Article Text

Abstract
Background Social innovation in health is a community-engaged process that links social change and health improvement, drawing on the diverse strengths of local individuals and institutions. However, there are few studies that examine community engagement, financing and outcomes. The purpose of this study is to use a qualitative descriptive analysis to assess 40 social innovations in health identified through a global open call.
Methods This qualitative analysis examined social innovation case studies from low- and middle-income countries identified by a global social innovation network. A crowdsourcing open call identified projects and key components of each social innovation were evaluated by an independent panel. We used a US Centers for Disease Control and Prevention framework to measure community engagement as shared leadership, collaboration, involvement, consultation or informing. We used descriptive statistics to examine key aspects of community engagement, financing, health outcomes and non-health outcomes.
Results Data from 40 social innovations were examined. Social innovations were from Africa (21/40), Asia (11/40), and Latin America and the Caribbean (8/40). Community engagement was diverse and robust across the cases and 60% (24/40) had either shared leadership or collaboration. Financing for social innovation came from research grants (23), national or provincial government support (15), revenues from sales (13), donations (13) and local government support (10). Social innovations reported health and non-health outcomes.
Conclusion Our data demonstrate social innovations had robust community engagement. Innovative financing mechanisms provide mechanisms for sustaining social innovations. Further research on health and non-health outcomes of social innovation is needed.
- social work
- sociology, medical
- public health
Data availability statement
Data are available in a public, open access repository. All data are available and listed in the supplementary material.
This is an open access article distributed in accordance with the Creative Commons Attribution 4.0 Unported (CC BY 4.0) license, which permits others to copy, redistribute, remix, transform and build upon this work for any purpose, provided the original work is properly cited, a link to the licence is given, and indication of whether changes were made. See: https://creativecommons.org/licenses/by/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Social innovation in health suggests innovations may be more effective when organically emerging from local actors in partnership with community members.
Importance of community engagement has been recognized but more research and action on community engagement is needed to ensure sustainability.
WHAT THIS STUDY ADDS
Data suggests robust community engagement across the life of social innovations, with over half of the cases meeting criteria for shared leadership or collaboration.
Diverse funding sources support social innovations and these financing mechanisms enable the sustainability of social innovations.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE AND/OR POLICY
Community engagement is a critical component of social innovations which should be highlighted for programmatic and policy considerations.
Exceptional innovation opens space for the implementation of both health and non-health outcomes; further research is needed.
Introduction
Health systems and services remain largely implemented through an expert-driven, top-down process which often fails to recognise community engagement as a key feature of improving health and well-being. However, the field of social innovation in health suggests that innovation may be more effective when it organically emerges from local actors in partnership with community members, especially people in low- and middle-income countries (LMICs). Social innovation in health is a community-engaged process that links social change and health improvement, drawing on the diverse strengths of local individuals and institutions.1 Social innovation provides innovative solutions to address healthcare delivery challenges, engaging community from multiple sectors.
Drawing on the expanding social innovation in health movement, the Social Innovation in Health Initiative (SIHI) was launched in 2014.2 SIHI is a diverse network of community members, innovators, researchers and government leaders focused on creating an enabling environment for social innovation and engage countries in advancing social innovation through research, capacity strengthening and advocacy. SIHI aims to unlock the capacity of all health system actors and stakeholders, including innovators, policymakers, front-line workers and academics, and to advance community-engaged social innovation. Community engagement, defined as the process of working collaboratively with groups of people who are affiliated by geographic proximity, special interests or similar situations with respect to issues affecting their well-being,3 remains a critical factor in driving this culture shift. While the importance of community engagement has been recognised for decades,4 there has been more research and action on community engagement to ensure sustainability. In addition, non-health collaborations can help social innovations to have impact on social, environmental and other outcomes.
There is limited research on social innovation in health.5 Few studies have examined community engagement or financing related to social innovation. In addition, research has not explored relationships between Sustainable Development Goals (SDGs) and health and non-health outputs emerging from social innovations. Better understanding community engagement, financing and outcomes related to social innovation will help to expand this field and increase the rigour of research.6 TDR (the UNDP/UNICEF/World Bank/WHO Special Programme for research and training in tropical diseases), the WHO and other organisations have underlined the importance of high-quality research on social innovation.5 7
In this paper, we assess social innovation cases identified through a crowdsourcing open call approach.8 Crowdsourcing has a group of individuals solve all or part of a problem and then share solutions with the public.9 The comprehensive open call process appointed independent expert panels to review key aspects of each social innovation. The crowdsourcing open call was conducted in 2015 and subsequent open calls resulted in selection of a total of 40 case studies conducted by SIHI researchers. These solutions have increased access to affordable and effective healthcare delivery and strengthened public health systems. This analysis uses descriptive case study research methodology to investigate mechanisms of operation and learn transferable lessons from social innovations, including critical elements of community engagement. The purpose of this study is to use a qualitative descriptive analysis to assess 40 social innovations in health identified through a global open call to better understand community engagement, financing and social determinants.
