Article Text

Statistics from Altmetric.com
Summary box
What are the new findings?
Inpatient telehealth programmes can augment care delivery by enhancing patient connection to outside support systems.
Successful implementation and sustainability of telehealth programmes require new workflows to minimise burden on frontline clinicians.
This case study demonstrates that a video visit consult service can be feasibly implemented across diverse health systems.
How might it impact on healthcare in the future?
In the future, inpatient telehealth programmes may connect patients to social support mechanisms beyond family members and loved ones, including expert consultants from other institutions or patients’ outpatient primary and specialist clinicians.
Introduction
As COVID-19 spread across the globe, hospitals restricted visitors to protect patients and healthcare providers.1 The absence of in-person visitors, who play a central role in patient well-being and clinical decision making by clarifying medical histories and bridging linguistic and cultural divides, left patients vulnerable to social isolation, delirium and fragmented clinical care.2 With ongoing COVID-19 infections, health systems continue to grapple with how to support patients and loved ones during visitor restrictions.3
Many technology-driven innovations emerged during COVID-19 to conserve personal protective equipment, protect healthcare workers and prevent nosocomial transmission, but, to our knowledge, this was the first programme designed by medical trainees with the specific goal of connecting patients with their loved ones.4–8 Here, we describe the design and early impact of an inpatient video-conference telehealth initiative, and we provide a model for health systems interested in designing similar telehealth programmes to connect patients and loved ones. The objective of this initiative was to reconnect patients with their loved ones during COVID-19-related visitor restrictions across diverse hospital settings to improve patient experience and care delivery.
Methods
Setting
Resident physicians and medical students provide clinical care at three affiliated health systems, including a large tertiary referral centre, a county hospital, and a veterans administration hospital (VA). Sites were chosen because of their central affiliation with the tertiary academic medical centre in which trainees work. Each health system is independently organised with separated electronic health record (EHR) systems, governance, and funding mechanisms. Implementation across different sites helped test the feasibility of a video-conferencing telehealth initiative across disparate settings.
Team design
The leadership team consisted of resident physicians in the Internal Medicine Residency Programme. Given the diversity in organisational structures, patient populations and resources at each hospital, residents divided into site-based teams. Medical students, who were largely removed from clinical responsibilities during initial stages of the pandemic, joined these teams (table 1). Each site developed its own meetings, roles and operations. Weekly cross-site meetings were held to share best practices and solutions to obstacles.9 10
Project design
Fundraising and technology
Guided by literature from the non-profit setting, the team drew on strong levels of motivations for donation during COVID-19 to design the fundraising process, which included research, solicitation and stewardship.11 The team created a map of our donor networks and solicited tablet donations, established a crowdfunding campaign, and ultimately raised US$10 000 to pay for ancillary hardware (eg, speakers and stands).
The repository of tablets, which included Amazon Fire, Android and Apple tablets, were allocated across sites based on demand and information technology (IT) requirements. At the tertiary hospital, devices were customised and enrolled in a secure wireless network for optimal control of network bandwidth, while devices at the county hospital were permitted to operate on guest networks as private devices. At the VA, lack of wireless connectivity initially impeded widespread tablet use until wireless hotspots were obtained and used throughout the hospital.
Multiple software platforms were trialled in parallel and evaluated based on criteria including privacy, security and familiarity. Zoom was ultimately chosen for video conferencing calls based on its support for multiple callers, short learning curve for participants and providers, and Health Insurance Portability and Accountability Act (HIPAA) compatibility.12
Workflows
To maximise use of a limited number of tablets and minimise the number of individuals to be trained, medical student-led consult teams were created to coordinate video visits. To request a visit, any clinician could page the consult team during the business hours. The consult team coordinated with the patient and loved ones to obtain consent, download and troubleshoot Zoom, schedule visit times and set up the tablet (figure 1). Many patients were elderly with limited English proficiency, experienced challenges with navigating technology, did not own video-enabled devices, or were too ill to reach out to loved ones on their own. In response to challenges, the designed workflows involved hands-on support to organise and set up video conferencing calls for patients. For patients in the intensive care units, students remained nearby to provide ongoing technological support throughout the duration of the video conferencing call.
