Article Text

Abstract
Objective To examine the ability of the criteria proposed by the WHO to identify pneumonia among cases presenting with wheezing and the extent to which adding fever to the criteria alters their performance.
Design Prospective classification of 390 children aged 2–59 months with lower respiratory tract disease into five diagnostic categories, including pneumonia. WHO criteria for the identification of pneumonia and a set of such criteria modified by adding fever were compared with radiographically diagnosed pneumonia as the gold standard.
Results The sensitivity of the WHO criteria was 94% for children aged <24 months and 62% for those aged ≥24 months. The corresponding specificities were 20% and 16%. Adding fever to the WHO criteria improved specificity substantially (to 44% and 50%, respectively). The specificity of the WHO criteria was poor for children with wheezing (12%). Adding fever improved this substantially (to 42%). The addition of fever to the criteria apparently reduced their sensitivity only marginally (to 92% and 57%, respectively, in the two age groups).
Conclusion The authors' results reaffirm that the current WHO criteria can detect pneumonia with high sensitivity, particularly among younger children. They present evidence that the ability of these criteria to distinguish between children with pneumonia and those with wheezing diseases might be greatly enhanced by the addition of fever.
Statistics from Altmetric.com
Pneumonia is still a leading disease in childhood in developing countries.1 2 The WHO has developed guidelines, based on simple clinical signs, for the identification and treatment of pneumonia in developing countries.3 4
Despite widespread recognition that the WHO case management strategy has helped to reduce mortality,5 there is concern that children with non-severe pneumonia are still receiving antibiotics unnecessarily. Studies have reported a lot of antibiotic treatment failure for pneumonia in children with wheeze,6 7 suggesting they constitute a special group requiring a separate management algorithm.7 8
We examined the ability of the WHO criteria to identify pneumonia among cases presenting with wheezing and how adding fever to these criteria altered their performance.
Patients and methods
We analysed data from a prospective study on children living in São Paulo, Brazil. Details of the clinical data have already been published.9
What is already known on this topic
▶ WHO criteria to diagnose pneumonia in children (cough or difficulty breathing plus tachypnoea) are sensitive to identify pneumonia among children with acute respiratory infection, particularly those with upper respiratory infection.
▶ The same WHO criteria are not sensitive to identify pneumonia among children with acute respiratory infection and wheeze.
What this study adds
The addition of fever to such WHO criteria greatly enhances their ability to identify pneumonia among children presenting with wheezing.
Study population and diagnostic definitions
Children aged between 2 and 59 months presenting to the paediatric emergency departments of five public hospitals in a 15-month period were screened by a paediatrician upon arrival. Children with acute lower respiratory tract disease (LRTD) (wheezing, rales, tachypnoea, and/or dyspnoea were considered to be signs of LRTD) whose parents gave informed consent, were recruited into the study, excluding those with: recent history of aspiration (liquid or foreign body); tuberculosis; measles; pertussis; congenital, inherited, neurological, neuromuscular or immunological diseases; cancer; or gastro-oesophageal reflux.
LRTDs were classified as follows:
▶ Pneumonia: pulmonary infiltrate on chest x-ray (CXR) plus history and clinical findings of fever and/or respiratory complaints
▶ Acute bronchitis: cough and sputum after an upper respiratory tract infection (URTI) of less than 3 weeks' duration, without wheezing and no previous diagnosis of asthma
▶ Acute bronchiolitis: cough, breathlessness, tachypnoea, wheezing, crepitations and pulmonary hyperinflation on CXR, following URTI in children aged <2 years
▶ Wheezing: children with their first or second episode of wheezing, without other characteristic signs or symptoms
▶ Recurrent wheezing: children with wheezing and with a history of at least two similar episodes in the past.
Data collection
Children were prospectively recruited into the study when a full clinical history was taken and a thorough examination was performed by a paediatrician. Those with respiratory distress received appropriated medical care (ie, salbutamol) before examination. Respiratory rate was assessed twice by observing the thorax for 60 s when the child was awake, calm and without fever (nurses assessed their temperature and, when necessary, gave them an antipyretic before examination). CXRs were taken for all suspected cases of pneumonia and acute bronchiolitis, and when exclusion criteria needed investigation.