Methods
Scope
The overarching goal was to gain insights from existing case studies of social innovations used across Africa, Asia and Latin America, to determine best practices and gaps to be addressed. A qualitative analysis of 40 social innovations identified characteristics of successfully initiating community-led or community-engaged innovations to enhance healthcare delivery.
Study design
The study adopted a qualitative analysis of case studies identified by the SIHI network. We used textual methods to identify themes and extract relevant data on community engagement and other characteristics from 40 selected social innovation case studies. This qualitative analysis involved an iterative process combining elements of content analysis and thematic analysis. We also examined the depth and nature of engagement using the community engagement framework.3
Case study recruitment
The SIHI network has periodic global and regional crowdsourcing open calls to identify social innovation. More details about crowdsourcing open calls can be found in the TDR/SESH/SIHI practical guide.10 The network has consensus guidelines on implementing open calls.11 The first crowdsourcing open call took place in 2015, with subsequent regional open calls during 2017–2018. The open calls invited individuals and organisations from all backgrounds and sectors to nominate social innovation initiatives that help to solve local healthcare delivery challenges. Nominations were received through a dedicated online platform and open during a 6- to 8-week period. To review and select innovations, SIHI appointed independent panels comprising external experts to review submissions received through the call according to a predefined criteria: degree of innovativeness, affordability, inclusiveness and effectiveness. Each project was reviewed by at least two panel members and high scoring projects proceeded to a second round of review. This second review assessed the extent to which cases contributed to knowledge about social innovation in health. SIHI researchers then travelled to each local partner to see the implementation and collect additional data in the form of document reviews, participant observations and semistructured interviews. This resulted in a total of 40 case studies.12
Data extraction
We used qualitative data analysis methods to examine text in the case studies. Thematic content analysis addresses a priori issues embedded within the data while allowing enough flexibility to incorporate new and hitherto unconsidered issues. Specific themes generated prior to coding were merged with existing data-driven codes to develop analytical and descriptive themes, respectively. Three coders individually coded the case studies. During coding, if a theme was unclear, it was discussed within a core group of five authors for resolution.
Data analysis
Following extraction of key elements of community engagement and other characteristics of social innovations from detailed descriptions of 40 selected case studies, content analysis was carried out using inductive and deductive coding. Our coding drew on a community-based participatory research framework developed by the US Centers for Disease Control and Prevention.13 This framework (figure 1) was developed which aligned with the levels of engagement framework as defined as: Inform (provides community with information); Consult (gets information or feedback from the community); Involve (involves multiparticipation with community on issues); Collaborate (forms partnerships with community on each aspect of the project), and Shared Leadership (strong or long-term partnership structure is formed).14 We also used content analysis aligned with community engagement framework3 to generate themes that are potential facilitators and barriers of community engagement. A summary codebook was then used to code each case study submission separately. An analysis of descriptive characteristics of social innovations were similarly examined to facilitate understanding of phenomenon across social innovations.
