Article Text

Abstract
Despite the benefits derived from the use of assistive technologies (AT), some parts of the world have minimal or no access to AT. In many low-income and middle-income countries (LMIC), only 5–15% of people who require AT have access to them. Rapid demographic changes will exacerbate this situation as populations over 60 years of age, as well as functional limitations among older populations, in LMIC are expected to be higher than in high-income countries in the coming years. Given both these trends, AT are likely to be in high demand and provide many benefits to respond to challenges related to healthy and productive ageing. Multiple databases were searched for English literature. Three groups of keywords were combined: those relating to AT, ageing population and LMIC selected for this study, namely Brazil, Cambodia, Egypt, India, Turkey and Zimbabwe. These countries are expected to see the most rapid growth in the 65 and above population in the coming years. Results indicate that all countries had AT designed for older adults with existing impairment and disability, but had limited AT that are designed to prevent impairment and disability among older adults who do not currently have any disabilities. All countries have ratified the UN Convention on the Rights of Persons with Disabilities. The findings conclude that AT for ageing populations have received some attention in LMIC as attested by the limited literature results. Analysis of review findings indicate the need for a comprehensive, integrated health and social system approach to increase the current availability of AT for ageing populations in LMIC. These would entail, yet not be limited to, work on: (1) promoting initiatives for low-cost AT; (2) awareness raising and capacity building on AT; (3) bridging the gap between AT policy and practice; and (4) fostering targeted research on AT.
- Assistive Technology
- Geriatrics
- Global Health
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Background
According to the United Nations Department of Economic and Social Affairs’ World Population Prospects, Brazil, Cambodia, Egypt, India, Turkey and Zimbabwe, are expected to see a rapid growth in the 65 and above population in the coming years (see online supplementary appendix A, table 1). Among low-income and middle-income countries (LMIC), Brazil, Cambodia, Egypt, India, and Turkey are expected to have the highest growth in 65 and above age group by the year 2050 and 2100 within each WHO region (see online supplementary appendix A, table 2).1 Zimbabwe, on the other hand, is expected to have the second highest growth among the LMIC in the WHO Region for Africa (AFRO) by 2050 and third highest by 2100 (see online supplementary appendix A, table 2).1 In addition to rapidly ageing populations, functional limitations (activity and participation restrictions) due to impairment and disability among older populations in LMIC are expected to be much higher than in high-income countries (HIC). Impairment is defined by the International Classification of Functioning, Disability and Health (ICF) as any loss or abnormality of psychological, physiological or anatomical structure or function.2 Disability is defined by the ICF as any restriction or lack (resulting from an impairment) of ability to perform an activity in the manner or within the range considered normal for a human being. With increasing age, older adults are more likely to experience impairment and disability that increase activity limitations where they may face difficulties in executing activities, and participation restrictions where they cannot become involved in social activities.2
For cognitive-related functional limitations, according to the World Alzheimer Report 2010, the growth in number of people with dementia in low-income countries is expected to increase from ∼35 million in 2010 to ∼115 million by 2050, compared to HIC where the increase is expected to be from ∼15 million in 2010 to close to ∼35 million by 2050.3 In 2012, years lived with disability (YLDs) due to falls in adults aged 50–69 in developing countries (66%) was nearly double the rate in developed countries (34%).4 Falls have been documented as a key health concern leading to YLDs that older adults are facing today, and occur at home, in institutions and in the community.5
AT are defined as “the application of organized knowledge and skills, procedures and systems related to provision of assistive products, whose primary purpose is to maintain or improve an individual's functioning and independence, facilitate participation, and enhance overall well-being and quality of life.”6 AT provide significant support and benefits for older adults in various ways: safety and prevention (ie, prevention of falls), mobility and independence, social connectivity and ease of living, preservation of cognitive abilities, delay in depression, decline in functional loss and improved well-being and quality of life.7–13 Safety has consistently been identified as one of the most important reasons for the use of AT among older adults.8 ,10 According to Heywood et al10 home adaptations have reported a 70% increase in feeling safe at home among older adults, while adaptations such as grab rails and handrails have been found to produce lasting positive consequences. A systematic review by Chase et al14 found that AT, home modifications, along with other interventions prevented falls among community-dwelling older adults. Evidence from the current literature suggest that more than half (62%) of older adults felt safer from a risk of an accident with the availability of even minor adaptations.7 According to a study published by the AARP Foundation in the United States of America (USA), home safety devices made the majority of older adults feel safer (85%) and gave them peace of mind (78%).7
The definition of AT used in this review includes all the external technologies or products that are designed for and used by older adults. These technologies may assist in carrying out actions (ie, walking, bathing, remembering to take medications) and/or prevent severe health outcomes such as falls and injuries that may lead to more complicated health problems. There is a vast range of AT; according to the WHO, most of these products can be divided into several classes (table 1).6
Classes of AT
AT are a fundamental part of broader, integrated health and social system solutions to supporting older adults. Yet, despite the documented benefits of AT, some parts of the world have minimal or no access to AT that are designed for older adults. According to the WHO, in many LMIC, only 5–15% of people who require AT have access to them.15 LMIC are expected to experience the most rapid and dramatic demographic change, in shortened timeframes as compared to higher income countries. For example, it took more than 100 years for the share of France's population aged 65 or older to double from 7% to 14%,16 whereby it has been estimated that countries like Brazil will take less than 25 years to reach the same threshold.16 With rapidly ageing populations, accompanied by increasing functional limitations, in LMIC, AT are likely to be in higher demand.
