
Abstract
We investigated the relationship of visual impairment (VI) and age-related eye diseases with mortality in a prospective, population-based cohort study of 3,280 Malay adults aged 40–80 years between 2004–2006. Participants underwent a full ophthalmic examination and standardized lens and fundus photographic grading. Visual acuity was measured using logMAR chart. VI was defined as presenting (PVA) and best-corrected (BCVA) visual acuity worse than 0.30 logMAR in the better-seeing eye. Participants were linked with mortality records until 2012. During follow-up (median 7.24 years), 398 (12.2%) persons died. In Cox proportional-hazards models adjusting for relevant factors, participants with VI (PVA) had higher all-cause mortality (hazard ratio[HR], 1.57; 95% confidence interval[CI], 1.25–1.96) and cardiovascular (CVD) mortality (HR 1.75; 95% CI, 1.24–2.49) than participants without. Diabetic retinopathy (DR) was associated with increased all-cause (HR 1.70; 95% CI, 1.25–2.36) and CVD mortality (HR 1.57; 95% CI, 1.05–2.43). Retinal vein occlusion (RVO) was associated with increased CVD mortality (HR 3.14; 95% CI, 1.26–7.73). No significant associations were observed between cataract, glaucoma and age-related macular degeneration with mortality. We conclude that persons with VI were more likely to die than persons without. DR and RVO are markers of CVD mortality.
Similar content being viewed by others

Introduction
With aging populations, age–related eye diseases and visual impairment (VI) pose substantial public health issues1. VI can lead to functional disability2,3,4, loss of independence5, reduced social interaction, depression6, accidents7, falls8 and fractures9. In addition, as visual acuity is a reflection of one’s functional status and ocular health, the presence of VI may also be a marker of frailty and may hence predict mortality10. Several population-based studies have shown a possible link between VI with increased mortality11,12,13,14,15,16,17,18,19. However, there have only been few studies in Asian populations20,21,22, who have different patterns of eye diseases, systemic risk profiles, healthcare knowledge and access to care23.
The presence of age-related eye diseases such as cataract, diabetic retinopathy (DR) and age-related macular degeneration (AMD) has also been postulated to be associated with increased mortality risk15,18,19,22. The severity of DR, for example, may reflect systemic vascular risk24. AMD shares common risk factors with mortality and cardiovascular diseases (CVD)25,26,27,28,29,30,31. Similarly, retinal vein occlusion (RVO) has been associated with increased vascular risk and mortality32,33,34. However, the relationship between specific age-related eye diseases with mortality in population-based studies has been mixed. While some studies have reported associations between cataract15,18,19,20,22,35, AMD15 and DR18,19,22 with mortality, others have not found independent relationships12,16,18,19,22,36. In addition, only few studies have been conducted in Asia20,21,22 in which AMD and glaucoma, in particular, have different clinical features and possibly underlying pathogenic mechanisms37,38,39,40.
Age-related eye diseases and VI is likely to increase substantially in Asia in the next few decades41,42,43. In this study, we describe the relationship of VI and major age-related eye diseases with all-cause and CVD mortality events in a population-based cohort of Asian Malay persons.
Methods
Study population
The Singapore Malay Eye Study is a population-based, cohort study, in which 3280 (response rate 78.7%) urban Malay adults aged 40 to 79 years living in Singapore were examined between August 2004 and June 2006. Study design and population details have been described elsewhere44. A total of 3273 participants were included in this analysis as visual acuity could not be successfully measured in 7 participants. All study procedures were performed in accordance with the tenets of the Declaration of Helsinki as revised in 1989. Written informed consent was obtained from the subjects and the study was approved by the Singhealth Centralised Institutional Review Board (CIRB approval number R1107/9/2014). Participants underwent a standardized interview, systemic and ocular examination and laboratory investigations at baseline.
