Article Text

Abstract
Experts probably have to immerse themselves in their discipline for at least a decade before they have the knowledge and insights needed to produce world-class work. Medical practitioners with long experience in their specialist fields are particularly well placed to know what type of devices might be needed to make their patients’ journeys back to health more comfortable, secure and cost-effective. Medical school curriculae, however, are devoid of formal innovation and business training at least in the UK. The strategies required to convert an idea into reality remain beyond most medical graduates’ terms of references, and progressing a ‘Eureka moment’ is perceived, perhaps understandably, as an overwhelming challenge. Indeed, as exciting, interesting and satisfying though the field can be, medical device development is a complex, time consuming and expensive undertaking requiring more than a fair share of good fortune. Contrary to the impression given by reality television programmes in which budding entrepreneurs pitch their ideas to successful businessmen, funding does not necessarily mean that an idea is worthy of success or destined for it, and vice versa. Equally, the acquisition of intellectual property is in many cases a pyrrhic victory. Using as an example the development of Tube Anchor, a novel device to secure intravenous crystalloid administration tubing, this paper outlines the pathway from concept to a marketed clinical device.
- Delivery
- Inventions
- Economics
Statistics from Altmetric.com
Introduction
Many patients in hospital receive fluids intravenously at some point during their stay. If they are confused or restless, as is often the case, there is a high risk that their intravenous cannulae will become accidentally dislodged. Irrespective of mental status, inadvertent tension on the administration tubing increases the risk of infection by making cannulae piston in and out, and the tendency for them to kink at their skin entry site leads to the familiar ward chorus of repeated pump alarms. Fear of cannula loss and the discomfort of having them replaced discourages patients from mobilising during the day and disturbs their sleep at night. Adding tape, particularly in hirsute individuals, increases the risk of skin damage and contributes further to their discomfort. Poorly functioning cannulae delay critical drug administration and interfere with intravenous hydration and nutrition. Cannula re-siting is painful, expensive in terms of time and consumables, increases infection risk and diverts nursing and medical staff from other tasks.
A subsidiary forearm anchor for administrating tubing was an idea inspired by the difficulty of looking after a particular patient whose confusion and agitation led to repeated cannula loss.
The original concept
The central design feature was to create a clamp by securing two rigid but contoured jaws to a flexible base. By flexing them apart, administration tubing could be repeatedly inserted and removed without having to detach the device from the skin (figure 1A, B). The design prototypes won a ‘Bright Ideas’ competition at our health trust.

(A) Development of the original models featuring two rigid jaws attached to a flexible base, with a channel formed between them. The silicone rubber mould is shown front right. (B) The first finished prototype. (C) The first professional prototype with a channel too wide to retain the tubing. (D) A prototype with much more enclosed channel ends and a wider gap in the middle as a thumb notch to start tube insertion. (E) Channel straightened and repositioned widthwise. The slight curve of the base is less than that of the forearm and shows the tendency for the base to lift itself away from the skin at the edges. (F) The finished shape, with a much smaller base radius to fit closely the circumference of the forearm and reduce skin and hair tug.
Intellectual property
Lack of candour rather than inadequate intellectual property protection is far more likely to block an idea and slow progress by preventing useful people from contributing, and on that basis the help of several trusted advisors was sought early on. It is very easy to overestimate the uniqueness and strength of an idea, or to assume that an idea or a patent has value in itself. This assumption is akin to a geological survey estimating ore, oil or gas reserves beneath the land that you happen to own. Without vast investment and immense expertise to retrieve it and transport it to a future market that has been predetermined to justify the expense, what lies beneath the ground is in effect worthless.
The principal function of a patent and utility of intellectual property for an innovation seems self-evident. Useful for a curriculum vitae and often pursued as a sine qua non of ‘a worthy invention’, intellectual property is a significant and sometimes overwhelming drain on financial resources, and its possession may not incentivise commercial involvement. The process of patent application disseminates design information at an early stage and theoretically signals intentions to those who might become interested in pursuing similar ends. It also precipitates a stream of official-looking but entirely spurious junk invoices from sources claiming to be dealing with the intellectual property in obscure territories. In reality, if an idea is good, endless small variations can be made to overcome almost any patent description, and processes supposedly intended to protect the inventor and designer become actively counterproductive. Funding that would be better spent on product presentation and publicity is consumed in a lottery that lawyers invariably benefit from.
