Article Text

Abstract
The Social Innovation in Health Initiative (SIHI) piloted a community engagement self-monitoring (CE-SM) strategy, where communities were actively engaged in monitoring the implementation and performance of their social innovations to ensure that their objectives were achieved. This strategy aims to empower communities to document processes, understand the factors involved and measure outcomes by developing a community-grounded self-monitoring tool and implementing their own approach.
Two community comanaged social innovations were selected. For one innovation, the communities implemented the CE-SM independent of external intervention. For the second, the communities were provided with minimal assistance by SIHI. These communities identified their monitoring indicators and selected local monitors to collect data to assess performance outcomes and document the entire process.
Communities chose indicators based on their perceived importance and practicality, while monitors were chosen based on their familiarity with the community. Community leaders’ proactive leadership and community members’ participation contributed significantly to its success. The important role of regular feedback sessions was also emphasised, not only as a means of monitoring progress but also for boosting their morale. The level of external support needed by a community was determined by the scope of the project and the community’s grasp of the strategy.
CE-SM has been demonstrated to be a viable strategy when communities realise their capacity to monitor their own projects using an approach they deem fit. It has also enhanced their sense of ownership which could improve the chances of sustaining these initiatives and contribute to more accessible healthcare and services.
- Community Medicine
- Public Health
- Primary Healthcare
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Summary box
What are the new findings?
The project demonstrated a novel and inclusive method to codesign and coimplement monitoring and evaluation strategies for social innovations in health.
Regular feedback sessions of the local monitors served not only as a means of monitoring their progress but also as a means of boosting morale. Weekly sessions served as a ‘safe space,’ where local monitors were free to voice their insights and opinions.
When social innovations are conceptualised, cocreated and used by a community, there is a sense of ownership and a better grasp of their principles, making the implementation and monitoring process more efficient and meaningful at the community level.
How might it impact healthcare in the future?
Self-monitoring and evaluation of communities for social innovations in health can help these communities access data needed to improve and refine these innovations to further improve health outcomes in the community.
Empowering communities to implement self-monitoring and evaluation strategies for health initiatives in their communities can enhance their sense of ownership of these initiatives, which could improve the chances of sustaining these initiatives and contribute to more accessible healthcare and services.
Introduction
Social innovations in health (SIH), defined as a community-engaged process that links social change and health improvement, drawing on the diverse strengths of local individuals and institutions,1 are embedded in strengthened community engagement processes that promote people-centred health systems and equitable health services.2 They have been shown to enhance public health sector delivery capacity, prioritise impact, agility and sustainability, and produce outcomes that extend beyond health.3 These must therefore be scaled up, sustained and integrated into existing health systems.
Globally, community scorecards have been used as a participatory social accountability tool for planning, monitoring and evaluating services in health, education, water and sanitation.4 In the Philippines, scorecards are used as a means to evaluate and monitor the performance of local government units in the implementation of reforms within the health system.5 However, it largely uses a top-down approach with little involvement from the community. Hence, there is a need to explore community-grounded, community-managed and contextualised approaches to the monitoring and evaluation of health intervention performance and implementation. A similar strategy was adopted for the control of onchocerciasis in Africa, which was found to promote sustainability, community ownership and empowerment.6
In this regard, the Social Innovation in Health Initiative (SIHI) engaged selected communities in the Philippines to implement a community engagement self-monitoring (CE-SM) strategy with a focus on social innovations among urban and rural communities. This allows communities to be involved in the entire process of monitoring, where they can plan, design and implement how to monitor their projects as they deem fit. Enabling relationships among community stakeholders and partners to enhance existing practices in addressing health challenges specifically in monitoring and evaluation is deemed to be an effective approach to promote ownership and sustainability at the community level.7 8
Objective
To describe the processes and dynamics of the communities in implementing a community-grounded and contextualised CE-SM strategy for SIH, which will help identify factors and describe strategies to best engage communities. It also seeks to explore factors influencing the level of external support a community needs to conduct the strategy.