Assessment of visual impairment
Presenting visual acuity (PVA) (with participants wearing their glasses or contact lenses, if any) and best-corrected visual acuity (BCVA) (with subjective refraction conducted by certified optometrists) were measured using the logMAR number chart (Lighthouse International) at a distance of 4 m. If no numbers were read at 4 m, the participants were moved to 3, 2, or 1 m, consecutively. If no numbers were identified, visual acuity was assessed as counting fingers, hand motions, light perception, or no light perception. BCVA and PVA were used in our analysis, although PVA is likely to be more relevant in the practical setting as this reflects the “true” visual acuity of the study population in their daily activities of living. VI was defined as greater than 0.30 logMAR in the better-seeing eye (US definition)45.
Assessment of age-related eye diseases
Complete ophthalmic examinations of the anterior segment, fundus and optic discs were conducted at the slit lamp using standardized protocols. Cataracts were assessed from lens photographs using the Wisconsin Cataract Grading System46 and defined as nuclear cataract opacity 4 or greater, cortical cataract 25% or greater, posterior subcapsular cataract 5% or greater, or previous cataract surgery. Glaucoma was diagnosed and classified using the International Society Geographical and Epidemiological Ophthalmology scheme based on gonioscopy, optic disc characteristics, and/or visual fields results47. The presence of DR was graded from retinal photographs according to a modification of the Airlie House classification system as used in the Early Treatment Diabetic Retinopathy Study48. The presence of AMD was graded from retinal photographs according to the Wisconsin Age-Related Maculopathy Grading System49. Recent central retinal vein occlusion (CRVO) was characterized by retinal edema, optic disc hyperemia or edema, scattered superficial and deep retinal hemorrhages and venous dilation. Old CRVO was characterized by occluded and sheathed retinal veins, or vascular anastomosis at the optic disc50,51. Branch retinal vein occlusion (BRVO) involved a more localized area of the retina in the sector of the obstructed venule and was characterized by scattered superficial and deep retinal hemorrhages, venous dilation, intraretinal microvascular abnormalities and occluded and sheathed retinal venules50,51. The presence of any retinal vein occlusion (RVO) was defined as presence of CRVO or BRVO.
Assessment of other risk factors
Participants underwent a standardized interview for socioeconomic measures (eg, income, education, type of housing), lifestyle risk factors (eg. smoking), medication use and self-reported history of systemic diseases. Non-fasting venous blood samples were collected for analysis of cholesterol and glucose levels. Hypertension was defined as systolic blood pressure of 140 mm Hg or higher, diastolic blood pressure of 90 mm Hg or higher, or use of antihypertensive medication. Diabetes was defined as a random glucose level of 200 mg/dL (to convert to millimoles per liter, multiply by 0.0555), use of diabetic medication, or a physician’s diagnosis of diabetes. Body Mass Index (BMI) was defined as body mass (kg) divided by the square of the height (m2). History of CVD was ascertained through self-reporting (yes or no).
Assessment of mortality
The unique national registration identity card numbers, together with date of birth and gender, of the 3273 members of the original cohort were matched with mortality records maintained by the National Registry of Diseases Office of Singapore (NRDO). Vital status as of 31 December 2012 was determined for all of the participants. Information on the date of death, all-cause deaths and CVD deaths for the participants were extracted. The underlying cause of death was reported using the International Classification of Diseases 9 codes.
Statistical Analysis
Time-to-event was calculated for each participant from the date of examination where visual acuity was measured through December 31, 2012. Cox proportional hazard regression was used to investigate the associations of PVA, BCVA, age-related eye diseases and mortality. We constructed 2 multivariable models: 1) adjusted for age and gender; and 2) adjusted for age, gender, socio-economic status, hypertension, smoking, diabetes, BMI and history of CVD. This permits the evaluation of specific ocular diseases and VI on survival while controlling for other risk factors. Finally, each specific ocular condition was added to the model to determine its independent effect on mortality. Hazard ratios and 95% confidence intervals (CI) were presented for stratified PVA and BCVA groups. We regard P values of <0.05 from 2-sided tests to indicate statistical significance. We further tested the interaction between DR and VI with mortality by including cross-product interaction term as independent variable (i.e. DR*VI) in the model. Statistical interactions were deemed significant if the P value for interaction was <0.1, All statistical analyses were performed using STATA version 12.
