Article Text

Abstract
Introduction Several public policies were proposed to reduce the negative impact of COVID-19 pandemic. This work aimed to determine how a management model is capable of strengthening the community network, providing support, healthcare and channelling public government’s aid during COVID-19 pandemic situation.
Methods It is an intervention study that tested the effectiveness of a management model for both healthcare and essential goods access in a socially vulnerable neighbourhood called ‘Puente de Fierro’ in La Plata the capital of Buenos Aires State, Argentina, during the COVID-19 pandemic. Altos de San Lorenzo suburb area was considered as control group. Variables studied were: level of contagion and death due to the SARS-CoV-2 virus; access to food, medicine and other goods; strengthening of community networks; performance of government programmes in territory.
Results A new management paradigm was tested by moving essential goods towards the people, instead of making the people move to obtain those benefits. Accessibility to ‘Food Bag’ and ‘Food Bank’ were significantly increased, a reduction of contagion level and mortality rate for COVID-19 was achieved (2.3/100 000 vs 3.6/100 000 inhabitants in control area; and ‘fatality rate’ was 2.8% vs 3.6%, respectively). Support was also provided to installed in local stores virtual payment devices for food cards acceptance.
Conclusion The management model based in healthcare and goods and service supplies during COVID-19 pandemic reduced the negative impact of disease and its measures of isolation in socially vulnerable neighbourhoods.
- COVID-19
- Community Medicine
- Delivery of Health Care
- Health Care Quality, Access, and Evaluation
- Health Care Facilities, Manpower, and Services
Data availability statement
Data are available in a public, open access repository.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- COVID-19
- Community Medicine
- Delivery of Health Care
- Health Care Quality, Access, and Evaluation
- Health Care Facilities, Manpower, and Services
WHAT IS ALREADY KNOWN ON THIS TOPIC
There is no doubt that socially marginalised people become even more vulnerable in emergencies, due to their dependence on the informal economy, their inadequate access to social services or political, their limited capacities and opportunities to adapt to new situations, or to their lack of access to early-warning systems, technologies or health services. It should not surprise us then, why COVID-19 particularly affected the socially vulnerable population.
During the pandemic, governments have decreed strict quarantine and isolation measures, without addressing the special situations of some sectors of society that have marginal conditions.
It is in this sense that the present study was based on an intervention aimed at the management of social and health policies in vulnerable neighbourhoods.
WHAT THIS STUDY ADDS
This study implemented a new model of healthcare at the population level during pandemic situations, such as COVID-19; and established an innovative local management regarding the distribution of basic supplies among the socially vulnerable population living in extreme conditions of isolation due to quarantine.
The experience demonstrated that a model based of community organisation active participation (NGO participative tables), where the population decides about our behaviour, common measures, awareness and responses to the social and health challenges, was able to reduced not only infections and deaths due to COVID-19 but also guaranteed compliance of isolation measures established by the government in a socially marginalised population.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE AND/OR POLICY
Unfortunately, environmental conditions, pandemics, and social, economic and security conditions are becoming more and more frequent in the world and warrant installing quarantines more and more often. The COVID-19 pandemic has not been the first nor the last. The direct and indirect consequences (due to the restrictions imposed to avoid contagion) lead to the population being greatly affected, especially those with fewer economic or educational resources, and geographically isolated.
The intervention model, validated by this experience, might be applied in similar situations in the future, where certain communities may suffer prolonged isolation because of weather, natural disasters, pandemic or social reasons.
The management of healthcare based in continues epidemiological reports, in personalised the follow-up the health evolution of each member of the community, and in control of people circulation during quarantine, might be helpful in future pandemic situations.
Also, the way that essential goods were distributed in this experience can be used to provide special resources, such as food and medicines, to an isolated population.
