Article Text

Abstract
Introduction Opioid overdoses claim tens of thousands of lives every year. Many of these deaths might be prevented if overdose-reversal medications such as naloxone are administered in a timely manner. Drones may help overcome barriers to timely arrival on scene for opioid overdoses. This study analyses the time required for a drone carrying naloxone to traverse various distances, simulating the response time for a drone to the scene of an opioid overdose. For comparison, we used the time required for ambulances to traverse similar distances while responding to the scene of actual or suspected opioid overdoses.
Methods Fifty flight trials, using a modified Dà-Jiāng Innovations (DJI) ‘Inspire 2’ drone, were conducted across seven distances, and the travel time for the drone was then compared with historical response time data from 200 actual or suspected opioid overdose cases that occurred within Detroit, Michigan.
Results We determined with 95% certainty that drone arrival times were discernibly quicker than ambulance arrival times at all distances where sufficient data were available to perform statistical comparisons including 0.5 km, 1.0 km, 1.5 km, 2.0 km and 3.0 km.
Conclusion We have shown that a drone is capable of travelling several ranges of straight-line (ie, ‘as the crow flies’) distance faster than an ambulance. Further exploration into the use of drones to deliver life-saving therapies in urban and rural settings is warranted. Head-to-head prospective trials that consider the practical challenges of medical drone delivery are needed to better understand the viability of incorporating this technology into existing emergency response infrastructure.
- delivery
- drone
- opioid overdose
- emergency medicine
- accessible
Statistics from Altmetric.com
Introduction
Unmanned aerial vehicles (UAVs) and unmanned humanitarian vehicles, also referred to as ‘drones’, represent emerging technological platforms that may allow for innovation across various sectors. These dynamic aircraft make available the airspace above cars and below planes that, until recently, has only been used by helicopters. Recent exploration of the use of drone technology for parcel delivery by companies like Amazon, Google, United Parcel Service (UPS), Dalsey, Hillblom and Lynn (DHL), and Domino’s Pizza suggests that there is significant interest in assessing the viability of aerial delivery models that include the use of drones.1 Moreover, advances in drone technology have paved the way for novel humanitarian uses in the healthcare sector, especially to accomplish urgent medical tasks in places that lack sophisticated transportation infrastructure.2
Opioid overdoses claimed 47 600 American lives in 2017,3 yet a highly effective reversal agent, naloxone, is readily available. Efforts to increase naloxone distribution are increasing,4 but this has not stemmed the tide of opioid overdoses. Naloxone’s ability to reverse an opioid overdose is fundamentally time-dependent, so minimising the time required to make contact with the patient and get the drug on-scene is critically important. Drone delivery of naloxone may be able to provide rapid naloxone delivery resulting in expedited resuscitation. However, data on time-to-scene arrival for drones compared with medical first responders (MFRs) are lacking. As such, we sought to quantify the time required for a four-rotor drone to fly various distances corresponding to the distance from dispatch-to-scene for 200 actual and suspected opioid overdoses that took place in the city of Detroit throughout 2018. This effort will serve as a preliminary comparison of the speed with which a drone can travel across certain distances relative to an ambulance. Our goal is to first establish whether or not this platform can even travel as fast as—or possibly faster than—ambulances under ideal conditions. Our results can suggest the viability of further studies to assess the practicality of using drones under conditions more representative of what would actually be found in a typical urban setting. The discovery of dramatic speed advantages, for instance, could help facilitate applications for waivers necessary to conduct head-to-head trials of drone flight times versus ambulance travel times in a real-world context.
Methods
Flight trials were conducted using a customised version of the commercially available Dà-Jiāng Innovations (DJI) ‘Inspire 2’ drone. This 3.4 kg aircraft features two lithium polymer batteries that allow for 23–27 min of flight time. The drone has a maximum range of 7 km, a maximum speed of 94 km/hour, and a maximum wind resistance of 10 m/s. It is equipped with an internal global positioning system, as well as dually redundant upward, downward and forward vision sensors that allow for multidirectional obstacle avoidance.5 The platform comes standard with a forward-facing first-person view camera, but we outfitted our model with an additional Zenmuse X4S video camera attached to a three-axis gimbal, so that we could monitor flight paths via the 4K video output.6 We further modified the drone in several ways to make it more suitable for emergency medical deployment (figure 1). We wrapped the drone with a reflective neon skin and also affixed emergency service decals. A 600-lumen headlamp was mounted to the top of the vehicle that would enable easier identification of the patient and bystanders on-scene if this technology were deployed in a real-world setting. Finally, we equipped the drone with mechanical payload release hooks that carried a shock-proof container that housed both intranasal naloxone, as well as instructions for administering the drug.