Results
Baseline Characteristics
In total, 3273 participants were included. Of these, 992 (30.3%) met the definition of VI using PVA and 360 (10.9%) met the definition of VI using BCVA.
Table 1 shows the baseline characteristics of participants according to their PVA in the better-seeing eye. Persons with VI tended to be females, have lower socioeconomic status, lower BMI and have a history of CVD, hypertension, diabetes, glaucoma, cataract, retinopathy, AMD and RVO. Supplementary Table 1 compares the baseline characteristics of participants who met the criteria of VI by PVA but not by BCVA and participants with VI by PVA and BCVA. Persons with VI by both PVA and BCVA tended to be older, have lower socioeconomic status, lower BMI and have a history of CVD, hypertension, diabetes, cataract and late AMD.
Visual impairment and mortality
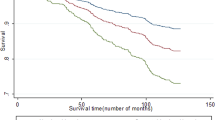
By December 31, 2012 (median follow-up 7.24 years), 398 (12.2%) persons had died in the SiMES cohort. In Cox proportional-hazards models adjusting for age, gender, socioeconomic status, hypertension, diabetes, smoking, BMI and history of CVD, participants with VI (based on PVA) had a higher all-cause mortality rate (hazard ratio [HR], 1.57; 95% confidence interval [CI], 1.25–1.96) and CVD-mortality (HR 1.75; 95% CI, 1.24–2.49) than participants without VI (Table 2). Persons with VI in terms of presenting VA (VA > 0.30) had poorer overall survival (Fig. 1) and higher CVD-cause mortality, compared with those without (Fig. 2). Similarly, persons with VI in terms of BCVA had higher all-cause and CVD-cause mortality. The results were similar when the WHO cut-off for visual impairment (VA < 6/18 in better-seeing eye) was used for presenting and best-corrected VA (Supplementary Table 2).

Survival curves for all-cause mortality according to better-eye presenting visual acuity categories, adjusted for age, gender, socio-economic status, diabetes, hypertension, smoking status, BMI and cardiovascular disease.

Survival curves for CVD-cause mortality according to better-eye presenting visual acuity categories, adjusted for age, gender, socio-economic status, diabetes, hypertension, smoking status, BMI and cardiovascular disease.
Age-related eye diseases and mortality
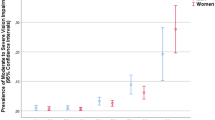
In terms of specific age-related eye disease (Table 3), DR was associated with increased risk of all-cause (HR 1.70; 95% CI, 1.25–2.36) and CVD (HR 1.57; 95% CI, 1.05–2.43) mortality. Participants with DR had poorer survival due to all-cause mortality (Fig. 3) and CVD-cause mortality (Fig. 4) respectively. In addition, RVO was only associated with increased risk of CVD mortality (HR 3.14; 95% CI, 1.26–7.73) but not with all-cause mortality (HR 2.02; 95%CI, 0.91–4.63). None of the other major age-related eye diseases (i.e., cataract, glaucoma and AMD) was statistically significantly associated with mortality. In the stratified analysis (Supplementary Table 3), we found that the association between DR and all-cause mortality was stronger in subjects with VI (p-interaction = 0.035). However, no statistically significant interaction was found with CVD-cause mortality for DR and VI (p-interaction > 0.1).

Survival curves for all-cause mortality in subjects with and without diabetic retinopathy, adjusted for age, gender, socio-economic status, hypertension, smoking status, BMI and history of cardiovascular disease.

Survival curves for CVD-cause mortality in subjects with and without diabetic retinopathy, adjusted for age, gender, socio-economic status, hypertension, smoking status, BMI and history of cardiovascular disease.
Discussion
In this prospective population-based study, persons with VI were more likely to die than persons without VI, even while controlling for other clinical and socio-economical risk factors for mortality. In particular, DR and RVO were associated with increased risk of mortality, particularly CVD mortality.
