have attempted to carry out preliminary due diligence on the supplier insofar as proposing and planning pilot use cases, the full due diligence activity for wide-scale adoption is best carried out by the procurement departments negotiating the full deal.
This paper contributes to knowledge and practice in four ways. First, we have used the Arbutus Drill Cover System as an exemplar of the challenges faced by innovations conceived in LMIC, and by entrepreneurs and innovators, as they seek to spread innovations within HICs. Second, we have shown an example of how publicly funded innovation centres such IGHI and ICHP can act as impartial intermediaries which conduct due diligence on innovative startups and also can help them to navigate complicated and confusing large healthcare systems such as the NHS. Third, the write-up of this case study should be useful as a case template for use in other publications that present the potential of innovations. Fourth, we have presented here the prospects of potentially significant cost savings from one specific frugal innovation. At the same time we caution against relying too much on one product for wide-scale savings across a large health system. But our argument here is that such consideration for testing and implementation needs to be taken piecemeal, step-by-step and meticulously through small but several pilot tests which requires participation and support from several stakeholders. Such efforts, when taken together, can offer significant savings across the system. And this is only possible if we embrace cultural change and create openness among health systems to innovations from unusual sources and that involve unorthodox practices which challenge long-held practices.
Conclusions
As a frugal innovation, the Arbutus Drill Cover medical device holds much promise in reducing upfront and life span costs for one of the most fundamental equipment to the practice of orthopaedic surgery without any loss of effectiveness or safety benchmarks. The innovation has gone through rigorous internal and third-party evaluations for medical devices. However, if the NHS is to realise the significant cost-saving potential of the Arbutus Drill Cover System, the innovation will need support to navigate the complicated and decentralised procurement processes of such a large health system, and clinicians and healthcare leaders will need to overcome cognitive bias against an innovation deemed to be untraditional.
Acknowledgments
The Arbutus team in Canada and Kenya, colleagues at Imperial College Health Partners and the respondents and users at CoRSU-Uganda, Kenyatta National Hospital-Kenya and CURE-Kenya for providing first-hand feedback during our site visits 14-18 May 2017.
Footnotes
MP, IA and YB contributed equally.
Contributors All coauthors contributed equally to different aspects. of the study, including research, review and revision of paper. MP and IA conducted initial research. MP, AI and YB conducted field trip data collection. AD supported field trip and provided leadership and supported funding. IA wrote the first draft of case study. YB wrote the first draft of article followed by all coauthors. YB, MH and MP planned the overall study. YB was the principal investigator. MH was co-investigator.
Funding This research was funded by the UK National Institute for Health Research (NIHR) Biomedical Research Centre based at Imperial College Healthcare NHS Trust and Imperial College London.
Disclaimer The views expressed are those of the author(s) and not necessarily those of the UK National Health Service, the NIHR, the UK Department of Health or Arbutus Medical.
Competing interests None declared.
Patient consent Detail has been removed from this case description/these case descriptions to ensure anonymity. The editors and reviewers have seen the detailed information available and are satisfied that the information backs up the case the authors are making.
Provenance and peer review Not commissioned; externally peer reviewed.
Collaborators Imperial College Health Partners: George Garrad, Amy Darlington and Axel Heitmueller; Arbutus Medical: Florin Gheorghe.