Methods
Key persons and their roles
The SIHI is a global network of individuals, organisations and institutions advocating for and advancing research in social innovation in health. The SIHI country hub in the Philippines (SIHI Philippines) conducted the project.
Innovators pertain to community-based organisations, represented by their heads, who have developed and implemented social innovation(s) to address identified priority health needs of Filipino communities.
Documenters are individuals that innovators have assigned to document how communities plan, collect, analyse and report data. They serve as observers and were not to intervene in the communities’ processes. Essentially, they are the community’s link to the SIHI team.
Local monitors refer to community-selected volunteers who are part of the community where the social innovation is being implemented. Their main task is to collect data throughout the self-monitoring process.
CE-SM implementers collectively refer to the innovators, local monitors, community members and community leaders who have been involved in the implementation of the strategy.
Overview of CE-SM strategy implementation
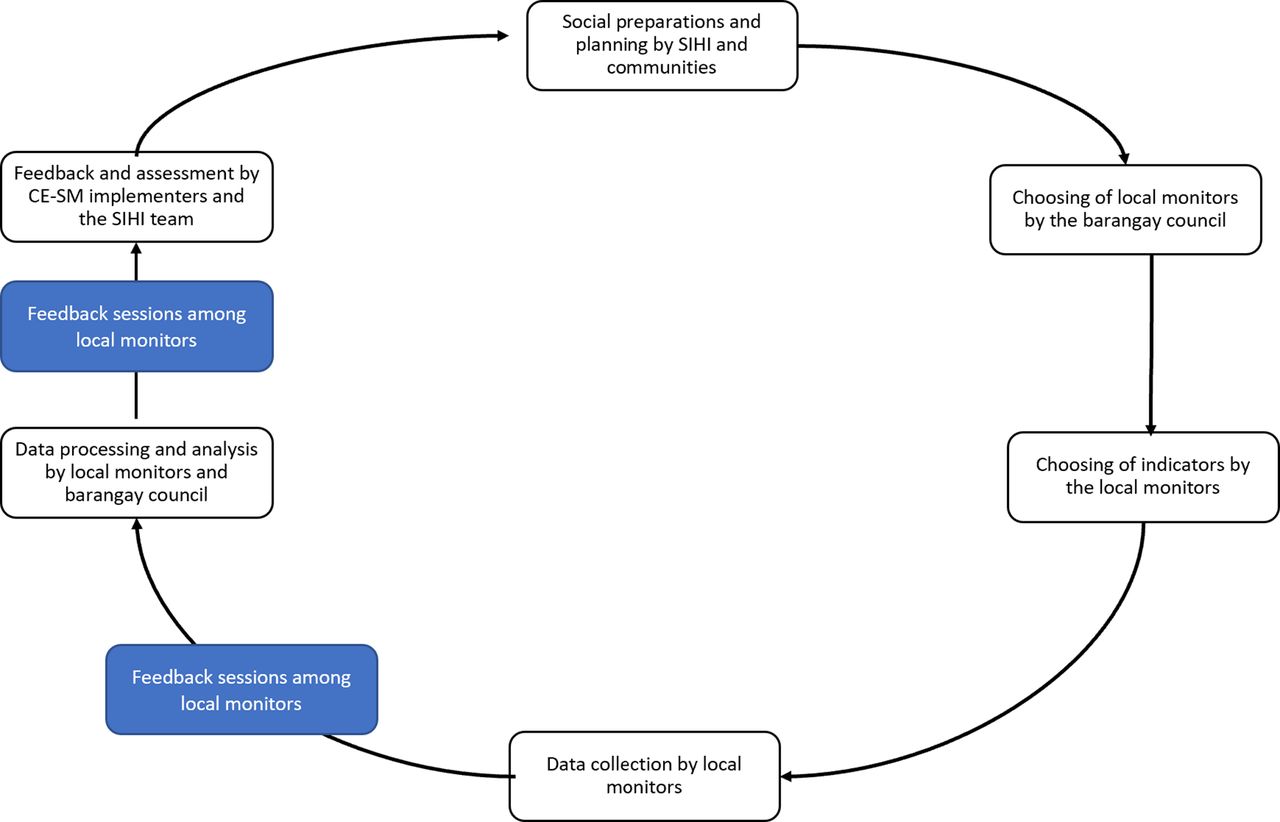
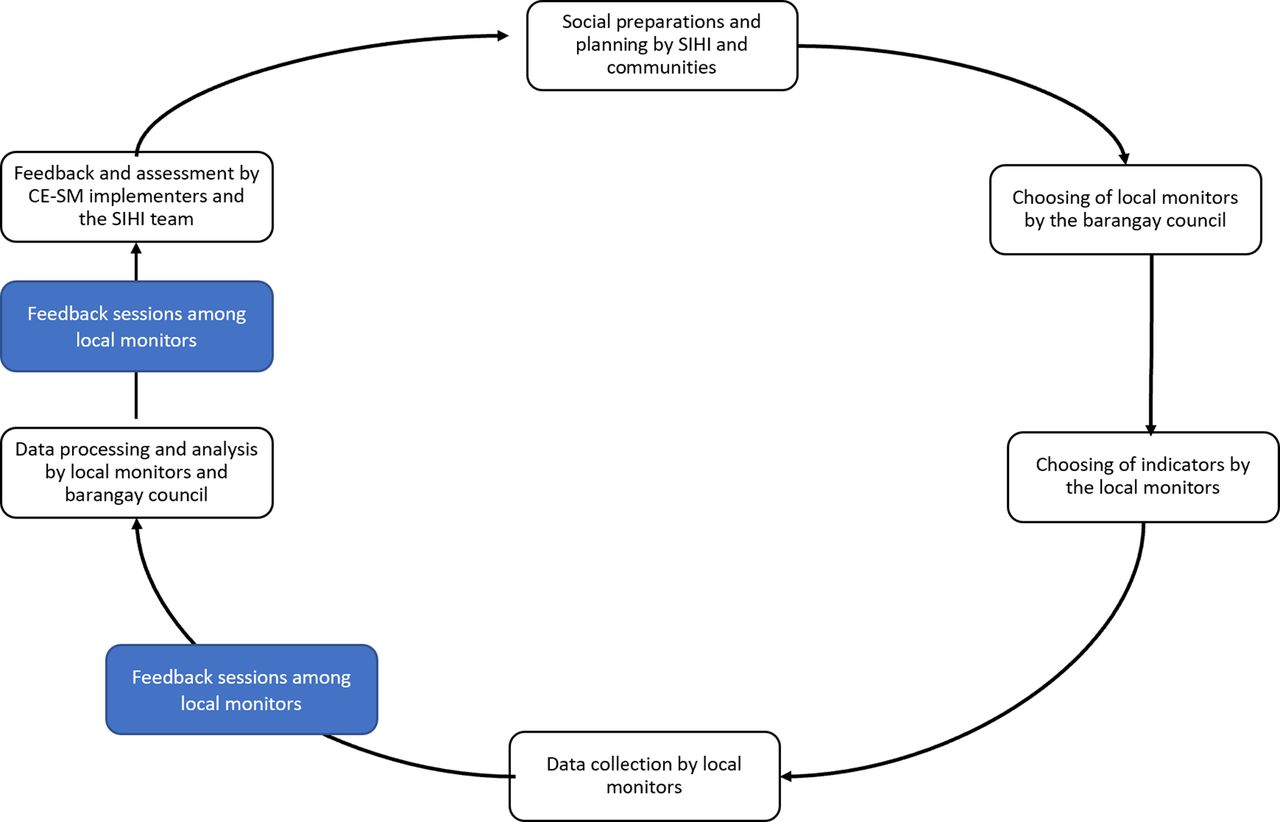
In the preparatory phase of CE-SM, SIHI conducted the selection of innovations and planning with the innovators, including the selection of specific communities to be engaged. This was followed by the identification of local monitors and the selection of monitoring indicators. The actual implementation of the monitoring process, documentation of community performance outcomes and reporting of feedback were then carried out by the communities(figure 1). These were conducted from September to December 2021.