Introduction
Socioeconomic inequality is a barometer that measures how certain members of a society are excluded from essential goods and services that improve their quality of life. This situation is from any point of view, unfair since, by the simple fact of having been born in a certain geographical, territorial, historical and cultural context; individuals will have different opportunities to access to drinking water, sewers, transportation, education, employment, worthy or healthcare. Unfortunately, these cycles of inequality tend to perpetuate through generations.
From this epidemiological perspective, these unfair situations obey a ‘Chinese box model’, which identifies communities not only based on their individual and social characteristics but also from the social territories where the community lives; strengthening the concept of ‘social determination of health’, established by critical social epidemiology Latin American thinking school.1
Although inequality has focused on its economic aspects, especially on income distribution; the way in which material resources are distributed is the true expression of inequality and exclusion. The subordination and exclusion of the socially vulnerable population in each region leads to increase migration (both inside and between countries), which it is later translates into settlements around large urban centres, where economic backwardness and poor living conditions are reflected.2
This concept of vulnerability usually refers to poverty, marginalisation, exclusion, but lack to reflect the dynamics of the true causes of these social disadvantages that lead a single person or a hole community to this unfair condition that favours the maintenance of stereotypes of disadvantaged groups.3
According to Kaztman,4 the vulnerability approach makes it possible to explain social disadvantages by establishing a relationship between two levels of analysis: the micro-social level, which analyses the behaviour of individuals and households; and the macro level that relates to organisations and institutions.
Therefore, the decisive dilemma is to understand popular cultures in connection with the conflicts between social classes, with the conditions of exploitation in which these sectors consume and produce.5
It should be recognised that vulnerability is not synonymous with poverty, it means that deficiencies and needs are transformed in a state of defencelessness, insecurity and exposure to risks, which makes a certain community and its members submerged in an unstable and dynamic situation, that depends on government assistance.6
This situation of vulnerability can arise or deepen in the face of unexpected adverse events, such as natural disasters or epidemics. The closest example to highlight this point is the COVID-19 pandemic, which has severely affected all countries in the world.7
In South America, high daily levels of COVID-19 contagion and deaths still persist. In Argentina, for example, 15% of the population was affected by the disease (more than 5 million cases) with more than 130 000 deaths since the beginning of the pandemic.8 Some sources place the country among the first 10 areas most affected in the world in terms of mortality. According to Office of Workforce Development, Argentina is second in Latin America in deaths caused by COVID-19 per million inhabitants.9 However, the analysis of excess mortality, which is the most complete indicator that measures the direct and indirect impact of the pandemic,10 shows that Argentina is the country in Latin America that had the least excess mortality (10.6%), only surpassed by Uruguay, placing it below the world average for excess mortality (14.3%). This difference in the indicators for mortality in the same country shows us not only the variety in the population composition of the countries when we compare it but also the existence of a heterogeneous regional epidemiological mosaic.
Since 21 March 2020, strict quarantine measures were decreed in Argentina, which includes limitations on the movement of people, avoiding to leave their home without a justify cause, impediment to the use of public transport, among other restrictions. This situation extended for 3 months, and then a progressive situation with selective restrictions was installed according to the different epidemiological contexts maintaining the limitations on the use of public transport, and unnecessary circulation.