Our finding that VI is associated with higher risk of mortality is consistent with that found in several studies in the Western population (Table 4)12,15,16,17,18,19 and three in Asian studies20,21,22. As the above population-based studies span across different ethnicities, it is now highly convincing that VI has a close linked relationship with mortality. There are some possible explanations to justify this. First, visual acuity is a reflection of functional status and ocular health. Previous studies have clearly demonstrated that VI leads to functional problems and can contribute to loss of independent mobility2,3,4,5, falls8, accidents7 and psychosocial implications such as depression6. These functional problems in turn may contribute to an increased risk of mortality. Second, VI can also be seen as being a marker of aging52 and therefore it is not surprising that with aging comes higher incidence of mortality. Having said that, studies have not directly proven a causal relationship between VI and mortality and thus the exact mechanisms for higher mortality rates associated with VI remain unclear. Our study adds to knowledge of the impact of VI not only on morbidity but also mortality. Reduction of VI such as cataract surgery may also be associated with a reduction in risk of mortality. For example, in the BMES, cataract surgery resulting in the correction of VI resulted in lower long-term mortality risk (HR, 0.55; 95% CI, 0.41–0.73)53. Further studies are essentially needed.
In our study, we also observed that major age-related retinal vascular conditions such as DR and RVO were associated with CVD mortality, even after adjusting for potential confounders. DR was also associated with higher risk of all-cause mortality. This positive association of DR with mortality is consistent with other cohort studies54,55,56. The ETDRS study also found that poor visual acuity was associated with mortality in type 1 diabetics, whereas worsening levels of DR was associated with increasing risk of mortality57. This is in line with the hypothesis that microvascular diseases such as retinopathy may reflect the macrovascular status in major organs such as the heart and kidney as they may share similar underlying pathophysiology58. The presence of DR has also been associated with other risk factors for CVD including hypertension and hyperlipidaemia59. When we performed interaction analysis, we found that the association between DR and all-cause mortality was stronger in subjects with VI, indicating that persons presenting with the coexistence of DR and VI were more likely to have increased risk of all-cause mortality. This further highlights the importance of prompt management of DR, which can be sight saving as well as life-saving. Vigilant screening for DR, which can be conveniently achieved in a non-invasive way by direct visualization of the retinal vessels of the eye and early diagnosis for RVO may therefore play an important role in risk stratification of CVD. In the presence of retinopathy, prompt management of the ocular condition as well as optimization of associated vascular risk factors will be beneficial in disease control and preserving vision, hence reducing VI, which has also been shown to increase risk of mortality as above. We did not find an association between glaucoma, AMD, cataract and increased mortality risk, which was similar to the negative findings in many other studies.
The strengths of this study include its large sample size, long follow-up and standardized diagnostic protocols for cataract, AMD, DR, RVO and glaucoma. To our knowledge, this is also the first study evaluating the association of VI, age-related eye disease and mortality in an Asian Malay population. Limitations of our study include the possibility of some of the results being due to chance as there are a large number of confounding factors involved and not all may be accounted for. Further studies are also needed to investigate if VI has a direct or indirect causal effect on mortality. Longer duration of follow up may also be useful in confirming these associations. We also did not have data on the time of onset of cataract and time of surgery, which may confound the relationship between the presence of cataract and mortality and whether cataract surgery had an effect on mortality risk.
In conclusion, persons with VI were more likely to die than persons without VI. The presence of DR and RVO were, in particular, markers of increased mortality and CVD risk.
Additional Information
How to cite this article: Siantar, R. G. et al. Impact of Visual Impairment and Eye diseases on Mortality: the Singapore Malay Eye Study (SiMES). Sci. Rep. 5, 16304; doi: 10.1038/srep16304 (2015).
References
Bourne, R. R. et al. Causes of vision loss worldwide, 1990–2010: a systematic analysis. Lancet Glob Health. 1, e339–49 (2013).