Customised DJI Inspire 2 drone used for this study. DJI, Dà-Jiāng Innovations.
The drone was registered with the Federal Aviation Administration (FAA) before flight trials began and subsequent tests were undertaken in accordance with regulations for small unmanned aircraft as outlined in the FAA’s Part 107 guidelines.7 In accordance with 14 Code of Federal Regulations (CFR) §107.19, a remote pilot was in control throughout the entire duration of every flight. Adhering to 14 CFR §107.33, we employed a visual monitor to ensure that the areas immediately adjacent to the flight paths remained clear during the course of testing. Peak altitude did not exceed 400 ft (122 m), as mandated in 14 CFR §107.51, and no trials were undertaken within restricted airspace, as defined in 14 CFR §107.41. Tests were conducted during the daytime, as required by 14 CFR §107.29. Finally, the drone remained within visual line-of-sight for all tests (per 14 CFR §107.31), and no missions involved flying over human beings (14 CFR §107.39).
Fifty total flight trials were conducted during clear weather conditions (max. wind speed 3.7 m/s) between November and December 2018. The drone was flown across seven different straight-line (ie, ‘as the crow flies’) distances, as outlined in table 1, to obtain data that spans the distance ranges that are common for MFR responses, according to our reference data set. Each trial began with the drone ascending to a height of approximately 45 m. This elevation was arbitrarily selected as a representation of what might be necessary to avoid obstructions that would be present in an urban environment, while allowing us to remain comfortably within the altitude restrictions established by the FAA in 14 CFR §107.51. After reaching an altitude of 45 m, the drone was flown the straight-line distance corresponding to the particular distance being tested (eg, 0.25 km, 0.5 km, 1 km, etc). In order to keep the drone within visual line-of-sight at all times, we executed trials for distances of greater than 500 m as a series of continuous 500 m ‘sprints‘whose total equalled the overall distance being studied. In other words, after starting the stopwatch, the drone would fly up to a height of 45 m, and then continuously travel forward 500 m then back 500 m along a straight-line path until the sum of the distance being studied, for example, 3.0 km, was reached. The total time required for the drone to take-off, vertically ascend to its ‘cruising altitude’, and then travel the horizontal distance in question was recorded in the ‘UAV - Time’ (UAV-T) variable. Descent time was not included as part of the UAV-T value, as this trial only sought to compare the time required for a drone to travel specific distances versus an ambulance. Both drones and ambulances may arrive on-scene and then encounter issues finding the patient. Therefore, because it would be difficult to standardise how long it would take a drone to actually make contact with a patient, we simply chose to compare drone and ambulance transit times, starting from when each vehicle departed its respective dispatch site (ie, fire house for the ambulances and launch site for the drone) and ending when it first reached the scene, or simulated scene in the case of the drone. To derive this travel time for ambulances, we used 200 MFR runs in which first responders reported dispatching naloxone after encountering patients suffering from actual or suspected opioid overdoses. All of these runs took place within the city of Detroit, and they all occurred between January and December 2018. The data set was provided by the Detroit East Medical Control Authority, and it detailed the time elapsed between MFR dispatch from various firehouses around the city and arrival on-scene. These values were recorded in the ‘medical first responder-time’ (MFR-T) variable. MFR-T was compared with UAV-T across different distances in order to identify any disparities in the time between dispatch and arrival-on-scene for the MFRs as compared with the elapsed time for the drone to travel the same distance.