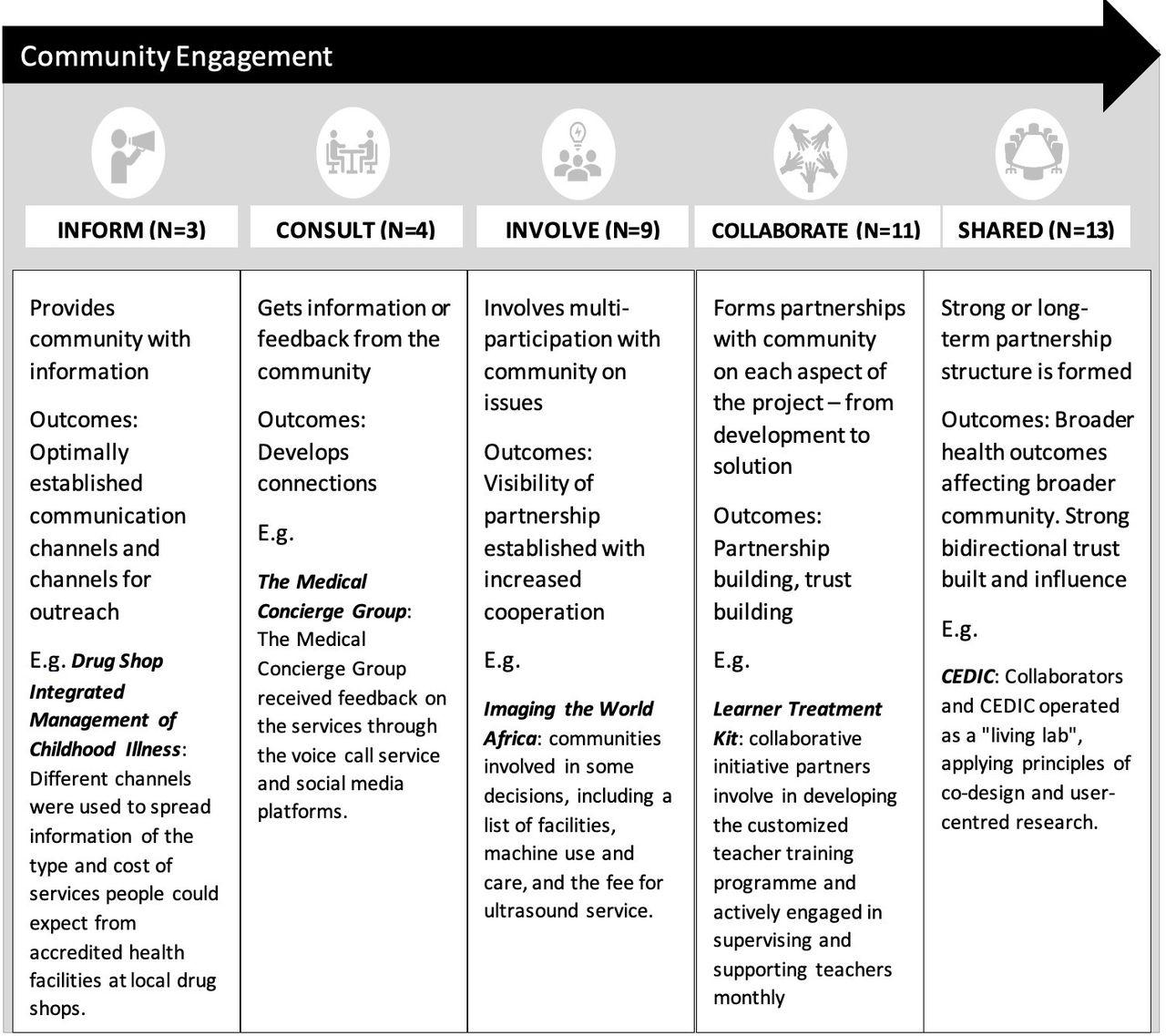
Spectrum of community engagement demonstrated in social innovation in health projects. Categories adapted from the US Centers for Disease Control and Prevention framework.
We also categorised each social innovation according to which SDGs it could potentially address. We undertook this analysis because social innovations often reach beyond the health sector,1 and this provides a more rigorous framework for categorising non-health values in a structured way.
Results
Among the 40 case studies (table 1), more than half of them, that is, 52.5% (21/40) were from Africa. 27.5% (11/40) of cases were from Asia. 20.0% (8/40) of cases were from Latin America and the Caribbean. Nearly half of the social innovations 47.5% (19/40) focused on provision of primary healthcare services whereas others provided maternal and child health, malaria and HIV services. Regarding the health system focus of these social innovations, slightly more than a third aimed at improving service delivery while 17.5% (7/40) of them were focused on improving health workforce and community service delivery.
Characteristics of social innovation case studies included in this analysis (n=40)
Majority of the beneficiaries of the social innovations were women (87.5%), children (77.5%) and men (70.0%). It was noted that most of these social innovations 57.5% (23/40) were financed through research grants. We observed substantial community engagement across the cases studies. The largest group of social innovation projects was classified as shared leadership (n=13, 32.5%), followed by collaborate (n=11, 27.5%), involve (n=9, 22.5%), consult (n=4, 10%) and inform (n=3, 7.5%). Shared leadership demonstrated strong and often long-standing relationships, grounded in shared principles, co-ownership or partnerships between social innovators and community stakeholders. Processes of inclusive training and capacity building were shown in shared leadership cases (online supplemental table 1). One team provided medical and management training programmes to faith-based primary care clinics, nurturing mentorship. This service also provided access to drug delivery and medication insurance.