{kind=link}
Steps in the implementation of the CE-SM strategy. CE-SM, community engagement self-monitoring .
Selecting social innovations
For the pilot implementation of the CE-SM strategy, the social innovations should be: (1) codesigned and (2) comanaged by the community or have a strong community participation component and (3) implemented within the time frame of the project. Innovations were chosen from those that were identified and recognised by SIHI Philippines for developing and implementing social innovation(s) based on the identified priority health needs of Filipino communities.9
Two social innovations were selected: (1) Kalinga Health of Innovations for Community Health,10 and (2) Seal of Health Governance (SOHG) of the municipality of Del Carmen, Surigao del Norte,11 as listed in table 1. A difference in the urban–rural setting of the innovations was also taken into consideration to explore differences in the strategy implementation (table 1). The CE-SM implementers for Kalinga Health were designated as the community-managed group, which did not receive any intervention from external partners. In contrast, the CE-SM implementers for SOHG were assigned as the SIHI comanaged group. They received minimal assistance from SIHI by being provided with an initial list of monitoring indicators but were able to modify this as they deem fit.
Profile of identified social innovations
In general, both innovators aimed to conduct monitoring to determine progress towards objectives and gain an understanding of the factors which serve to enable the innovation’s sustainability. For SOHG, which is a leadership programme with a monitoring component itself, CE-SM was geared towards determining if the objectives are being achieved and if such an initiative can be sustained. The indicators have then been selected based on what the local government unit and the community considered important for sustainability, specifically the community’s perception of and participation in the programme. Kalinga Health, on the other hand, was focused on increasing case detection and treatment compliance, as reflected by their indicators. It is important to note that ultimately, it was the local monitors who had the final say on what indicators to use and how to go about the strategy, in consultation with barangay leaders.
Planning sessions with innovators
The SIHI team conducted an orientation session, with the support of an expert in community engagement in global health, to facilitate an understanding of CE-SM, its value for social innovations and partners, and its specific implementation steps. SIHI’s definition of social innovation, the principles and dynamics of CE-SM, the importance of community engagement and the use of CE-SM results were discussed. It was an interactive session with the innovators, SIHI team and members of various SIHI country hubs.
Implementation of the CE-SM strategy by the communities
Kalinga Health first engaged K! Leaders, who helped distribute letters to all barangays to introduce the project, along with an invitation for a virtual meeting with barangay officials. Two barangays agreed to be part of the project. A series of sessions were subsequently conducted by Kalinga Health to orient chosen monitors on collecting, interpreting and reporting data. A special session was facilitated on collecting data from the online dashboard that Kalinga Health developed. During the 4-week implementation period, data were collected from the online dashboard once weekly.
For the monitoring of SOHG, an orientation led by the local government head was conducted in each barangay to reintroduce the innovation, introduce the CE-SM strategy, and discuss implementation with members of the barangay council, who are in charge of planning and implementing government programmes and passing resolutions and ordinances in the community. They participated in consultative sessions to select monitoring indicators and local monitors through votation. The chosen local monitors were assigned to conduct house-to-house visits and interview household representatives based on the assigned catchment areas using a questionnaire that they themselves devised. Paper-based monitoring was used. After collecting data, accomplished questionnaires were checked, consolidated and finalised by members of the council.
Feedback loops
The documenter for Kalinga Health held two virtual sessions with local monitors, where weekly data were reported, and difficulties were discussed. After the 4-week implementation, local monitors presented their findings during a feedback session. The documenter for SOHG had separate face-to-face meetings with the local monitors of all barangays to discuss difficulties encountered in collecting and analysing data.