Chiang, P. P., Zheng, Y., Wong, T. Y. & Lamoureux, E. L. Vision impairment and major causes of vision loss impacts on vision-specific functioning independent of socioeconomic factors. Ophthalmology. 120, 415–22 (2013)
Lamoureux, E. L. et al. Vision impairment, ocular conditions and vision-specific function: the Singapore Malay Eye Study. Ophthalmology. 115, 1973–81 (2008).
Wang, X. et al. Health burden associated with visual impairment in Singapore: the Singapore Epidemiology of Eye Disease Study. Ophthalmology. 121, 1837–42 (2014).
Wang, J. J., Mitchell, P., Smith, W., Cummin, R. G. & Attebo, K. Impact of visual impairment on use of community support services by elderly persons: the Blue Mountains Eye Study. Invest Ophthalmol Vis Sci. 40, 12–19 (1999).
Tolman, J., Hill, R. D., Kleinschmidt, J. J. & Gregg, C. H. Psychosocial adaptation to visual impairment and its relationship to depressive affect in older adults with age- related macular degeneration. Gerontologist. 45, 747–53 (2005).
Ivers, R. Q., Mitchell, P. & Cumming, R. G. Sensory impairment and driving: the Blue Mountains Eye Study. Am J Public Health. 89, 85–87 (1999).
Lamoureux, E. L. et al. Visual impairment, causes of vision loss and falls: the Singapore Malay Eye Study. Invest Ophthalmol Vis Sci. 49, 528–33 (2008).
Ivers, R. Q., Norton, R., Cumming, R. G., Butler, M. & Campbell, A. J. Visual impairment and risk of hip fracture. Am J Epidemiol. 152, 633–9 (2000).
Klein, B. E., Klein, R., Knudtson, M. D. & Lee, K. E. Frailty, morbidity and survival. Arch Gerontol Geriatr 41, 141–9 (2005).
Thompson, J. R., Gibson, J. M. & Jagger, C. The association between visual impairment and mortality in elderly people. Age Ageing 18, 83–8 (1989).
McCarty, C. A., Nanjan, M. B. & Taylor, H. R. Vision impairment predicts 5 year mortality. Br J Ophthalmol 85, 322–6 (2001).
Wang, J. J., Mitchell, P., Simpson, J. M., Cumming, R. G. & Smith, W. Visual impairment, age-related cataract and mortality. Arch Ophthalmol 119, 1186–90 (2001).
Lee, D. J., Gomez-Marin, O., Lam, B. L. & Zheng, D. D. Visual acuity impairment and mortality in US adults. Arch Ophthalmol 120, 1544–50 (2002).
AREDS Research Group. Associations of mortality with ocular disorders and an intervention of high-dose antioxidants and zinc in the Age-Related Eye Disease Study: AREDS report no. 13. Arch Ophthalmol 122, 716–26 (2004).
Thiagarajan, M., Evans, J. R., Smeeth, L., Wormald, R. P. & Fletcher, A. E. Cause-specific visual impairment and mortality: results from a population- based study of older people in the United Kingdom. Arch Ophthalmol 123, 1397–403 (2005).
Freeman, E. E., Egleston, B. L., West, S. K., Bandeen-Roche, K. & Rubin, G. Visual acuity change and mortality in older adults. Invest Ophthalmol Vis Sci 46, 4040–5 (2005).
Knudtson, M. D., Klein, B. E. & Klein, R. Age-related eye disease, visual impairment and survival: the Beaver Dam Eye Study. Arch Ophthalmol 124, 243–9 (2006).
Cugati, S. et al. Visual impairment, age-related macular degeneration, cataract and long-term mortality. Arch Ophthalmol 125, 917–24 (2007).
Khanna, R. C. et al. Cataract, visual impairment and long-term mortality in a rural cohort in India: the Andhra Pradesh Eye Disease Study. PLoS One. 8, e78002 (2013).