Number of drone flights and MFR responses at each distance
We used an online platform8 that calculates the straight-line distance between two street addresses in order to determine the straight-line distance from the fire station to the patient for each MFR run. As we took drone measurements only at discrete distances, we rounded the MFR data to the nearest half kilometre for comparison with the drone data. After rounding, distances with fewer than five data points were not included in further analysis. For each distance, the mean value and SE of the mean of MFR-T was calculated. Similarly, the mean value and SE of the mean of UAV-T was calculated at each distance.
The value of interest in this study is the difference between UAV-T and MFR-T, which we will denote ∆T. The mean value of ∆T at a given distance is calculated by directly computing the difference in the mean values of UAV-T and MFR-T, and the SE on this measurement is determined by adding the SEs of UAV-T and MFR-T in quadrature. All data analysis and associated visual plots were produced and conducted using a Python code that we created to perform the calculations.
Results
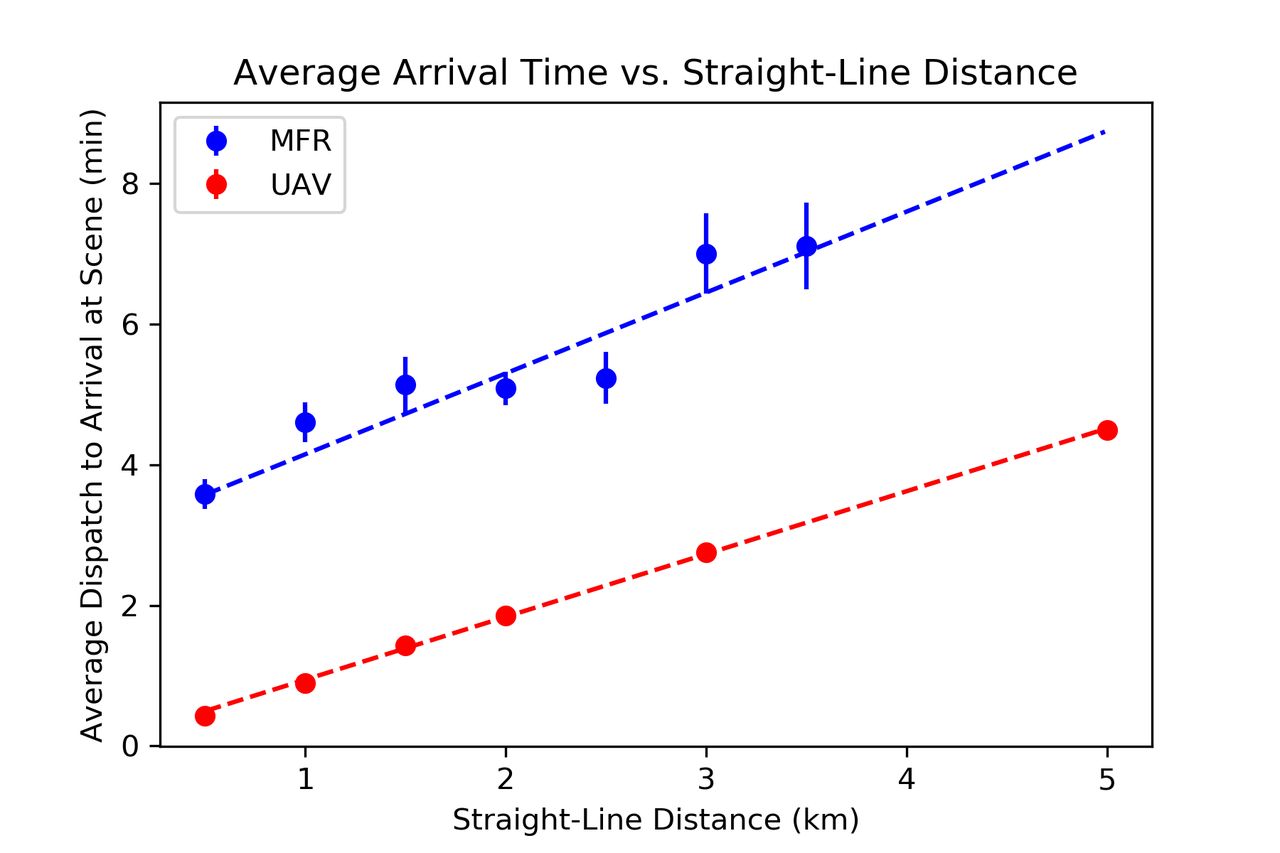
The averages of UAV-T and MFR-T (in minutes) are shown in figure 2, with all error bars corresponding to 1 SE, and results are shown in table 2, where we were able to determine the values of ∆T to within a 95% CI at various distances. These data show with greater than 95% certainty that drone travel times are demonstrably better than ambulance arrival times at all distances where sufficient data was available to perform a statistical comparison—namely, distances of 0.5 km, 1.0 km, 1.5 km, 2.0 km and 3.0 km. At the remaining distances, we were not able to draw statistically significant conclusions due to either an insufficient quantity of first responder data at these distances (ie, fewer than five data points), or because we did not conduct drone trials at such distances.