Using the history and clinical findings recorded by the paediatrician and the CXRs, a paediatric chest physician recorded a diagnosis for each child, blinded to the paediatrician's diagnosis. The CXRs were evaluated by a paediatric radiologist, blinded to any other data. For children with a CXR the final diagnosis was that agreed by two of the above professionals and, in the absence of a CXR, was that given by the examining paediatrician (figure 1).

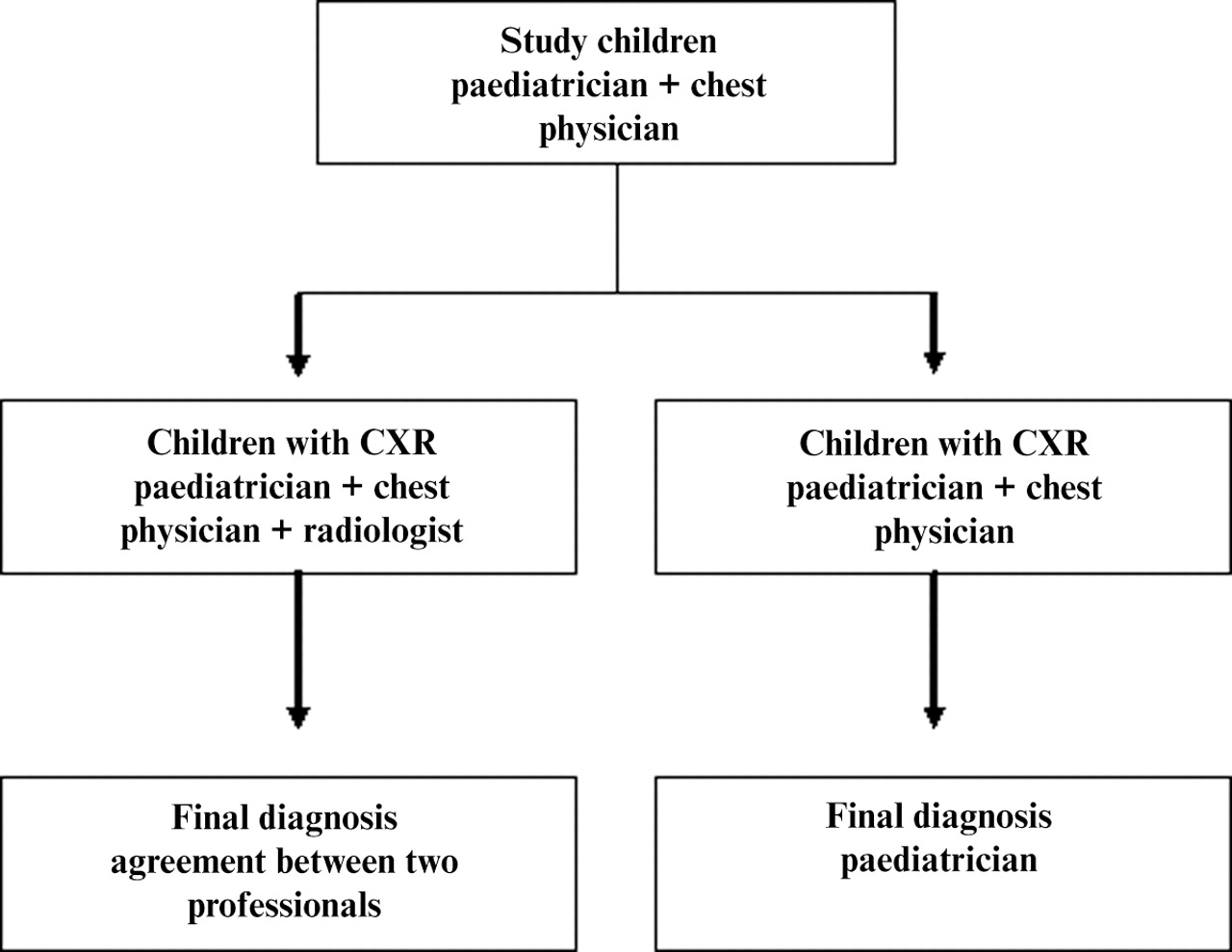{kind=link}
Flowchart for the diagnosis of pneumonia.