Given the trends in LMICs, this review investigated the currently available AT, existing enabling legislation for provision of AT, and initiatives that promote AT for older adults in Brazil, Cambodia, Egypt, India, Turkey and Zimbabwe. The objective is to explore in the published literature, if currently available AT and existing legislation related to AT-provision are sufficient to support ‘ageing in place’ rather than ageing in institutionalised care homes; facilitate better health for older adults, especially in terms of functioning and independence (ie, carrying out Activities of Daily Living or ADLs and Instrumental Activities of Daily Living (IADLs)); encourage inclusion and full participation in community activities; and enhance older adults’ overall well-being and quality of life.
Methods
Data sources and search strategy
A systematic approach was taken to conduct the systematic review. The search strategy aimed to retrieve literature in English language that focused on AT to assist older populations (60 and above) in Brazil, Cambodia, Egypt, India, Turkey and Zimbabwe. Databases searched were MEDLINE (1950 to week 1 July 2014), EMBASE (1980 to week 1 July 2014), Scopus (1966 to week 1 July 2014) and Cochrane Library (1996 to week 1 July 2014).
WHO regional indexes including African Index Medicus (AIM); the Eastern Mediterranean Region Library Network (EMLIBNET); Pan American Health Organization (PAHO) Library Institutional Memory Database; Europe (EURO) publications; Index Medicus for South-East Asia Region (IMSEAR); WHO/WPRO Library; Western Pacific Region Index Medicus (WPRIM); and the WHO Library Database (WHOLIS) using the WHO Global Health Library platform were searched for relevant publications.
Three groups of keywords were combined: those relating to AT, ageing population and selected LMICs. Search terms used in each database are shown in figure 1. All retrieved articles were initially reviewed by title and abstract to find potentially relevant papers. Those papers were reviewed to obtain articles that met the inclusion criteria. Reference lists of articles that met the inclusion criteria were reviewed to identify any further relevant papers.

Search terms used in each database.
Study selection-Inclusion criteria
Selected papers were assessed against the following inclusion criteria: (1) studies published in academic and peer-reviewed journals, research reports, government reports (2) studies answered ‘yes’ to all three screening questions (3) written in English.
Screening Questions:
Does the publication address AT as a primary research topic?
Does the publication focus on one of the six countries?
Does the sample size or intended population include older adults (≥60 years old)?
Study selection-exclusion criteria
If the abstract indicated that the study did not relate to AT for ageing populations in LMICs, the study was excluded (ie, material relating to disability studies involving only younger people). Studies that focused on the technology use in hospitals were excluded, since the rationale of the systematic review is to focus on AT that have a direct impact on older adults to enhance their ADLs and participation in the community and at home. Duplicates were excluded (figure 2).