Mean time between dispatch and arrival for MFR (MFR-T) versus drone (UAV-T) at various distances (95% CI)
{kind=link}
{kind=link}
Average drone response time (UAV-T) versus average ambulance response time (MFR-T) across various distances. MFR-T, medical first responder-time; UAV-T, unmanned aerial vehicle-time.
Discussion
The response time difference that we discovered between the drone and the MFRs was less than what has been previously reported. For instance, Swedish researchers conducted a similar study analysing the time required for drone delivery of an automated external defibrillator in out-of-hospital cardiac arrest situations as compared with standard emergency medical services (EMS).9 They found that the drone arrived more quickly than EMS in all cases with a median reduction in response times of 16:39 min. However, the median EMS response time for their comparison trials was 22:00 min. It naturally follows that they would find a much more dramatic improvement considering the median response time for Detroit MFRs across all of the straight-line distances we analysed (none of which exceeded 6.34 km) was only 5:00 min. Drones may be especially valuable in areas with protracted response times, like the region from the Swedish study, or certain rural areas of the USA, where researchers have found that median response times are double that of urban centres (13 min vs 6 min, respectively).10
Still, our results demonstrate that drones may also be useful in an environment that has relatively fast response times, as our vehicle is capable of travelling faster than some traditional MFRs responding to actual or suspected opioid overdoses within the city of Detroit. Drones may still serve a purpose in urban settings, as city officials could identify areas with particularly high overdose rates and establish drone-deployment stations in the proximity of high-risk areas. Should an overdose occur within the radius of a given station, a drone equipped with naloxone could always be ready to quickly reach the patient and empower bystanders to assist even if it is mere minutes before first responders arrive.
A system like this would require a bystander to be present to assist the patient, who may be located inside dwellings; however, even if no one were to be on scene when the vehicle arrives, the drone might still offer valuable telemetry that assists en-route first responders. For instance, the on-board video cameras can be used to provide in-transit paramedics, firefighters or police with real-time video feeds that offer a visualisation of the scene to which they are travelling. This not only has implications for protecting first responders who might be entering dangerous situations, but it could also help them more easily locate the individual in need of assistance and generally assess the scene before actually arriving. There is no reason to believe that other urgent medical supplies, such as an epinephrine autoinjector, an albuterol inhaler, anticonvulsant medication, or an automatic external defibrillator cannot also be delivered to patients via drone.
Notwithstanding these potential applications, myriad technological, economic and regulatory considerations must first be explored before any attempts to integrate this platform into municipal emergency response services are made. We, therefore, recommend further consideration and analysis of the practical application of drones in the EMSs arena. A valuable next step may therefore be positioning a drone at a firehouse and, after a 911 call comes in, having the aircraft directly race an ambulance to the scene. This would lend clear insight into the difference in response times for drones as compared with traditional ambulances. This process could then be repeated in a number of urban and rural environments, so as to determine the optimal circumstances for drone implementation.
