Article Text

Statistics from Altmetric.com
Summary box
What are the new findings?
We describe a novel instrument that permits a rapid and safe minor salivary gland biopsy in cases of suspected Sjögren’s syndrome or other diseases.
How might it impact on healthcare in the future?
Minor salivary gland biopsy can be performed by a single person
The intervention is less invasive and more rapid
No neurological complications such as numbness were observed
Introduction
Sjögren’s syndrome (SS) is a chronic autoimmune condition with a prevalence of up to 1%.1 Salivary gland biopsy showing focal lymphocytic sialadenitis (focus score of ≥1) is required to fulfil the classification criteria for SS in seronegative patients, which is the case in up to 30%.2 Salivary gland biopsy is also an important tool to diagnose or exclude other systemic diseases causing sicca symptoms, such as sarcoidosis, amyloidosis, Mikulicz’s disease or IgG4-related disease. So far, there has been no standard technique for salivary gland biopsy. Minor salivary gland biopsy (MSGB) of the lower lip is widely used due to its low invasiveness, and has a sensitivity ranging from 63% to 93% and a specificity of >90% reported in most studies.3 In contrast to biopsy of the parotid gland, fascial nerve damage does not occur in MSGB. Yet it can lead to transient local paraesthesia of the lower lip in up to 11% of the interventions, at least when including different techniques regarding length and direction of incision or punch biopsy.4 Newer, less invasive techniques applying transcutaneous pressure manually or using devices such as adapted chalazion forceps5 reduce permanent neurological complications to 0.1%.6 7 In a study, using a needle tip for vertical mucosal incision and dissection of the glands along with pressure applied from the sides by the operator showed better results than the more invasive elliptic incision.8
MSGB is commonly performed by two operators, one providing assistance to hold the lip with or without pressure and the main operator performing local anaesthesia, mucosal incision and extraction of the glands. In this retrospective study we characterise the use of a novel disposable device to facilitate MSGB in routine practice.
Methods
We retrospectively studied 28 consecutive adult patients with clinically suspected SS who underwent MSGB using Saliclick (Curmed, Switzerland) between August 2018 and March 2020. We also studied 22 patients who underwent MSGB during this period without the device. In this case, transcutaneous pressure was performed by a second person after receiving instructions.
The clamp is a single-use device produced by three-dimensional printing and injection moulding subsequently. The technical use of the device is described in the Results section. We recorded the demographics of the patients, the side of the biopsy, the number of incisions, sample surface and the number of lobuli when possible. We also assessed if the quality of the sample was sufficiently useful for clinical decision making. We noted any use of stitches and any occurrence of complication, notably transient or persistent numbness, bleeding or infection.
Results
Procedure
Local anaesthesia of the lower lip was performed in all cases before the intervention. Figure 1 shows the device in the form of a disposable two-leg clamp with teeth-row sparing concave distal ends to be placed on the lower lip. A stamp is located on the lower leg with an opposite notch. A locking mechanism is situated in the middle of the device to allow application of constant transcutaneous pressure on the lower lip. In all 28 interventions the clamp was locked in the first grid with acceptable pressure for the patients and with sufficient pressure to provoke protrusion of the salivary glands after incision. The procedure is shown step by step in figure 2. A video of a representative procedure is seen in the following link: https://vimeo.com/chuv/review/436329329/644f692d5e.
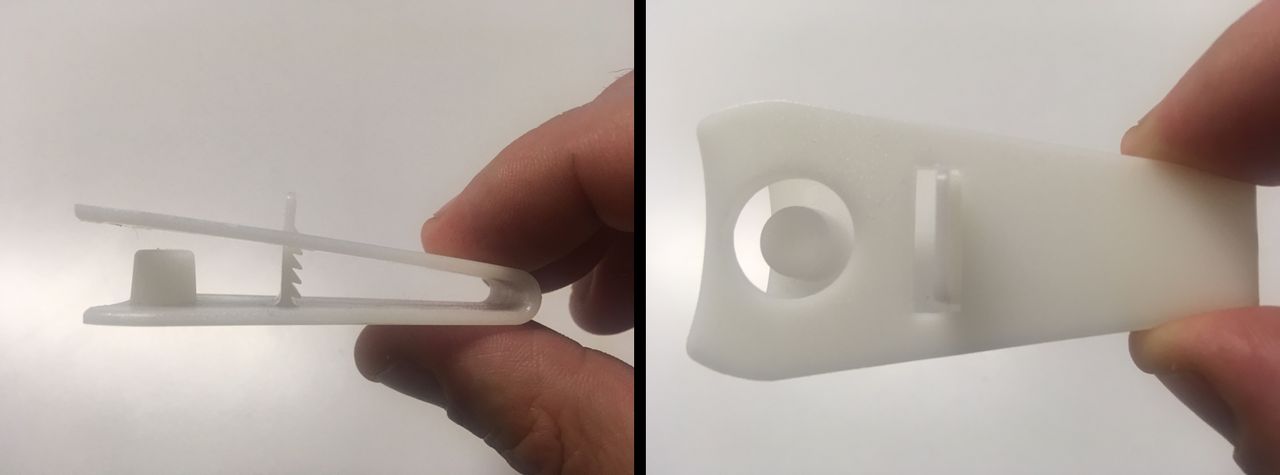
Saliclick lip holder.