Supplemental material
Collaborative cases involved community partners at several steps. One case study had teachers facilitate school-based malaria detection and treatment referral in Malawi. Community members, especially parents, were mobilised to develop and evaluate the programme. The District Health and Education officials supervised and supported teachers on a monthly basis.
In ‘involving cases’, communities participated in only some processes of the project. Another social innovation had community partners providing knowledge, materials and craftsmanship to build and maintain boats used for the intervention. Boats were then assigned to midwives in each of the village health stations. In consultative cases, community stakeholders participate in either the initial stages being required for information or offered feedback or both. Lastly, in informative cases, social innovators directly spread information or provided suled by local nursesrveys to community members. One project in Kenya delivered health promotion and disease screening services in a neighbourhood-based primary healthcare chain at affordable private rates.
Our analysis identified a wide range of financing mechanisms to localise support for social innovation projects, studies and pilots. Social innovation financing came from research grants (23), national or provincial government support (15), revenues from sales (13), donations (13), local government support (10) and private sector contributions (5). Although financing mechanisms included both foreign and domestic sources, there was a prominent trend towards localisation and strong local municipal, regional and national support. The often long-standing relationships between social innovators and local community stakeholders were leveraged to create resources for the development and maintenance of the social innovation. One social innovation in China15 was initially supported by foreign grants, but then support was transitioned to a mix of foreign and domestic research grants. In addition, strong links between social innovators and beneficiaries provided mechanisms for revenue generation.
We also identified innovative mechanisms to finance social innovations for health (figure 2). These include community-based health insurance and nurse franchising. One community-based health insurance model16 provided coverage for hard-to-reach rural areas in Malawi. A Rwandan project created a system of rural health centres led by local nurses.17 Nurses with at least 5 years of experience can join the network and have access to a rent-free building in their village to provide health services as part of a franchise system. They received training on essential primary care services and then generated income by charging small fees with services. Partnerships with the Ministry of Health increased the likelihood of sustainability as they were able to scale or embed the initiative more broadly.

{kind=link}
{kind=link}
Localisation of financing demonstrated in social innovations.
Social innovations reported on both health and non-health outcomes. The most frequently reported health outcomes focused on improving disease-specific services (n=22). Other health outcomes included an increase in the overall efficiency of healthcare service delivery (n=10), improving maternal and child health (n=8) and providing health education (n=4). When mapped against the SDGs (table 2), all social innovations addressed SDG3 (Good Health and Wellbeing). However, some health-related benefits may have a dual impact by addressing multiple SDGs (table 2). This can be seen with interventions that provide health interventions embedded within education (SDG3 and SDG4) as well as health interventions that improve industry, innovation and infrastructure (SDG3 and SDG9).
Social innovation health and non-health impacts mapped against the Sustainable Development Goals (SDGs)
The non-health social benefits of the innovative community-based interventions were substantial. The most common non-health impact was community engagement (n=15) which is characterised by reducing inequities (SDG10) and strengthening partnerships (SDG17). Other common outcomes included capacity building (n=16), fostering digital innovation (n=8), building resilient infrastructure through housing reform (n=3) and empowering women and girls (n=5). Additional health and non-health impacts related to SDGs are highlighted in table 2.
Discussion
This qualitative study analysed social innovation case studies from LMICs to assess community engagement, financing and outcomes. Our data suggest robust community engagement across the life of the social innovations, with over half of the cases meeting criteria for shared leadership or collaboration. Diverse and novel financing mechanisms were used in these cases. Non-health outcomes captured social benefits from the interventions. Our study extends the literature by focusing on social innovation in LMICs, examining non-health outcomes related to social innovation and measuring community engagement.
Our study showed robust community engagement across all types of case studies included. This finding contrasts a broader literature showing minimal community engagement18 19 and is consistent with other social innovation research. While shared leadership projects achieved long-term investments in community partnerships and empowered the community to make their own decisions, projects with a lower level of community engagement were still able to increase awareness and knowledge in the community. Our study provides insights on community engagement that could similarly be organised in other LMIC settings. Potential explanations for the higher level of community engagement include more diverse funding, engagement of community leaders and local government stakeholders20 and involvement of beneficiaries in the planning of social innovations.21 We speculate that the increased community governance in social innovation research studies may allow for greater sustainability, but further dissemination and implementation research is needed.