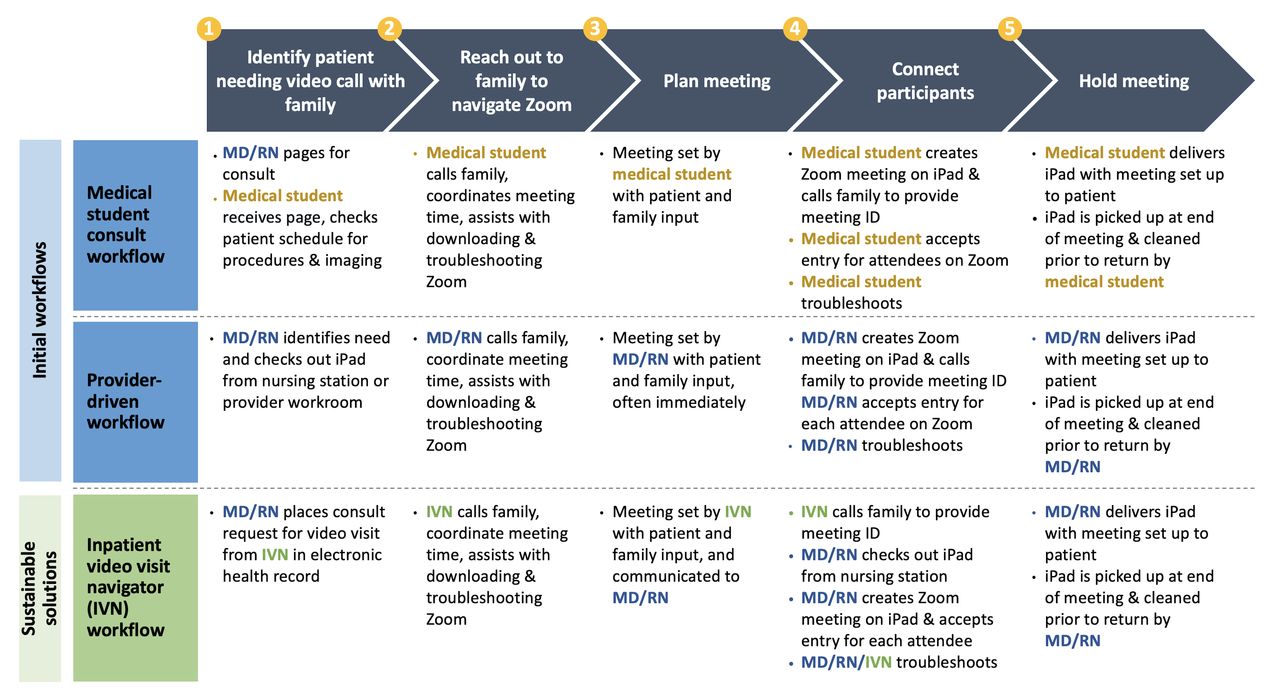
{kind=link}
Video visit workflow design. MD, Medical Doctor; RN, Registered Nurse.
At the tertiary hospital, in response to requests for after-hour consults, a ‘provider-driven’ self-checkout workflow was developed for residents and nurses to checkout tablets on demand. Based on initial success, the other two hospitals also established ‘provider-driven’ systems (figure 1).
Sustainability
Each site engaged with stakeholders to design sustainable solutions. At the tertiary hospital, the team worked with a newly established institutional inpatient telehealth team to design an inpatient video visit navigator (IVN) role in which a dedicated employee could subsume the responsibilities of volunteer students (table 1). In this model, a clinician places a consult order in the EHR to the remote IVN with information about the requested consult including who should join the meeting, the type of meeting requested (eg, social visit, caregiver teaching), and any additional information about the consult. The IVN role is staffed by a trained health system employee with access to the EHR, which provides access to information about the patient’s medical context. The IVN role is suitable for individuals trained as nurses, medical assistants and licensed vocational nurses. The IVN helps loved ones download and troubleshoot Zoom and sets up the video call on a secure tablet with the help of the patient’s bedside nurse. Given the programme’s success and ongoing need, the health system provided staffing for two full-time video navigators who coordinate video visits from 8:00–20:00 hours daily. Further, a private family donation provided funding to expand efforts at the tertiary hospital and the county hospital.