The SIHI team conducted weekly meetings with the documenters to discuss the progress of the communities, the difficulties they encountered and recommendations to improve their approach. These meetings were crucial to identify barriers early and formulate timely solutions. To synthesise insights from the project, a joint assessment meeting was conducted at the end of the implementation period.
Results
Choosing local monitors
For Kalinga Health, K! Leaders were chosen as local monitors primarily because of their familiarity with the community and innovators. For SOHG, selected local monitors were mostly barangay health workers and barangay nutrition scholars because of their familiarity with the community and their perceived ability to execute required tasks. Barangay secretaries and treasurers were selected to spearhead data consolidation, while barangay captains and councillors acted as team leaders.
Choosing monitoring indicators
Monitoring indicators for both innovations were chosen based on what local monitors perceived as important, feasible and practical (see online supplemental appendix 1). For Kalinga Health, the two barangays came up with similar indicators, which include identifying the number of patients who have been: (1) diagnosed with tuberculosis, (2) lost to follow-up and (3) completed treatment in Kalinga Health. For SOHG, the majority of barangays opted to maintain the indicators provided by SIHI with two to three indicators per innovation objective, prioritised based on significance to their community and availability of data, as listed in table 2. The majority chose indicators that assessed the relevant involvement of stakeholders in the development, implementation and monitoring of the programme, the type and coverage of community-based initiatives, and the community’s perception of and response to the initiatives. These were translated into Filipino and the local language of the community.
Supplemental material
An excerpt of the monitoring indicators identified for SOHG
Dynamics of the monitoring process
Local leaders considered representation, active participation and cocreation as important factors in achieving the project’s goals. Moreover, the engagement and commitment of the community to the project were observed to be largely dependent on their perception and trust in its principles and objectives.
The frequency and timing of monitoring were dependent on the availability of the workforce and their timeline. Local monitors for Kalinga Health collected data weekly while those from SOHG monitored once for the entire duration of the project. The former noted ease in monitoring because of their access to an online dashboard, which the local monitors were trained to use. The latter opted to do monitoring only once because of the large number of households to cover within a limited time frame. It was also difficult to monitor more frequently because of other simultaneous community projects and commitments.
Challenges encountered
An initial challenge for the CE-SM implementation for Kalinga Health was establishing rapport with community members which necessitated the extension of the preimplementation period. The unfamiliarity of the barangay councils with Kalinga Health and restrictions set by the COVID-19 pandemic also contributed to this.
During data collection, the limited time to complete interviews and difficulty collecting relevant data due to the unavailability of household heads and initial confusion of respondents were identified as challenges by both SOHG and Kalinga Health.
During data processing, the lack of familiarity with technology such as softwares for encoding and poor internet connection posed difficulties for both communities. To remedy this, help was sought from teachers and the Sangguniang Kabataan (Youth Council) for the questionnaires and from rural health unit nurses and the Disaster Risk Reduction and Management team for the coordination of visits. Explaining and expounding on concepts provided understanding and valuable insights to the respondents. One remark of note was a respondent who said, ‘Sa tagal namin dito, ngayon lang kami natanong tungkol sa ganito’ (In the many years of living here, this is the first time someone asked for our thoughts about a project).
Discussion
Throughout the project, the political will of barangay leaders contributed significantly to its success. This is consistent with Arnstein’s take on engagement and how the relationship between power, community and government affects the decision-making power of the community.12 The importance of following the community’s timeline was also emphasised. A pre-existing relationship between community members and the project team members facilitated active participation and better working relationships. Good relationships were an enabling factor for better engagement, observed in both communities. Moreover, the important role of regular feedback sessions was emphasised, not only as a means of monitoring progress but also to boost their morale and sense of ownership. Weekly sessions served as a ‘safe space’ where local monitors were free to voice their insights and opinions. This facilitated a continuous people-centred approach in the implementation and improvement of initiatives and cocreation of more community innovations. The sense of ownership also leads to more efficient and meaningful implementation and monitoring which enables project sustainability, even when external funding and support decreases or ends. The focus of monitoring was dependent on the nature of the social innovations and was geared towards determining progress towards goals and exploring elements crucial for sustainability. This was determined through a synergistic approach with the social innovators. Throughout the process, strategies and factors to best engage communities were identified, including building rapport, tapping community leaders, explaining the purpose and importance of the project to the community members, and holding regular feedback sessions.