The study protocol was approved by the institutional Ethics Committee.
Analysis
In addition to the diagnoses they received according to the criteria described above, children were classified as with or without pneumonia according to WHO criteria (rapid breathing or lower chest indrawing).3
We also examined a modification to the WHO criteria by adding mother's report of fever or presence of fever (axillary temperature ≥37.5°C3) on admission (WHO criteria+fever). The sensitivity and specificity of the original WHO criteria and of the WHO criteria+fever for the diagnosis of pneumonia were calculated, taking radiographic diagnosis of pneumonia as the gold standard.
Results
A total of 410 patients were examined and 20 were excluded because of gastro-oesophageal reflux, sickle cell disease, HIV positivity and lack of data on breathing pattern. CXRs were available for 153 of the remaining 390 children. A total of 167 (43%) children were aged between 2 and 11 months, 98 (25%) were between 12 and 23 months and 125 (32%) were between 24 and 59 months. The male:female ratio was 1.38:1.
Diagnoses were acute bronchitis in 28 (7%) children, acute bronchiolitis in 7 (2%), wheezing in 117 (30%), recurrent wheezing in 168 (43%) and pneumonia in 70 (18%) (15 of them with recurrent wheezing). Agreement between the paediatricians' and the paediatric chest physicians' diagnoses was high (κ=0.86, 95% CI 0.82 to 0.90).
The validity of WHO criteria with and without fever is presented in table 1. When only children with a CXR were considered in the analysis, WHO criteria showed similar sensitivity to WHO criteria+fever (84%, 95% CI 73% to 92% vs 81%, 95% CI 70% to 90%) but lower specificity (14%, 95% CI 8% to 24% vs 33%, 95% CI 23% to 45%).
Sensitivity and specificity of the WHO criteria (±fever) for detecting pneumonia by age
We also examined the performance of both sets of criteria in children with and without wheezing at the physical examination, both sets of criteria being more specific in children without wheezing (table 2).
Sensitivity and specificity of the WHO criteria (±fever) for detecting pneumonia according to the presence or absence of wheezing
Discussion
Our results indicate that WHO criteria have high sensitivity to detect pneumonia, particularly among children aged <24 months. Their specificity, however, was low in all age groups and very poor in wheezing children. Adding fever to the WHO criteria improved specificity substantially, with very little loss in sensitivity, avoiding the risk of undertreating children with pneumonia.
The diagnostic criteria used in this study were standardised and compliance with them was carefully evaluated.9 All children were walk-in patients without referral from primary healthcare clinics, and thus represented cases of community-acquired pneumonia in the whole city. Proportionally, recurrent wheezing was most common during the summer with the incidence of infectious respiratory diseases (acute bronchitis, acute bronchiolitis or pneumonia) and wheezing peaking in winter.