Foong, A. W. et al. Visual acuity and mortality in a Chinese population. Ophthalmology 115, 802–7 (2008)
Wang, Y. X., Zhang, J. S., You, Q. S., Xu, L. & Jonas, J. B. Ocular disease and 10-year mortality: The Beijing Eye Study 2001/2011. Acta Ophthalmologica. 92 e424–8 (2014)
Wong, T. Y., Loon, S. C. & Saw, S. M. The epidemiology of age related eye diseases in Asia. Br J Ophthalmol. 90, 506–11 (2006)
Kawasaki, R. et al. Multi-Ethnic Study of Atherosclerosis. Is diabetic retinopathy related to subclinical cardiovascular disease? Ophthalmology. 118, 860–5 (2011).
van Leeuwen, R. et al. Blood pressure, atherosclerosis and the incidence of age-related maculopathy: the Rotterdam Study. Invest Ophthalmol Vis Sci. 44, 3771–7 (2003).
Wong, T. Y. et al. Age-related macular degeneration and risk of coronary heart disease: the Atherosclerosis Risk in Communities Study. Ophthalmology. 114, 86–91 (2007).
Cheung, C. M. & Wong, T. Y. Is age-related macular degeneration a manifestation of systemic disease? New prospects for early intervention and treatment. J Intern Med. 276, 140–53 (2014).
Fernandez, A. B. et al. Age-related macular degeneration and incident cardiovascular disease: the Multi-Ethnic Study of Atherosclerosis. Ophthalmology. 119, 765–70 (2012).
Wong, T. Y. Age-related macular degeneration and cardiovascular disease in the era of anti-vascular endothelial growth factor therapies. Am J Ophthalmol. 148, 327–9 (2009).
Sun, C., Klein, R. & Wong, T. Y. Age-related macular degeneration and risk of coronary heart disease and stroke: the Cardiovascular Health Study. Ophthalmology. 116, 1913–9 (2009).
Cackett, P. et al. Smoking, cardiovascular risk factors and age-related macular degeneration in Asians: the Singapore Malay Eye Study. Am J Ophthalmol. 146, 960–7 (2008).
Cugati, S. et al. Retinal vein occlusion and vascular mortality: pooled data analysis of 2 population-based cohorts. Ophthalmology. 114, 520–4 (2007).
Wong, T. Y. & Mitchell, P. The eye in hypertension. Lancet. 369, 425–35 (2007).
Wong, T. Y. & Scott, I. U. Clinical practice. Retinal-vein occlusion. N Engl J Med. 363, 2135–44 (2010).
West, S. K. et al. Mixed lens opacities and subsequent mortality. Arch Ophthalmol 118, 393–7 (2000).
Borger, P. H. et al. Is there a direct association between age-related eye diseases and mortality? the Rotterdam Study. Ophthalmology. 110, 1292–6 (2003).
Lim, L. S., Mitchell, P., Seddon, J. M., Holz, F. G. & Wong, T. Y. Age-related macular degeneration. Lancet. 379, 1728–38 (2012).
Chakravarthy, U., Wong, T. Y. & Fletcher, A. Clinical risk factors for age-related macular degeneration: a systematic review and meta-analysis. BMC Ophthalmol. 13;10–31 (2010).
Yanagi, M. et al. Vascular risk factors in glaucoma: a review. Clin Experiment Ophthalmol. 39, 252–8 (2011).
Flammer, J. et al. The impact of ocular blood flow in glaucoma. Prof Retin Eye Res. 21, 359–93 (2002).
Wong, T. Y. et al. Vision Loss Expert Group of the Global Burden of Disease Study. Prevalence and causes of vision loss in East Asia: 1990-2010. Br J Ophthalmol. 98, 599–604 (2014).
Jonas, J. B. et al. Vision Loss Expert Group of the Global Burden of Disease Study. Prevalence and causes of vision loss in Central and South Asia: 1990-2010. Br J Ophthalmol. 98, 592–8 (2014).
Keeffe, J. et al. Vision Loss Expert Group of the Global Burden of Disease Study. Prevalence and causes of vision loss in Southeast Asia and Oceania: 1990-2010. Br J Ophthalmol. 98, 586–91 (2014).
Foong, A. W. et al. Rationale and methodology for a population-based study of eye diseases in Malay people: the Singapore Malay Eye Study (SiMES). Ophthalmic Epidemiol. 14, 25–35 (2007).