Our data show diverse funding sources to support social innovation. In addition to traditional scientific research grants, governments at all levels supported social innovation through funding, in-kind support, policy support and advocacy. This is important because cooperation between organisations and the public sector plays a key role in creating an environment conducive to social innovation. Social innovation collaboration between organisations and public sector partners can accelerate universal health coverage programmes and contribute to SDGs.1 In addition, sustainable funding is essential for health services, especially services for marginalised groups like people living with HIV. These diverse funding sources increase the likelihood of sustainability.
The study suggested that many social innovation projects addressed health service delivery gaps. Similarly, other studies noted that health innovations improve health service delivery in LMICs.22–25 The focus on health service delivery may be related to the importance of this topic within LMIC health systems. In addition, this finding may have been related to many social innovations directly related to primary care services. Many studies indicate that comprehensive primary healthcare services are an essential part of strengthening the health system.26 27 This suggests the importance of social innovations in expanding primary care services to achieve universal health coverage.
Our analysis of social innovations demonstrated non-health outcomes that align with the framework of the SDGs. Social innovations are wide ranging and encompass products, services, behavioural practices, and models or policies which can work to solve various community challenges. Improving healthcare delivery involves influencing the social determinants in the environment. As a result, it is important to explore innovations that can alter environments through non-health spillover effects and indirectly improve health. Our research shows that social innovations may have direct and non-direct mechanisms for improving health outcomes. Cocreation through community engagement provides an opportunity for stakeholders to contribute and learn processes that affect their health and can influence scale-up and sustainability. For example, social innovations that build modern home infrastructure to facilitate vector control show how health and non-health outcomes are often tightly linked. Research on non-health outcomes and spillover effects produced by social innovations is warranted.
A few limitations should be considered when interpreting the study findings. First, this is a small sample of social innovations and is not representative of the various community-based solutions present within the selected contexts. As a result, the study was not powered to assess differences in community engagement, financing or other key outcomes. However, our sampling frame was determined through a global consortium that intentionally focused on LMICs. Second, the data collected were limited to the compendium text alone. Qualitative research is needed to better understand the social context of social innovation and community engagement. Third, the extent of community engagement was not completely captured in the case study texts. At the same time, each social innovation was assessed by an external expert panel.28 Fourth, our data did not include detailed information about the evolution of financing over time, mechanisms for securing government support and how financing could work outside of SIHI hubs. Each of these financing issues is worthy of further consideration.
In conclusion, finding appropriate ways to fund social innovations and tailoring solutions to local conditions, social structures, emergencies and constraints, is more likely to address health issues across services. Embedding local stakeholders and communities in any stage of the ideation, implementation and evaluation of social innovations can also enhance the uptake and sustainability of interventions. Social innovations can provide direct and indirect health and non-health outcomes that catalyse the achievement of the SDGs. There is a need for more rigorous community engagement research to better understand underlying elements to emulate in similar conditions. From a policy perspective, this study demonstrates the funding mechanisms that may be useful for social innovators and partnerships to support future social innovation initiatives.
Data availability statement
Data are available in a public, open access repository. All data are available and listed in the supplementary material.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
Acknowledgments
We thank the authors of the studies included in this review, as well as the SIHI team members who helped to identify, assess and report on these social innovations: Rachel A Hounsell, Juliet Bamulagayo, Maxencia Nabiryo, Barwani Msiska,Vincent Jumbe, Arturo M Ongkeko, Jana Deborah Mier-Alpaño, Martha Milena Bautista, Diana Castro Arroyave and Uche Amazigo.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
PA and JDT are joint senior authors.
Twitter @JosephTucker
Contributors PM, EA, PA and JDT developed the original idea for this study. JL, XS, YT and LVN identified data and helped organise data. PM and JDT wrote the first draft of the manuscript. BH, PA, and JDT supervised the study. All authors approved the final version.
Funding The work received support from the TDR, the Special Programme for Research and Training in Tropical Diseases cosponsored by UNICEF, UNDP, the World Bank and WHO. TDR is able to conduct its work thanks to the commitment and support from a variety of funders. These include our long-term core contributors from national governments and international institutions, as well as designated funding for specific projects within our current priorities. For the full list of TDR donors, please visit TDR’s website at https://www.who.int/tdr/about/funding/en/. TDR receives additional funding from Sida, the Swedish International Development Cooperation Agency, to support SIHI.
Disclaimer The authors alone are responsible for the views expressed in this article, and they do not necessarily represent the decisions or policies of PAHO or TDR. In any reproduction of this article, there should not be any suggestion that PAHO or TDR endorse any specific organisation services or products.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, conduct, reporting or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.