Ownership and patents
The claims of an employer over the intellectual property of an employee, whether that employee is a paid member of staff or working in a purely honorary capacity, were addressed at the outset. In the case of Tube Anchor, once suitable employer disclaimers had been obtained, two international companies involved in medical dressings and device manufacture were approached using effective and straightforward confidentiality agreement templates that are readily and freely available on the internet (search terms ‘sample confidentiality agreements’).
The original British patent provided protection for 1 year, the PCT (Patent Corporation Treaty) in around 150 countries for a further 18 months, before protection in individual territories (eg, North America, India, Japan, Europe), each expensive in its own right and with considerable on-costs, would need to be considered. Design registrations for the device were also considered.
Regulatory requirements
Medicines and Healthcare products Regulatory Agency
The Medicines and Healthcare products Regulatory Agency (MHRA) were consulted to determine whether Tube Anchor should be classified as a ‘medical device’. Classification of medical devices is surprisingly complex and the excellent MHRA enquiry and advice service was used to provide ‘a best judgment at the time’, given the available information, and confirmed by letter. The limited claim for Tube Anchor was that it had no direct role in improving functioning of the administration tube or cannula, or in modifying the medication flowing through it. It was therefore felt unlikely that the product would be regarded as a medical device or an accessory to a medical device, and as such that it would not fall under MHRA jurisdiction.
CE marking
As Tube Anchor is not a medical device there was no statutory obligation to have it CE marked. CE marking indicates, however, that the manufacturer has checked that the product complies with EU legislation and the relevant harmonised European standards, and satisfies the legislative requirements to be moved and sold freely within the European Economic Area. There are therefore marketing advantages derived from the perceptions of potential purchasers and users that make the pursuit of CE registration and marking worthwhile. This was felt to be the case with Tube Anchor.
Structured planning
A SWOT analysis is a simple but useful framework for organising and focusing on Strengths, addressing Weaknesses, exploiting Opportunities and minimising Threats to a project (table 1).
The hurdles to consider and overcome during product development are summarised below (box 1).
Confirm that the idea meets a genuine need
Involve enough people to build a successful team without disclosing the idea to potential competitors
Prototyping the idea
Making a working prototype (with rapid prototyping) to convince potential manufacturing and marketing partners
Finding a manufacturing partner
Producing final designs for manufacture, ensuring that costs are low enough to create a cost effective end product
Create an identity and branding for the new device
Creating a market for the new device and explaining its purpose and how to use it
Motivating sales teams to introduce the product to clinical teams
Ensure that the value proposition for the customer is compelling
Maintain momentum over multiple years
Adding value
A collaborative agreement license was signed with CareTechnica (CareTechnica Ltd, Bristol, UK) whose aim is to help take healthcare innovations from initial idea to widespread adoption and commercial success. Their first step was to suggest employing Amalgam (Bristol, UK), a company with digital skills, technical capability and craftsmanship to draw three-dimensional models and produce high fidelity prototypes simulating as closely as possible the characteristics of polypropylene injection mouldings.
The prototyping process immediately highlighted a design constraint. Particularly when warm, administration tubing has insufficient resilience to be held securely within a soft, compliant channel. At the same time, a channel that enclosed sufficient circumference of the administration tubing to retain it, prevented tubing being inserted into it in the first place.
Four rounds of design, prototyping, mould making and casting, informed by findings from a purpose built test rig to quantify pull out and tug out forces were required to arrive at the finished design (figure 1C–F). The importance of the shape of the channel throat, designed to guide tubing into the channel, but retain it securely once inserted, was also clarified (figure 2).