Results
Video visits began on 9 April 2020, 1 month after visitors were prohibited from hospitals in San Francisco per the citywide public health mandate. Over 100 visits were completed by early May and 456 visits by early June, which accounted for 190 unique patients. Approximately 52% of patients requested repeat calls. Video visits were conducted in 12 different languages with 71.6% of calls in English, 10.0% in Spanish, 9.5% in Cantonese. Most video visit consults came from Medicine and intensive care units (63%) and neurology/neurosurgery services (22%). Many of the telehealth use cases were similar across sites; the most common use cases for video visits included connecting patients to family, medical updates and decision making with providers, end-of-life care and caregiver teaching. However, unique site-specific cases also emerged (table 2).
Use cases for video visits between patients and loved ones
Discussion
In response to visitor restrictions during COVID-19, medical trainees rapidly developed, designed and implemented a patient-centred, sustainable telehealth programme across three hospitals to connect patients and loved ones and improve clinical care. We describe below several key aspects of the initiative realised through the process of implementation.
Early barriers and solutions
The need to overcome early barriers led to frequent communication among team leads at each site, sharing learnings and resources. Examples of initial barriers included unmet needs for video calls, low awareness and utilisation of tablets for video calls, lack of knowledge around using new technology platforms such as Zoom, and inefficiencies in setting up calls with families. Ultimately, sites converged on a centralised consult service, which met key considerations including the need to have personnel with deep knowledge of workflows, alleviate frontline staff of additional responsibilities and maximise use of a limited number of tablets. Analysis of this initiative’s implementation highlighted key drivers of organisational buy-in, including openness to change during COVID-19 and alignment of initiative goals with the organisation’s mission to deliver patient-centred care.
Additional benefits beyond initial expectations
The use of tablets extended beyond their original purpose. At the tertiary hospital, tablets were used by patients to attend alcoholics anonymous meetings, and at the VA, tablets were used to help patients pay bills and access educational materials. While the aim was to reconnect patients and their local loved ones unable to visit, we found that family members from around the globe joined video calls. Even beyond the era of visitor restrictions, patients will continue to benefit from interventions that support active engagement of social support systems. Health systems should build or leverage existing inpatient telemedicine infrastructure to engage loved ones using IVN to field consults across the hospital and coordinate with distanced loved ones on a regular basis.
Value of trainees
The project also highlights how academic institutions could better capitalise on the diverse skillsets of its workforce, including trainees, to inform clinical care delivery improvement.13 14 Resident physicians and medical students frequently bring deep experience in diverse fields adjacent to medicine including operational experience, project management, advocacy, quality improvement and entrepreneurship. Working together, trainees combined their expertise with front-line clinical experiences and tacit understanding of the hospital systems to create this initiative.
Limitations
The initiative’s large scale and compressed implementation timeline was labour-intensive and used an untapped workforce made temporarily available by circumstances surrounding the COVID-19 pandemic. This limitation was mitigated by the development of self-checkout workflows and design of designated roles to assist in connecting patients and loved ones. Health systems frequently have volunteers and employees in need of temporary work accommodations who could be trained to serve in the IVN role.
Conclusions
Our rapid design and implementation employed the expertise and availability of medical trainees to improve communication among patients, loved ones and clinical teams through telehealth. This case study can serve as a model for health systems looking to create a sustainable inpatient telehealth programme to connect patients and their loved ones across different hospital settings. Further research is needed to elucidate the impact of inpatient telehealth on patient satisfaction and health outcomes.
Ethics statements
Acknowledgments
We would like to thank Michelle Mourad, MD and Lev Malevanchik, MD for their support and guidance throughout this project as well as the many trainees who contributed their time and effort to make this project a success.
Footnotes
Twitter @nickthomasmed
Contributors SG conceived of and presented the idea and wrote the initial manuscript draft with the help of EH, TP and NT. IG-G, KJ and ZL provided key contributions to the results and discussions sections. AV served as the senior mentor and supervised the findings of this work as well as provided input on each draft of the paper. All authors discussed the results and contributed to the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.