This situation of ‘preventive and mandatory social isolation’ and its derivations as a result of the pandemic situation made visible and deepened the structural deficits of the vulnerable populations. Given that the spread of the virus requires close contact between people, it is in the areas with the highest population density where the risk is heightened and the greatest impact is expected.11 In this framework, the popular socially vulnerable neighbourhoods arise as great challenges for achieving compliance with sanitary measures, since one of the important limitations that affect the possibility of isolation is based on overcrowding, especially in the case of precarious settlements, poor housing conditions and lack of basic services.12
Furthermore, for a large part of the population, isolation means total income interruption, as most people depend on an informal economy. Thus, the interruption of informal jobs and sub-jobs, together with structural poverty, leads to the critical situation of not having the daily essential provision of food for survival. Likewise, the isolation, the lack of contact with friends, family and relatives, the inability to leave the home for long periods due to the prolonged quarantine, also has had a negative impact on the mental health of the population.13
In these, neighbourhoods considered vulnerable in Argentina, especially in the capital surroundings called ‘AMBA’ region, these same isolation restrictions are much more complex, difficult to overcome, with severe limitations in access to social assistance due to mapping design of the neighbourhoods, that complicates the distribution of goods and the access to essential services. It is in these adverse and disadvantaged contexts, where community resilience takes on value and social skills emerges as a real or potential resource linked to a durable network of relationships that facilitate certain actions of individuals who participate in society.14
Complying with the strict home isolation measures proposed by the different governments, such as that of Argentina, during COVID-19 pandemic is certainly easier when homes have adequate comfort, such as the possibility of isolating themselves from rain or inclement of the weather; control the temperature of the environment inside the home, have available of drinking water, have access to entertainment such as TV or game consoles for children; be connected via internet or phone; have a refrigerator to store food, or have enough money to request delivery of food or essential goods at home.
However, socially vulnerable populations lack a home with a solid building structure, the roofs and walls of their houses are usually made of sheet metal or cardboard, they have no floors, the water is obtained outside the home, there is no gas network, they are enable to maintain an acceptable temperature inside the house; with overcrowding situation since several family members live in the same environment (without internal divisions, no bedrooms, no living room or kitchen; everything is together) and certainly without possibilities for entertainment or communications. Food and other essential goods are obtained day by day, and people are forced to leave their homes to survive.
It seems easy from the desk of a political/health authority to request a strict quarantine from the population, but in socially vulnerable neighbourhoods with conditions are the ones that we described, it is simply impossible. Although these communities could contribute with valuable information in order to obtain better results, unfortunately they are not consulted or actively participate in the development of programmes that the state proposes to these vulnerable sectors of society.
‘Puente de Fierro’ is one of the most socially vulnerable neighbourhoods in AMBA. Popular awareness about how to care in pandemic situation goes through people’s own creations, elaborated and shared by oppressed sectors from a solidarity activity. And in those cultural forms created by these people, they recognise and verify their circumstances and their potential for action.15
The objective of this work is to apply an intervention model that involves actions that allow a socially vulnerable population such as the one that lives in the ‘Puente de Fierro’ neighbourhood; can access the benefits provided by the state (economic aid, food, medical care) near their homes. With these measures, it is expected that those inhabitants can better accomplish with preventive isolation measures, reducing the level of contagion and deaths caused by the COVID-19 pandemic.
Methodology
Location
The ‘Puente de Fierro’ neighbourhood is located in La Plata, south suburb sof the capital city of Buenos Aires State, in a square limited between streets no. 23 and no. 30 and between no. 85 and no. 90. From the initiative of the neighbours, during 2017, a survey among ‘Puente de Fierro’ homes was carried out by our university team. Information about sociodemographic and educational aspects was collected. At that time, the neighbourhood consisted of 45 blocks, with a total of 1077 households and 4055 inhabitants. Within the framework of this work, a new survey in 2021 was carried out to update that epidemiological data detecting 1330 households and 5968 inhabitants that integrated the neighbourhood during pandemic situation that were enrolled in the project.
This population was classified by National Statistical Bureau (INDEC) as low-income community with 41.2% of poverty and 13.2% of indigence levels.
A neighbourhood called ‘Altos de San Lorenzo’ was selected as ‘control’ since it is considered a similar population with exactly similar characteristics (40.3% of poverty and 12.8% of indigence) by the INDEC.
Period of Study
20 March to 31 December 2020.
Study team conformation
Professors and students from Faculties of Social Sciences, Health Science; Computer Science of the National Universities of Quilmes and La Plata in Argentina, were voluntarily recruited to participate in this project. Professionals from different disciplines, such as sociologists, geographers, doctors, computer scientists, economists, managers, were part of this study.