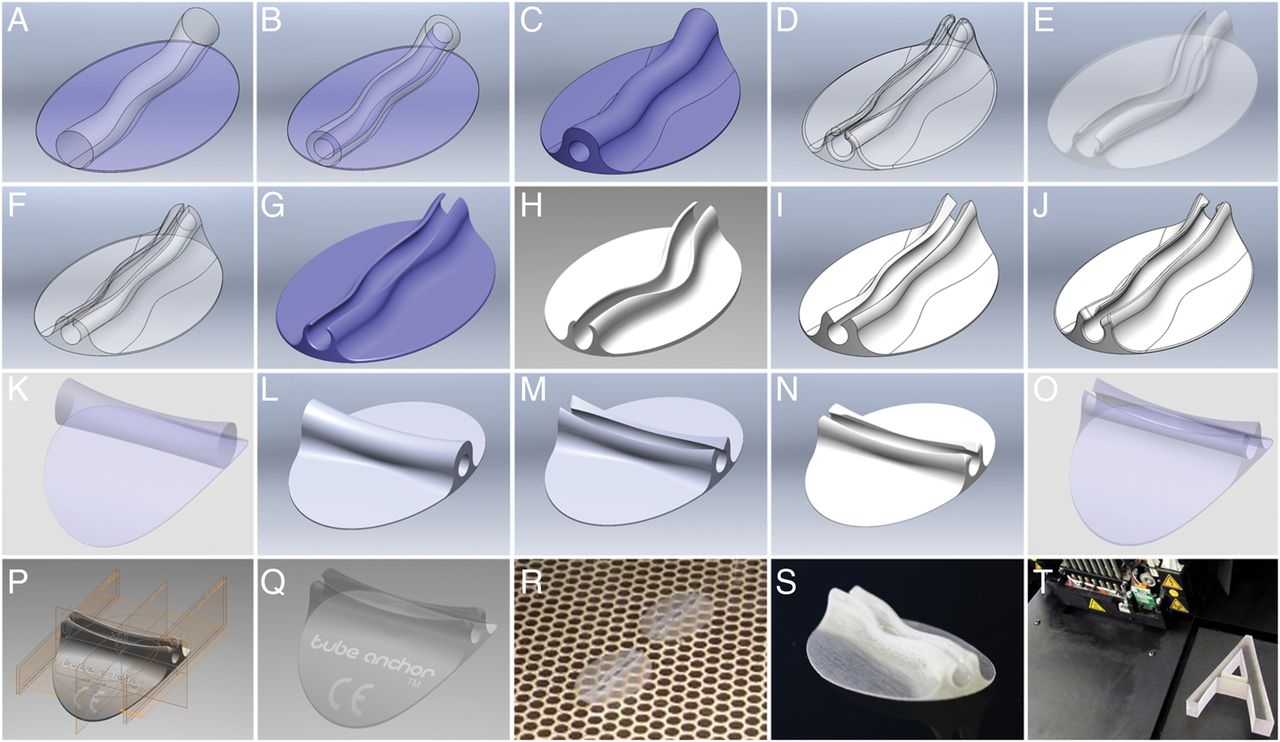
Highly experienced experts at Amalgam used ‘Solidworks’ software to produce a common base plate onto which the two channel forms were built using a versatile pair of lofted profiles, one for the outer shape and another for the inner channel (A–C) leading to the development of a series of profiles with longitudinal channels (D–J) and then transverse channels (K–Q) with different throat shapes. Shapes were three-dimensional printed using stereolithography (R and S) and later the Objet PolyJet prototyping process from ‘Objet Geometries’ (Stratasys) (T) which has superior definition and stability as shown by the 13D thin-walled ‘A’. The rigid physical forms were evaluated and adjusted before committing to prototyping in realistically pliable materials generated by resin vacuum casting polyurethane elastomer within a silicon rubber mould. This allowed variations in material stiffness and pliability to be explored and for the shape to be tested and sculpted further. The final shape was radically different from the original envisaged and will always subtly vary from the final polypropylene injection moulding.
A further important consideration was to determine the aggressiveness of highly specialised skin-safe adhesives, tested according to ISO 10993-5/-10 standards for cytotoxicity, skin irritation and skin sensitisation. This was required to control and optimise the relationship between duration of skin retention of the device relative to typical in-patient stay, tube retention and skin sheer.