In the 1990s, several studies examined the validity of WHO guidelines for detecting childhood pneumonia.10,–,15 However, these investigations excluded wheezing children and reveal that WHO criteria are sensitive and specific only for distinguishing pneumonia from URTIs, and concerns have been raised over the unnecessary use of antibiotics in cases of non-bacterial disease.16,–,19 Aiming at rationalising the use of antibiotics in children with wheeze, the WHO recommended a trial of rapid-acting bronchodilator in children with audible wheeze and fast breathing and/or lower chest indrawing before diagnosing pneumonia.4 Hazir et al8 identified fever, no family history of wheezing, and lower chest indrawing as predictors of subsequent deterioration in children with wheeze and fast breathing and/or lower chest indrawing who responded to inhaled salbutamol. In another study,20 CXRs of children diagnosed with non-severe pneumonia using WHO guidelines were analysed and showed radiographic evidence of pneumonia in only 14% of the 1848 CXRs examined. According to El-Radhi et al,21 fever has been the best predictor of bacterial infection. Other studies, focusing on factors influencing pneumonia treatment outcome, reported that clinical failure was significantly higher in children presenting with wheezing on examination.22
Surprisingly, a recent paper by Ayieko and English23 reviewed the evidence supporting WHO case management of pneumonia but did not address the problem of wheezy children or mention any of these studies in which fever appeared to be a clinical sign worthy of evaluation. However, a subsequent review by Graham et al7 states that the “case-management strategy assumes that the presentation of fever and cough with fast breathing means that the child has pneumonia and requires an antibiotic”. These authors, on the other hand, stress the need for a specific management algorithm for children with wheeze.
We analysed the subgroup of children without wheezing, obtaining a specificity of 62%, similar to that reported from studies which excluded wheezing patients.10,–,15 However, for children with wheezing, the specificity of the WHO criteria dropped to 12%. The addition of fever to the WHO criteria appears to improve distinction between pneumonia and other LRTDs, particularly among wheezy children. In our study, fever whenever present was lowered before respiratory rate was assessed. This should have minimised misclassification as it is known that fever affects children's respiratory rate.24 In an urban middle income easy access setting, the evaluation of tachypnoea was recently found to be useful in the assessment of pneumonia among children without wheeze.25 In a similar setting, fever or history of fever at home was among the associated findings with pneumonia in wheezing children.26
It is necessary to emphasise that the WHO guidelines were intended to be used by healthcare workers, especially in rural areas.4 The patients studied here presented to urban paediatric emergency departments, likewise those studied in investigations with findings similar to ours.25 26 In areas where pneumonia still threatens childhood survival,1 2 it may be reasonable to overtreat pneumonia.
For ethical reasons, CXRs were taken only to confirm the paediatrician's diagnostic impression and to investigate other possibilities. Thus, it might be argued that a bias occurring when the CXRs were ordered could explain our findings. We investigated this possibility by looking at the signs/symptoms which led the paediatricians to request a CXR and by restricting our analyses to children with a CXR. A multivariate analysis (data not shown) indicates that several findings were associated with CXR performance: crepitations, difficulty breathing in a child <24 months old, fast breathing, fever, previous medical consultation and sickly appearance.
Finally, some weaknesses and strengths of this study should be highlighted. Radiographic evaluation is subjective and thus in this study the CXRs, when available, were evaluated by two independent observers. Clinical evaluation also has subjective aspects, however, having two independent clinical evaluations performed at the same time for each patient was not possible for ethical reasons. Nonetheless, objective parameters such as respiratory rate and wheezing auscultation were used in this study and this should have minimised the subjectivity of the diagnosis. This study involved children presenting to urban hospital settings rather than to health facilities in rural areas and this could limit the external validity of our findings as it can be difficult for healthcare workers to measure temperature in resource-poor settings. However, our definition of fever (axillary temperature ≥37.5°C or mother's report of fever) is compliant with the WHO definition3 4 and with common practice.27
Our results reaffirm that the current WHO criteria detect pneumonia with high sensitivity, particularly among younger children. They also present evidence that the ability of these criteria to distinguish between children with pneumonia and those with wheezing diseases might be greatly enhanced by the addition of fever.
Acknowledgments
The authors thank the participating families who made this study possible.
MRAC and CMNC are investigators of the Brazilian Council for Science and Technology Development (CNPq). CNPq had no role in handling or completing the research. The authors had full control of all primary data.
References
Footnotes
-
Funding This research was funded by the International Development Research Centre (IDRC) – Canada.
-
Competing interests None.
-
Ethics approval This study was conducted with the approval of the University of São Paulo.
-
Provenance and peer review Not commissioned; externally peer reviewed.