Intervention: model of care applied to population studied
The University staff group offered to Puente de Fierro population a model of care that included all type of actions destinated to help people to better support the quarantine and the state recommendations to remain home and inside the neighbourhood limits. In order to do so, our group organised with the people, the way how state aid (food, money, medicines) could be obtained from those inhabitants who need this help. That is why, regular personal trips to obtain food in Dade county stores (11 km away from the suburb; or to extract money from banks (none of them near the area)) were replaced by massive transport of food bags to be distributed from local transitory store, or by mobile bank located in the neighbourhood once a week. Also, a local network was developed in order to attend in situ, health problems, COVID-19 cases or to increase access to medicines need by the population. All these measures were performed in order to avoid population unnecessary movements outside the village.
Participation action research
The participation methodology used was based on the application of typical techniques of participatory action research (PAR) processes that promote critical and consensual analysis of reality through the active participation of the community and the social organisations within a stimulating, a transformative practice and a social change of the communities.16
The PAR was developed through a ‘permanent participatory territorial work round table’ originally called ‘Mesa de Trabajo Participativa Permanente’ (MTP), within the framework of the ‘Territorii method’ and an innovative device called ‘Participatory Scientific Agenda’ (PSA) with the neighbours, and referents of the social organisations of the popular neighbourhood Puente de Fierro, belonging to La Plata, the capital city of Buenos Aires Province in Argentina.17 Given government regulations, the MTP and PSA were developed in face-to-face and virtual mode. This last modality merited the development of tutorials in video format, as well as pilot tests in order to training people involved. In addition, permanent communication was established between the territorial work team and the referents, via telephone, web and WhatsApp groups.
Strategies and tools for the development of the management model
Strengthening of a neighbourhood network, linking, communicational, interinstitutional and intersectoral partners
The management model developed was fundamentally aimed to strengthening the weak community communication network already existing among the neighbourhood social organisations; towards to increase their empowerment and self-management capacity, and to optimisation of the organised neighbourhood response in terms of prevention, early warning and control of the COVID-19 pandemic situation.
Community Epidemiological Surveillance System (CESS) through the use of intervention techniques: development of a software for mobile telephony
Part of the strategy for consolidation of the community management model included the implementation of a Community Epidemiological Surveillance System (CESS) at the neighbourhood scale, which allows promoting self-protection (individual, group and community) against COVID-19, and at the same time reproduce this type of care in other problems of health and in other neighbourhoods of Argentina.
The CESS was based on the development of a software for mobile telephones freely and voluntarily accessible to the residents of the neighbourhood, which would not only provide messages of self-care and protection against COVID-19 but also warn about steps to follow in cases of suffering symptoms of illness, alert to positive cases, support assistance for the transfer of confirmed cases to assistance centres, monitor the movement of the population outside the limits of the neighbourhood or attend to the needs of medicines to guarantee the continuity of treatment of neighbours with chronic diseases (hypertension, diabetes mellitus, etc) in order to avoid severe complications and risk of life.
The development of the software took into account the observations and suggestions of the social referents and it was inspired by the PAR and the principles of popular education, which also made possible data collection on health problems, and identification of the population with higher risk of contagion.
Implementation of a Geographic Information System
Data processing and building of maps were carried out with the Geographic Information System tool contributing substantively to the CESS18 and to logistics within the neighbourhood. The information was extracted either from primary sources (references from social organisations, field censuses, surveys, MTP) or from secondary sources (RPPVAP Provincial Public Registry of Villas and Precarious Settlements, Google Earth, RRI Plan for Flood Risk Reduction by UNLP–MLP agreement).
A mobile phone app was performed and uploaded in volunteers of the community. This app was used to observe street mobilisation in the neighbourhood, based in results obtained in theses ‘cases’.
Construction and measurement of epidemiological-health indicators
Defined qualitative and quantitative epidemiological indicators were selected and related with the activities arising from the interaction between the different social actors from the neighbourhood of Puente de Fierro. The purpose was to establish a baseline or initial sociosanitary diagnosis to support future actions of the management model, as well as evaluate the impact of the changes achieved.