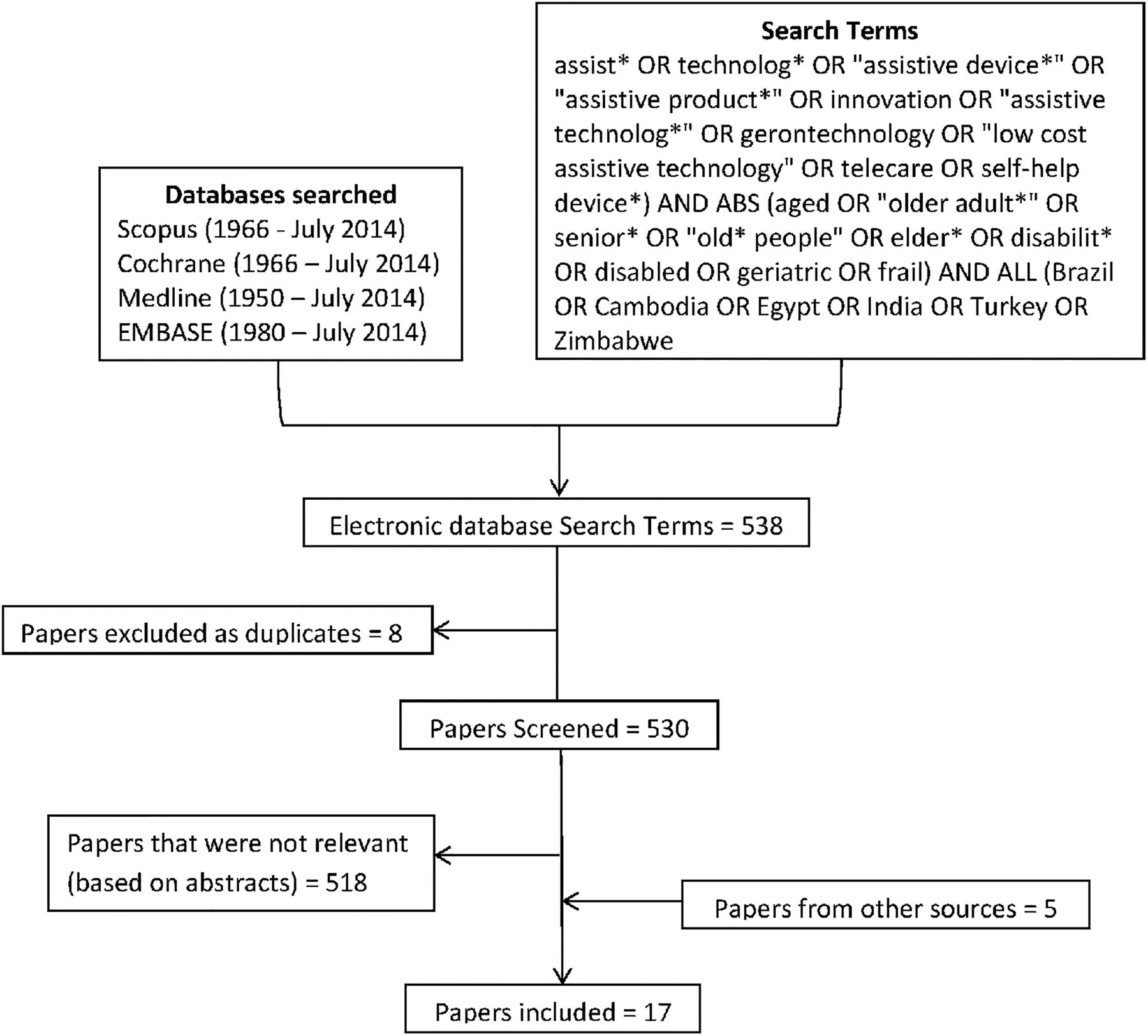
Literature search.
Results
The systematic review retrieved 17 relevant studies; four studies related to AT in Brazil, seven related to India, three related to Turkey and one study per each country for Cambodia, Egypt and Zimbabwe (figure 3). Seven publications focused on ‘mobility’ AT while six on ‘more than one function’; and AT for cognitive functions, ADLs, vision and others had one citation each (figure 4). Relevant studies are classified into four types as provided in table 2 below. Tables 3–5,17–33 provide an overview of relevant studies, existing enabling legislation and findings on AT for each country, respectively.
Study classification
Table of Evidence
Overview of legislation/national plans/policies and acts
Findings on AT availability by country (cited at least once in publications)

Number of publications retrieved by country.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Number of publications by assistive technologies category.