{kind=link}
{kind=link}
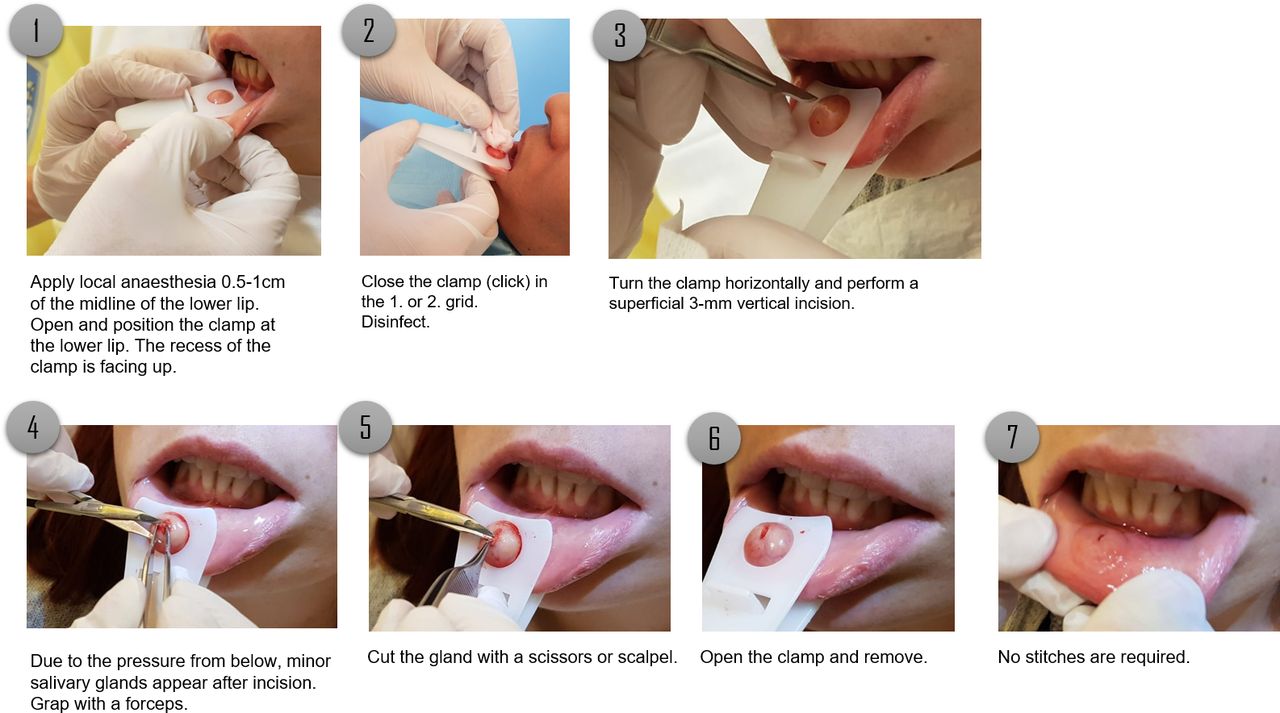
Step-by-step procedure of minor salivary gland biopsy using the Saliclick lip holder.
Outcomes
MSGB was performed by two operators (AD, TH). The characteristics and procedure outcomes of patients who underwent MSGB using the device are summarised in table 1. All MSGB procedures were performed during a 30 min routine clinic slot in outpatient clinic boxes. All MSGB procedures were performed by the operator alone without assistance. The mean sample surface was 4.4 mm2. For three patients, no glands were obtained on the first incision. The biopsy was repeated on the contralateral side with success in all three cases. In 89% of the cases the biopsy was conclusive and useful in the diagnosis or exclusion of SS. Alternative diagnoses such as amyloidosis or sarcoidosis were not reported. Complications occurred in two patients; one patient fainted, and the procedure had to be suspended for several minutes and resumed afterwards. Local haematoma was observed in the second patient. No neurological complications occurred; notably no hypoesthesia (or numbness) was reported. We found no difference between the intervention group using the clamp and the control group with an assisting person in terms of size. In the control group, one patient fainted and the procedure has been temporarily suspended.
Patient characteristics and technical outcome after MSGB using the clamp
Discussion
MSGB is a cornerstone in the diagnosis of SS. In this study we showed that a novel, self-locking clamp with a stamp can be used to perform MSGB safely and rapidly by a single person and thus is feasible to be integrated into a normal clinical consultation. Tissue yield and pathological assessment were comparable with results from other studies.6 We experienced mild haematoma in one patient, but notably no transitory or persistent numbness of the lower lip. We postulate that by transcutaneous pressure, incisions are more superficial than in other techniques, particularly as compared with punch biopsy. The duration of the procedure was not longer using the device when compared with the standard procedure including an assisting person, and yielded a similar number of glands. We observed less frequent bleeding during the procedure with the device compared with the standard procedure, even with patients under antiplatelet agents, and we postulate a haemostatic effect of the clamp through the applied pressure. Despite the technical advance in salivary gland biopsy, recent articles indicate that patients with SS may have negative biopsy results.9 Of note, other clinical criteria including ocular symptoms must be present in SS and should be investigated thoroughly. The recommendations for standardisation of labial salivary gland histopathology in clinical trials propose assessment of at least four labial salivary glands, with a surface of at least 8 mm2.10 Given the mean surface of 4.4 mm2 obtained in this study, at least two mucosal incisions are necessary if this device is used for clinical trials. In patients with suspected Mikulicz’s disease or lymphoma, submandibular gland biopsy has shown a higher diagnostic utility than MSGB and might be preferable.11
In conclusion we observed that the use of this device allows performance of MSGB without assistance, has good-quality outcomes and is not associated with neurological complication due to low invasiveness.
Footnotes
Contributors TH: development of the clamp, study design, biopsy and analysis, performance of biopsy, manuscript preparation. AD, BB, FK, JA-T: study design and analysis, performance of biopsy, manuscript preparation.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests TH developed the instrument and receives royalties.
Provenance and peer review Not commissioned; externally peer reviewed.