Although our findings indicate that drones can travel faster than ambulances across various distances, certain limitations of this study must be noted. Our comparisons were limited by the fact that we only had access to MFR response time data from a select number of overdose cases and only ones that took place within Detroit. It is also worth mentioning that all of our flight trials were conducted during the daytime, on days with clear weather and marginal amounts of wind, and they involved flying the drone only across straight-line flight paths. One major advantage of employing drone technology is that drones are often able to take a much more direct path than an ambulance, or any other traditional automobile. Since our goal was to compare UAV-T and MFR-T at various distances, we decided to compare both against the straight-line distance from dispatch to patient, rather than the distance along roads. We acknowledge that in most real-world situations, a drone would be unable to travel along a perfect, straight-line path from dispatch to patient in an urban environment, as it would need to avoid tall buildings and other obstacles. That being said, we concluded that a direct straight-line path is a more realistic approximation to the true flight path of our drone delivery method versus an indirect, non-straight-line path a drone would take if it were following the path of roads. Moreover, this was done to ensure that we were comparing UAV-T and MFR-T against the same distance metric, rather than two different quantities.
Additionally, we only conducted flight trials up to a distance of 5 km. Inspection of figure 2 suggests that a linear fit is well suited to the data in order to extrapolate how this result might extend to further distances. In doing so, we see that UAV-T appears to remain lower than MFR-T with a probability of just over 90%, indicating that drones may be faster than ambulances even at greater distances. While this result does not meet our threshold for statistical significance, it is unclear whether this is an artefact of a limited data set, or if this trend truly does not hold at longer distances. This result does suggest, however, that further studies may be warranted to determine whether the results here can be replicated for data at longer distances.
It should be noted that this methodology does not account for other factors that would impact these results at longer distances. Drones are inherently restricted by their battery and signal transmission technology. The DJI Inspire 2 platform we used, for instance, can fly for a maximum of 23–27 min with optimal usage (ie, minimal added weight, and reducing sharp, battery-depleting movements). It is also unable to reliably communicate with the receiver beyond 7 km. Our tests were only carried out across moderate distances.
In adherence with current FAA regulations, the drone could not be flown over human beings, and it had to be kept within visual line-of-sight at all times. Although researchers and corporations can apply for exemption waivers, these kinds of stringent regulatory requirements certainly hinder early-stage investigations, like this one, that seek to explore practical applications of a fairly new aerial technology. If research consistently demonstrates that drones offer significant advantages, then it is possible that regulations could change in a way that facilitates inquiry within the drone sector. However, at this point, strict federal and local airspace policies drastically limit real-world testing and especially real-world implementation of drone-based platforms.
It is important to note that while the aforementioned limitations are significant, they are not fundamentally insurmountable. Further technology and policy innovations could provide solutions to many of these challenges in the future, increasing the viability of integrating drones into existing medical response services.
Conclusion
We have shown that a drone is capable of travelling faster across several straight-line distances than an ambulance responding to the scene of actual or suspected opioid overdoses the same straight-line distance away. Our trials were carried out under ideal conditions, but further research projects that incorporate the practical considerations of urban drone flight (eg, weather, height of buildings, density of emergency response infrastructure, time required for lay people to collect and administer the therapy being delivered) are warranted. Drone technology is clearly an area of emerging interest, and, as the field progresses, researchers ought to continue evaluating the merits of using these platforms to improve patient outcomes.
Acknowledgments
In addition to our clinical and administrative advisors, we would like to extend a special thank you to Robert Dunne for granting us access to the Detroit MFR data used in our comparisons, as well as for providing mentorship and guidance throughout the research process. We would additionally like to thank Albert Jose for helping develop the drone used in this study.
Footnotes
Contributors CAT and MRT devised and planned the study, as well as conducted the flight trials, and coauthored the manuscript; they are joint first authors of this paper and are responsible for its overall content. RJW was responsible for the statistical analyses shown in this study; he devised methods for comparing our reference and collected data sets, generated relevant charts and figures, as well as authored the mathematical portion of the methods section. PDL provided clinical mentorship, helped gain access to the reference data set, ensured proper, objective execution of tests, and assisted in the editing and redrafting of the final manuscript. VHM offered administrative guidance, ensured adherence to ethical and regulatory protocols, helped devise analytical techniques and also assisted in the editing and redrafting of the final manuscript.
Funding This study was funded by a grant provided through Wayne State University’s Undergraduate Research Opportunities Programme.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data may be obtained from a third party and are not publicly available. Detroit Medical First Responder (MFR) data were obtained from the Detroit East Medical Control Authority. Inquiries related to this data sent may be forwarded to info@demca.org. Drone data were collected by our research team and may be obtained via request.