Finding a manufacturing and distribution partner
Finding a manufacturing and distribution partner is far from easy. After many months of concerted effort, contact with P3 medical limited (Bristol, UK), a UK-based theatre drape and surgical accessory manufacturing company who were keen to help take the project forward occurred entirely thanks to a chance meeting with their research and development manager. It soon became apparent that creating injection tools to manufacture a design with significant overhangs in the walls of a sinusoidal channel would be complicated. Tube Anchor was redesigned to incorporate a straight channel running widthwise rather than lengthwise. This also allowed the base of Tube Anchor to be curved to reduce skin tug and increase affordance (figure 1E, F and figure 2) whilst at the same time making the design more distinctive and aesthetically pleasing.
Product identity
Strapline
The strapline evolved from ‘Curved for Comfort and Reassuringly Secure’ through ‘Quick, Clean, Secure’, ‘Comfort, Cleanliness, Safety and Security’, ‘Comfortable, Clean and Secure’, before ‘Putting the Comfort into Care’ was considered. Eventually these themes were abbreviated into the elegant, minimalist and more emotionally compelling ‘Comfort Secured’.
Logo
The design of the Logo was commissioned from Moda Chick (Bristol, UK). The primary target were nurses with a secondary target of other healthcare professionals and patients. A series of designs and subsequently design modifications were submitted and of these, a further simplification led to the final logo (figure 3).

{kind=link}
{kind=link}
{kind=link}
Examples of Logo design. Development of a logo is a highly skilled job the outcome of which depends on a comprehensive brief focusing on the intended function, name and market for a device. The journey involves finding inspiration from the shape and name of the product, hence the ‘Pringle’ shape, the profile view of the anchor as well as the words ‘tube’ and ‘anchor’. Shapes and colour have particular subliminal significance and associations. Contour bias leads us to be more comfortable with curved rather than jagged shapes, and the blue used in pharmaceutical advertising (Pantone Reflex Blue C), for example, as blue as blue can be, representing professionalism and credibility. In contrast Pantone 284U is a lighter blue referred to as ‘baby blue’ in the fashion industry, a colour that confers a more relaxing and pleasant feel that puts people at ease and implies more of a design flair. Technical requirements for the logo were that it should use only one or two colours that could be used as ‘brand colours’, and would work well for both print on a white background (catalogue and product flyer in keeping with P3 style) and for digital media (website and animated video). It was determined that the logo should include the product name ‘Tube Anchor’ but not an additional strapline, and use a readily available font that would retain its clarity down to 100×60 pixels.
Website
The web domain ‘tubeanchor.com’ was registered and a dedicated Tube Anchor website developed by CareTechnica using the Wordpress content management system. It consists of just a single page, including links to two videos, designed as a landing for people who might hear about the product and search on the web using the search term ‘tube anchor’.
Promotional videos
As Tube Anchor is a new technology rather than an improvement on an existing one, an animated visual explainer was commissioned. A basic story line and script was put together and refined and improved by a Bristol University medical undergraduate, also a talented artist and graphic designer. Using the People Per Hour website (peopleperhour.com) the job of creating the explainer was sent over to a designer at votostudios.com in Parlier, California, and a UK-based voiceover artist was commissioned to speak the dialogue. Background music was purchased from pond5.com (see online supplementary movie 1).
A manikin forearm, hand and wrist made of water clear polyester casting resin was made by one of us for a demonstration video showing several easy methods for inserting administration tubing into Tube Anchor (see online supplementary movie 2).
Production and packaging
The production environment used was clean rather than sterile, with manual addition of the adhesive backing. Packaging of a device significantly influences our perception of its function and cost. The investment required for a blister packaging line is substantial. Amortising the cost of attractive packaging into Tube Anchor would, however, increase its retail price and reduce trust cost savings from a reduction in recannulation costs. It is a complex trade-off between potentially undermining initial sales through the use of suboptimal packaging, and limited sales by postponing investment in packaging lines.
Marketing, sales and distribution
Our trust is one of approximately 150 foundation trusts in the UK (as of 2013) and has an annual operating budget of approximately £500 million. In the year ending March 2011, The Trust purchased almost 260 000 standard intravenous cannulae and just under 10 000 administration tubing giving sets. Similar devices are used throughout the UK and the rest of the world, creating a huge ‘market’ for Tube Anchor. The population of people with a professed interest in purchasing Tube Anchor (a.k.a. The ‘potential market’) is an extremely small fraction of the above, however, and can only be created by contact with sales people who are skilled at generating a perceived need for the device. Local restrictions on ward purchasing reduce the potential market still further to a very modest ‘available market’. The ‘target market’, the segment of the available market that the manufacturing and distribution partner pursues, needs to fulfil sales expectations for long enough to allow Tube Anchor to break even if it is going to become successful.