AT- related National Initiatives Brazil
The Assistive Technology Innovation Programme (PITA) finances technological development and innovation of products, processes and services targeted at people with disabilities, older adults and as well as others with difficulties of mobility.49 A budget of US$70 million is anticipated for this programme until 2014 directed to ‘innovation activities’ carried out by companies, universities and research institutions. Innovation activities include development and/or enhancement of products, processes and services related to AT and/or contribution toward prevention, alleviation or elimination of deficiencies.49
Future plans include the establishment of the National Centre for Excellence in Adaptive Technology, composed of 20 research centres implemented in public universities to develop strategic technologies, with an emphasis on prevention, rehabilitation and accessibility. The programme launched a virtual catalogue of more than 1200 AT products available in Brazil (http://assistiva.mct.gov.br).34 The website is to be updated at least once a year, so consumers and professionals are aware of availability of AT products in the country.34
Cambodia
Phnom Penh's National Component Factory is the only source of Prosthetic and Orthotic (P&O) devices in the country. It monitors and evaluates the production of prosthetics and AT materials, in order to supply for workshops and centres that produce P&O.50 They supply close to 15 000 those in need a year. Since January 2009, Phnom Penh's National Component Factory has produced and supplied more than 3000 artificial limbs, knee joints and alignment systems to physical rehabilitation centres in the country, free of charge.51
A number of workshops are available to provide prostheses, wheelchairs and crutches, repair and maintenance services in Cambodia, where each workshop is operated in partnership between the Government and NGOs. Currently 21 workshops provide AT for people with locomotor disabilities. Some of the workshops are run by numerous associations, committees and organisations. Online supplementary appendix E provides an overview of the associations and services provided.
Egypt
In Egypt, non-governmental organisations (NGOs) such as the Egyptian Society for Elderly Care and Misr al-Kheir provide assistance in acquisition of ATs such as canes and wheelchairs.48 The Arabic Doctors’ Union (an NGO) provides hearing aids and cochlear implants to those of age 65 and above while the Egyptian Society for Hearing Impaired Persons is responsible for provision and training the use and maintenance of hearing aids.48 Furthermore, Wafaa and Amal48 compound established and run by the Egyptian Veterans Association includes an assistive device factory for manufacture, maintenance and some export of devices for disabled individuals and veterans, where majority are older adults.
The government contributes to the provision of AT through the development, production, distribution, maintenance and repair. The government also provides prostheses/orthoses, wheelchairs, crutches, hearing devices and visual devices.52 In addition, the Ministry of Health and the Ministry of Social Solidarity provide healthcare and rehabilitation services, including technical aids and devices through their institutions. Ministry of Social Affairs provides services such as physiotherapy, prosthesis and assistive devices and rehabilitation.
India
The Artificial Limb Manufacturing Company (ALIMCO), fully supported by the Government of India's Ministry of Welfare, manufactures a large number of tools, machines and components for producing AT and finished devices. So far, ALIMCO has provided AT to 4.2 million users in India and serves approximately 200 000 users annually. ALIMCO also provides AT to Afghanistan, Nepal and Bhutan among others.53
The Indian Drugs and Pharmaceuticals Ltd. is the only other Indian company that manufactures components for AT in large numbers.54 In addition, there are at least 15 agencies producing wheelchairs and 20 producing tricycles.54 The most commonly produced are hearing aids, by as many as 32 manufacturing agencies mainly in the private sector.54
Most of the time, AT are distributed through NGOs, district rehabilitation centres, medical colleges and hospitals, special schools and camps and national institutions in India. NGOs and government supported institutions have spread over 19 states and union territories, which are financially supported under the ADIP Scheme run by the Government's Ministry of Welfare.54 The Department of Rural Development is involved in distribution efforts, and some NGOs not supported by the government also give out assistive devices. As many as 25 out of 31 states and union territories have their own schemes of providing AT through government hospitals and voluntary agencies.54 Many district rehabilitation centres also provide AT in the rural areas of specified regions.