The study explored whether differences exist between communities receiving different levels of support from external sources for their implementation of the CE-SM strategy. For the monitoring of SOHG, SIHI provided support in the initial stage by providing a list of indicators. This was found to have a minimal effect on the process and outcomes. The community had difficulty providing information required by the monitoring indicators due to the unavailability and inaccessibility of data sources and lack of knowledge of the formulas needed to process data. On the other hand, the communities of Kalinga Health, which did not receive any form of support from SIHI, had no difficulty formulating indicators but had challenges moving forward, as they initially experienced difficulty in using the online dashboard. These demonstrate that the level of external support must be tailored to the baseline knowledge and skills of local monitors. Prior experience with the strategy and the availability of data sources are also some of the factors influencing the level of support needed. These might also indicate a mismatch between the perception of decision-makers of available community resources (financial and/or technical) and actual available resources. Levelling this could be important to future community self-monitoring programmes. Capacity-building activities focusing on creating questionnaires, building and understanding databases, and analysing data may also be beneficial.
Conclusion
The project discusses the community engagement and self-monitoring strategy, where communities are in charge of all phases of the strategy implementation. This is unique in that these efforts are community led, allowing them to change certain aspects of these processes as they deem fit. Other communities may benefit from it by contextualising the processes based on the specific problem being tackled and the actual circumstances of the community. Self-monitoring and evaluation of communities for social innovations in health can help these communities access data needed to improve and refine these innovations to further improve health outcomes in the community.
The results of the pilot implementation of the CE-SM strategy demonstrated that it is a viable approach when tailored to the capacity of the community, the nature of the project being implemented and its practicality and feasibility for the community. It further affirmed the pivotal role community engagement plays in motivating and empowering communities to actively participate in social innovations. Letting community members monitor their projects—from identifying monitoring indicators to collecting and analysing data, and finally using these to improve implementation and create more solutions to enhance health and quality of life—highlights the importance of developing a sense of ownership and partnership in ensuring the sustainability of an initiative, whether with the government or private sector.
Our study is exploratory in nature, hence the conclusions drawn from this study may not be applicable to other settings. The findings can be strengthened by exploring the strategy on a larger scale, with a longer timeline and in other sociocultural settings.
Ethics statements
Patient consent for publication
Acknowledgments
This study was conducted with the support of TDR, the Special Programme for Research and Training in Tropical Diseases. The authors would like to thank Hon. Alfredo Coro II, his team and the local monitors from the municipality of Del Carmen. We would also like to thank Ms. Gabrielle Larin, Mr. Reiner Tamayo, the rest of the Innovation for Community Health (ICH) team, and the local monitors from Marikina City for their valuable contribution to the study.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
ML and NJ are joint senior authors.
Twitter @janadeborahmd
Contributors UA, ML, NJ and BH conceptualised and designed the project. PMPT, JDM-A and JRBC designed and finalised the protocol. JE conducted the focus group discussions. PMPT, JDM-A, ML, JRBC, UA, JA and BH facilitated the qualitative analysis. All authors reviewed, edited and approved the final version of the manuscript. Deceased: NJ since deceased.
Funding The CE-SM project is conducted by the Social Innovation in Health Initiative (SIHI). It is funded by TDR, the Special Programme for Research and Training in Tropical Diseases cosponsored by UNICEF, UNDP, the World Bank and WHO. TDR is able to conduct its work thanks to the commitment and support from a variety of funders. For the full list of TDR donors, please see: https://www.who.int/tdr/about/funding/en/. TDR receives additional funding for SIHI from the Swedish International Development Cooperation Agency (Sida) to support SIHI. Grant/Award Number: N/A.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.