Introducing any new medical device can be challenging. Even when a new product offers a straightforward piece-part cost saving compared to an existing one, users are naturally resistant to change and risk averse. When a new device adds cost in exchange for efficiency or cost reduction elsewhere in the clinical pathway, the need to prove the ‘business case’ is overwhelming. Products that reduce trauma and complications or eliminate repeat procedures and readmissions are among the most difficult because the cost of failure is hidden away or in a different budget silo.
Establishing a sound business case is profoundly difficult and is a classic ‘Catch 22’. A good evidence base is required but is impossible to compile without sound data on usage. Getting usage is often impossible without the business case. Procurement will look to clinical staff for evidence and clinicians will point to Procurement. The only way this cycle can be broken is if a good champion emerges who is prepared to take on the challenge of helping to collect the evidence. Innovators themselves are often viewed with suspicion as they are not seen as independent. Manufacturers are often regarded as operating at the expense of rather than in close partnership with health service providers.
Many good innovations fail at this hurdle. Several organisations claim to be able to help, with NIHCE (the National Institute for Health and Care Excellence—often abbreviated to NICE) at the top of the tree. NIHCE themselves, however, also need an evidence base before conducting an assessment, so where could that evidence come from?
The landscape in England is further handicapped by the fragmented nature of procurement. Even a breakthrough in one hospital can mean little when the procurement process and the business case has to be repeated many times over elsewhere. The UK government has recognised this by launching its ‘Accelerated Access Review’ under Sir Hugh Taylor, amongst a number of initiatives targeting the same issue. George Freeman, the Life Sciences Minister, has used the term ‘Guided Runway’ for innovation and this is an incredibly worthwhile objective. A robust and simplified process for evaluation and evidence gathering would be a major benefit to the National Health Service (NHS) and to the economy and would be welcomed by all stakeholders involved in delivering sound and efficient patient outcomes, particularly those pursuing true innovation.
One obvious question is, if the UK is such a tough place to innovate, why not start overseas? The answer for UK-based companies is that few potential overseas customers will show much interest if a product has no track record of adoption in its own country. Some domestic use is almost always required.
Conclusions
The journey from medical device concept to bedside is often lengthy and after years of intellectual and financial investment there are no guarantees that costs will be recovered. By far the most important part of the jigsaw is to form an effective partnership with professionals whose knowledge base and skills dovetail, and who generate an open-minded and cooperative collaboration towards a shared goal. Patents and other forms of intellectual property are in many cases nothing more than a series of expensive locks fitted to rickety doors. It may be best to use nondisclosure agreements to limit ideas, designs, development and production to a small and trusted team who when ready to launch can make as much noise and fuss as publicity will allow using the war chest that would otherwise have been spent on intellectual property. If an idea is good, it will inevitably be copied, but once established as the originator of an invention, emulators may be less inclined to claim it as their own. Commercial success is a prerequisite if healthcare is going to have the opportunity to benefit from a new technology, but the primary goal of making our patients’ experience better needs to be kept centre stage. If brushed aside in a headlong commercial drive, propagation of the innovative process and the satisfaction to be derived from it may be diminished for all.
Acknowledgments
Rachel Clark, then innovations lead at The Trust and originator of the ‘Bright Ideas’ competition, without whose encouragement the prototypes for Tube Anchor (and VibraTip) would not have made it past the garden shed door. Dr Hassan Amrani, then research and development manager for P3, whose stock phrase ‘No Problem’ and business card, led to the critical connection with P3, and Dr Rich Purcell, now a junior doctor, whose graphics skills and generosity were entirely responsible for the video explainer.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online video 1
- Data supplement 2 - Online video 2
Footnotes
Competing interests AL reports that the purpose of the paper is to help and encourage others to move their innovative ideas forward. It is conceivable that readers may conclude that the rationale for the paper was to promote the device discussed.
Provenance and peer review Not commissioned; internally peer reviewed.