The Government of India launched the scheme of Science and Technology—Project in Mission Mode 1988, to provide suitable and cost-effective aids and appliances and improve mobility.54 The project concentrated on developing cost-effective technologies and appliances and guiding these to large-scale use. Furthermore, there are initiatives to encourage proposals, research and development of technological solutions for older adults. One such example is the Initiative on Science and Technology Interventions 2010 for the elderly population, introduced by the Department of Science and Technology, under Science for Equity, Empowerment and Development Division (SEED). The initiative included a number of valuable indicatives (see online supplementary Appendix F).55
Turkey
No further initiatives were found.
Zimbabwe
No further initiatives were found. However, assistive devices and equipment for persons with disabilities are partially financed by Government Ministries, persons with disabilities and NGOs. The Government of Zimbabwe is involved in the provision of assistive devices, and provides prostheses/orthoses, wheelchairs, crutches and hearing devices.56
Discussion
The systematic review found that AT designed for older adults, have received some attention in LMIC. The publications (n=17) retrieved, heavily focused on products that assisted older adults with existing impairment and disability and only a few projects17 ,20 ,22 ,24 ,30 focused on AT designed for preventing impairment and disability among older adults (ie, fall preventive devices or smart home technologies). While existing disability related AT (eg, prosthetics, orthotics) are somewhat available in LMIC, other products designed to prevent impairment, disability and other health outcomes among older adults have received minimal attention, putting aside the needs of older adults who do not have existing disabilities but are at risk for developing impairment and disability due to increasing age, who would otherwise benefit from AT. Therefore, AT for the entire ageing populations including older adults with disabilities and older adults without existing disabilities but are at high risk for impairment and disability, such as those who are living alone at home, are necessary.
Based on the country-level findings and an overall analysis of all materials gathered for this systematic review, a set of high-level findings are presented and discussed below that could be considered as broad action points in moving forward with the relevant agenda on AT for ageing populations in LMIC.
Promoting initiatives for low-cost AT
In many LMIC, production of AT is low; where access might be possible, costs are excessive.15 ,20 However, this systematic review found that of those LMIC that have AT initiatives in place, typically for disabled populations, many have started the production of low-cost AT (ie, Brazil, Cambodia, Egypt and India). In Cambodia, the majority of the technological solutions provided included low-cost or even, no-cost AT, which are produced by using locally available materials and designs.50 The construction of low-cost equipment in Brazil is a model example, where production cost of devices was 30% lower compared with the cost of imported equipment.20 In the past 5 years, Assistive Technology Centers in Brazil have been developing AT similar to the commercial products, but with use of low-cost material and price reduction of up to 70% (see online supplementary appendix G, table 6).34 Strategies such as producing low-cost products by using locally available materials increase potential for continuous growth and demand for AT and allow for mass production to all those needing them. It is one of the most suitable strategies for LMIC, and highly recommended for resource-poor contexts.57 Mass production can lower costs if the technologies follow universal design principles and are marketed widely. ALIMCO in India is an example where large amount of AT are produced and marketed internationally.53 In the countries that have large production, markets should be expanded beyond regional boundaries to allow for cost advantages, operational efficiency and lower variable costs. In particular, there is a priority need for producers of AT to tailor design, distribution and cost to the realities and demand of older adults.
In terms of production, many LMIC produced AT locally. Cambodia and India produce a considerable number of AT and components for AT with materials indigenous in these countries. This may be partly explained by the fact that the production workshops or companies themselves are partially or fully supported by or working in partnership with the government. Providing funds for local workshops such as the Egyptian Fund for Supporting Small Industries,48 further encourages local production. Manufacturing or assembling products locally, using local materials, can ensure that devices are suitable for the context.58 It may either be a locally produced, finished product or locally assembled products with imported materials. Where local production is not sustainable, reducing import and duty taxes on AT devices or components can help reduce costs. For example, Brazil does not impose import or duty taxes on imported materials,59 Turkey has exemptions for imported goods and partial exemptions for selected equipment, and Zimbabwe also allows for exemption from paying import tax for some equipment produced for older adults and disabled citizens.45 Therefore, local production and reduction of taxes, where import is required, are appropriate strategies that governments can acknowledge and support.