Tielsch, J. M., Sommer, A., Witt, K., Katz, J. & Royall, R. M. Blindness and visual impairment in an American urban population: the Baltimore Eye Survey. Arch Ophthalmol. 108, 286–90 (1990).
Klein, B. E., Klein, R., Linton, K. L., Magli, Y. L. & Neider, M. W. Assessment of cataracts from photographs in the Beaver Dam Eye Study. Ophthalmology. 97, 1428- 33 (1990).
Shen, S. Y. et al. The prevalence and types of glaucoma in Malay people: the Singapore Malay Eye Study. Invest Ophthalmol Vis Sci. 49, 3846–51 (2008).
Wong, T. Y. et al. Prevalence and risk factors for diabetic retinopathy: the Singapore Malay Eye Study. Ophthalmology. 115, 1869–75 (2008).
Kawasaki, R. et al. Prevalence of age-related macular degeneration in a Malay population: the Singapore Malay Eye Study. Ophthalmology. 115, 1735–41 (2008).
Lim, L. L. et al. Prevalence and risk factors of retinal vein occlusion in an Asian population. Br J Ophthalmol. 92, 1316–9 (2008).
Mitchell, P., Smith, W. & Chang, A. Prevalence and associations of retinal vein occlusion in Australia. The Blue Mountains Eye Study. Arch Ophthalmol. 114, 1243–127 (1996).
Pathai, S., Shiels, P. G., Lawn, S. D., Cook, C. & Gilbert, C. .The eye as a model of ageing in translational research - Molecular, epigenetic and clinical aspects. Ageing Res Rev. 12, 490–508 (2013).
Fong, C. S. et al. Correction of visual impairment by cataract surgery and improved survival in older persons: the Blue Mountains Eye Study cohort. Ophthalmology. 120, 1720–7 (2013).
Kramer, C. K., Rodrigues, T. C., Canani, L. H. Gross, J. L. & Azvedo, M. J. Diabetic Retinopathy Predicts All-Cause Mortality and Cardiovascular Events in Both Type 1 and 2 Diabetes Meta-analysis of observational studies. Diabetes Care 34, 1238–44 (2011).
Cheung, N. et al. Diabetic retinopathy and the risk of coronary heart disease: the Atherosclerosis Risk in Communities Study. Diabetes Care 30, 1742–6 (2007).
Rajala, U., Pajunpaa, H., Koskela, P. & Keinanen-Kiukaanniemi, S. High cardiovascular disease mortality in subjects with visual impairment caused by diabetic retinopathy. Diabetes Care. 23, 957–61 (2000).
Cusick, M. et al. Associations of mortality and diabetes complications in patients with type 1 and type 2 diabetes. Early Treatment Diabetic Retinopathy Study report no. 27. Diabetes Care 28, 617–625 (2005).
Moreno, P. R. & Fuster, V. New aspects in the pathogenesis of diabetic atherothrombosis. J Am Coll Cardiol 44, 2293–2300 (2004).
Cheung, N., Mitchell, P. & Wong, T. Y. Diabetic retinopathy. Lancet 376, 124–36 (2010).
Author information
Authors and Affiliations
Contributions
R.G.S., C.C., C.M.G.C., E.L.L., P.M., A.T., T.Y.W. and C.Y.C. wrote the main manuscript text. P.G.O. prepared the tables and figures. K.Y.C. contributed mortality data from National Registry of Diseases Office of Singapore. All authors reviewed the manuscript.
Ethics declarations
Competing interests
The authors declare no competing financial interests.
Electronic supplementary material
Rights and permissions
This work is licensed under a Creative Commons Attribution 4.0 International License. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/
About this article

Cite this article
Siantar, R., Cheng, CY., Gemmy Cheung, C. et al. Impact of Visual Impairment and Eye diseases on Mortality: the Singapore Malay Eye Study (SiMES). Sci Rep 5, 16304 (2015). https://doi.org/10.1038/srep16304
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/srep16304
This article is cited by
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