Awareness raising and capacity building on AT
Producing and providing AT in and of themselves is not adequate. Significantly fewer AT users in rural areas receive guidance and instructions on the use of AT, and only a few older adults are aware of the existing AT and their benefits in LMIC. For example, a major constraint to the availability of AT in India has been partly the lack of awareness among the users and professionals.24 Even if schemes are available to provide free or subsidised AT, unless users and professionals are aware of their existence and benefits, AT will not be able to prove their worth and purposes. Therefore, information sharing, awareness raising and training are all crucial for successful implementation and usability of AT. In addition, difficulty of use is one of the major reasons for disuse of AT among older adults.60 Our review found that provision of community-based skills programmes has increased total performance and sense of security with the devices to a greater extent among older adults (ie, wheelchairs) in Turkey.32 Hence, the provision of training along with guidance and instruction on the use of AT will reduce the hesitancy to use AT among older adults.
Adequately trained professionals are also an important part of successful implementations and use of AT. Many developing countries including Brazil, India and Zimbabwe58 are lacking occupational therapist (OT) and physical therapists (PT) mainly due to lower pay scales and lack of college or university training programmes. AT must be ensured to be appropriate, adaptable and high quality before distributing to older adults. They must suit the environment and the user and include adequate follow-up in order to ensure safety and efficient use. Especially when countries receive AT as donations from HIC, they need to be assured for quality and safety. For example In Egypt, a highlighted concern is that AT are largely inappropriate, and that there are no quality standards or criteria for monitoring of these services.61 Therefore, implementing policies and programmes for training professionals to assess, provide and promote AT are relevant approaches to successfully providing AT to older adults in LMIC. Furthermore, while training OT and PT, it is important to include other experts in the field such as geriatricians to foster a multidisciplinary team approach in order to provide appropriate technologies and services. Standards and guidelines on provision, development, production and distribution of AT in LMIC must be addressed with the input of experts in the field in collaboration with other countries.
Bridging the gap between AT policy and practice for older adults
The review findings point to the existing gap between legislation and practice. Examples (table 4) were found with some legislation and policies, but whether they have resulted in significant improvement in provision of AT for all older adults in practice is unclear. This is partly due to lack of documentation or lack of evidence available in the literature. Countries that have absolutely no legislation could possibly start with ratifying the UN-CRPD. Countries that have ratified the UN-CRPD and have legislation in place could make amendments and adopt new legislation that is more focused on improving function and well-being of older adults.
Most often, planning for and responding to health and social needs of older adults falls under either the Ministry of Social Solidarity and/or Ministry of Health, under umbrella terms such as ‘disabled care’ or ‘family care’ or ‘family medicine’ (ie, in Egypt).48 This partly explains the fewer existing legislation that focus on providing AT for older adults. Legislation tends to be specific to a population group (such as the disabled), or to specific health technologies, but rarely linking the two. There is thus, a need to help countries further develop legislation that supports both production and financing of AT along with their integration with health and social services, and in particular for older adult's functional and cognitive needs.
Fostering targeted research on AT
An interesting finding of this review that offers opportunities for further research is that AT for mobility, especially canes, were the most commonly used with the least difficulty in usability among older adults. It may be explained, in part, that canes are an inexpensive, versatile and light weight mobility option that are well suited for LMIC contexts. Production costs are low and products can be made by material readily available such as wood; hence may be among the most appropriate AT in LMIC. While mobility aids provide assistance, support, strength and balance and also prevent falls, some studies5 ,62 have reported that mobility aids such as canes could also cause falls. Therefore, additional research is required to understand the mechanisms leading to negative consequences, as well as to better design AT and identify use and environmental measures to prevent such negative consequences along with maximising appropriateness of different AT.
The review also found that benefits of AT are rated high and disadvantages low among older adults.21 As seen in the Cambodian study,21 availability of AT to fulfil ADL have increased self-reliance and contribution to the community by physically vulnerable older adults. Improvement in social status, self-esteem, not being a burden to others, improved well-being and economic situation are among the achieved benefits of AT. Whether older adults consider AT as beneficial or not beneficial in LMIC is an important precondition for successful implementations of AT. Therefore, attitudes, aspirations and demands towards technology contribute to their usefulness and usability and perceived advantages among the users, and must be explored further prior to supplying AT to older adults.
Another observation from the review is that of the countries that had available AT, such AT were found to be suitable for the local population. For example, in Cambodia, the most common AT were different forms of seating, which enabled individuals to sit comfortably and bathe from a water source. In Cambodia, it is traditional to bathe by scooping water from a source, using a household cup or bowl and pouring it over the body. Similarly, in Turkey, walking sticks carry traditional importance in some regions, and these were one of the most used mobility aids in Turkey. When introducing AT to LMIC settings, it is important to take into account traditional and cultural values and provide AT that are likely to be accepted by the targeted population. Social acceptability of AT contributes to the usability of devices and avoids development of devices that may be stigmatised in the society. When there is more social acceptability, users are more likely to use their devices.
In addition, in future research, education and action on innovation, AT require to be seen differently, which is as highly useful products and devices that support older adults with existing impairment and disability, and as a way to prevent severe health outcomes among older adults who do not yet have disabilities.
Limitations
The systematic review retrieved a limited number of relevant publications published in peer-reviewed journals, for each country, in English. This can be partly explained by the limited research in the field of AT, especially in LMIC. In many LMIC, numerous other health issues (eg, treatment of communicable and non-communicable diseases; health insecurity) are considered as pressing priorities. Only recently did AT for older adults are becoming a health priority consideration for LMIC. At the same time, there are a number of barriers that keep LMIC from having ready access to affordable technologies. These include cost, limited funding, lack of awareness on existing AT and their benefits, cultural perceptions (or misperceptions), inappropriate environmental conditions, heterogeneity of older adults terms of functional limitations and comorbidities and a limited number of trained practitioners to train individuals on the use of AT.19 ,48 Lack of research conducted on the subject in resource-poor contexts strongly emphasises the need for more research on AT for older adults in LMIC.
Another limitation is that the search was limited to English language. It is possible that many countries have some research published in different languages. For example, in the case of Egypt, most documents could have been published in Arabic and not translated to English, which is possibly a reason for the lack of evidence available on Egypt. Similarly with Brazil, the authors came across material that was not published in English. Additional limitations may include those related to lack of consistency in the use of the AT terminology; and lack of awareness or knowledge base to date of the needs of older populations in the six study countries. Despite the limitations, the authors believe that the results are important and represent the most comprehensive information currently available on AT (in English) for older adults in these LMIC.
Conclusion and recommendation
AT for ageing populations have received some attention in LMIC. AT that assisted older adults with existing impairment and disability have received more attention than AT that are designed for preventing impairment and disability among older adults who are inevitably at a high risk for impairment and disability as a result of ageing. More systematic planning and efforts are required to design, produce and ensure the availability of affordable, acceptable, accessible and adaptable AT to support older adults in meeting specific functional and cognitive limitation needs of a rapidly growing ageing population in the midst of advancements in assistive technological innovations globally.
With rapidly increasing ageing populations in LMIC, as exemplified in the six countries selected for this review, AT for the entire ageing population including older adults with existing disabilities and without existing disabilities, but are at high risk for impairment and disability, are necessary with the support of national enabling legislation. Analysis of review findings indicate the need for a comprehensive, integrated health and social system approach to increase the current availability of AT for ageing populations in LMIC. These would entail, yet not be limited to, work on: (1) promoting initiatives for low-cost AT; (2) awareness raising and capacity building on AT; (3) bridging the gap between AT policy and practice; and (4) fostering targeted research on AT.
Acknowledgments
This systematic review was carried out in 2014 by the WHO Centre for Health Development, also known as the WHO Kobe Centre (WKC), scientific work stream to build the evidence base for Innovation for Healthy Ageing (IHA). The authors would like to thank the technical inputs, review and kind assistance of WHO/WKC colleagues, namely: Mr Loic Garçon, Technical Officer, WKC; Mr Amit Prasad, Technical Officer, WKC; Mr Paul Rosenberg, Technical Officer, WKC; Mr Chapal Khasnabis, Technical Officer, WHO HQ NMH/VIP/DAR; Dr Said Arnaout, Coordinator, Healthy Life Style Team, WHO Regional Office for the Eastern Mediterranean (WHO EMRO); Egyptian team from Ain Shams University—Dr Sarah Hamza, Dr Mostafa Manar, Dr Mousa Shereen, Dr Shawky Ahmed, Dr Rashidy Doha and Dr Hala Sakrha. They also would like to acknowledge and appreciate the support of other members of the IHA team, WKC.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online appendices
- Data supplement 2 - Online table
Footnotes
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.