Population indicators were also measured in order to detect potential risk of COVID-19; to alert about COVID-19 impact on the health system and to weigh up the benefits obtained with neighbourhood network.
A survey performed household by household was carried out among the different members of the community, including general data such as age, sex, occupation, risks, pathologies and social aspects such as living conditions of the households, productive and working conditions, political–institutional capacities of the neighbourhood organisations and security issues. This survey was also performed at the end of the study to compared results obtained.
A cartography and spatial analysis were developed by dimension, with georeferencing each home and each institution of the neighbourhood.
The situational diagnosis was obtained not only through the survey of households but also from MTP (focus groups) and from interviews with key referents (from the social organisations) focusing on the homes of neighbourhood where exist currently structural social needs and on homes where needs were enhanced by the pandemic situation.
Main indicators used were access to food and essential goods; COVID-19 positive rate (positive cases each 100 000 inhabitants), and fatal rate (number of deaths each 100 000 inhabitants). Other parameters measured were street mobility and people’s isolation at home during quarantine.
Preparation of communication materials
Communicational products were designed and produced in graphic, sound and audiovisual language in order to contribute to the management model through: (a) the strengthening of the CESS based on communication to know, prevent and mitigate the effects of the COVID-19 pandemic; (b) the consolidation of the bonding and communication network at the neighbourhood level that promotes self-protection; and (c) the optimisation of the communicational, intersectorial network and link at the territorial scale, making the exchanges of inputs, products and services more efficient and effective.
Training
The training was a substantive tool for strengthening the communication and interaction network between the organisations' referents and members of the neighbourhood. The modality of contact was virtual with some meetings of face-to-face training when government regulations allowed it.
Training was carried out in: detection of COVID-19 cases and prevention of contagion; vaccines and health protection; preventive measures on other environmental health problems, construction, technological tools (computer workshops, cell phones and social networks); the ActuAR software application for mobile phones; data collection in homes, filling out forms, and in the management of social organisations.
Patients and public involvement statement
The participation of the community is implicit in the functioning of the care model proposed in this study. Participants (‘patients’) were involved from the very initial stage of the project since they participate from the design of the study though a technique called PAR that proposed the active participation of the community and the social organisations groups within transformative practice activities. Members of the community that participated in the study constituted the MTP ‘permanent participatory territorial work round table’, which is a framework of the ‘Territorii method’ element that helps to identified and execute an agreed agenda (called ‘PSA’) for each week, month and even the hole project. The neighbours themselves chose the actions to be followed by everyone in a consensual, coordinated and programmed manner.
The recruitment of the members of the community in the project was voluntary and free. Either NGOs member or neighbour was invited to join the ‘permanent decision table’. Previously, a meeting was held in order to explain the project, and the burden of time involved in participating of the experience. Every Friday, the ‘table’ took place in the Plaza place. Every member was invited to participate in the discussion of the agenda (the own members of the community lead the meeting with the facilitating support role of researchers). In each periodical meeting, it was analysed the development of the project, the degree of it progresses, the results obtained, the alerts and the advices provided to the community, news about the evolution of those patients affected, how goods provided by local, provincial and national governments, would be distributed and future actions.
After 1 year of project, several members of the community (NGOs referents) and participants of this project helped to disseminate not only the results but also the model of care performed in the experience. These community participants of the project helped to reply the experience in Florencio Varela suburbs, which is a socially vulnerable and marginalised population living in an excluded geographical area of Buenos Aires state.
Statistical analysis
All data analysis was conducted using SPSS V.24. Descriptive statistics were used to define the general characteristics and variables such us residence, access to food, banks and medicines; COVID-19 infection rate and deaths. These variables allowed to compare intervention group (inhabitants of ‘Puente de Fierro’) versus control group (‘Altos de San Lorenzo’ population). Qualitative data collected from ‘Territorii method’ were using Atlas.ti programme.
Results
About community and territorial initial situational diagnosis analysis
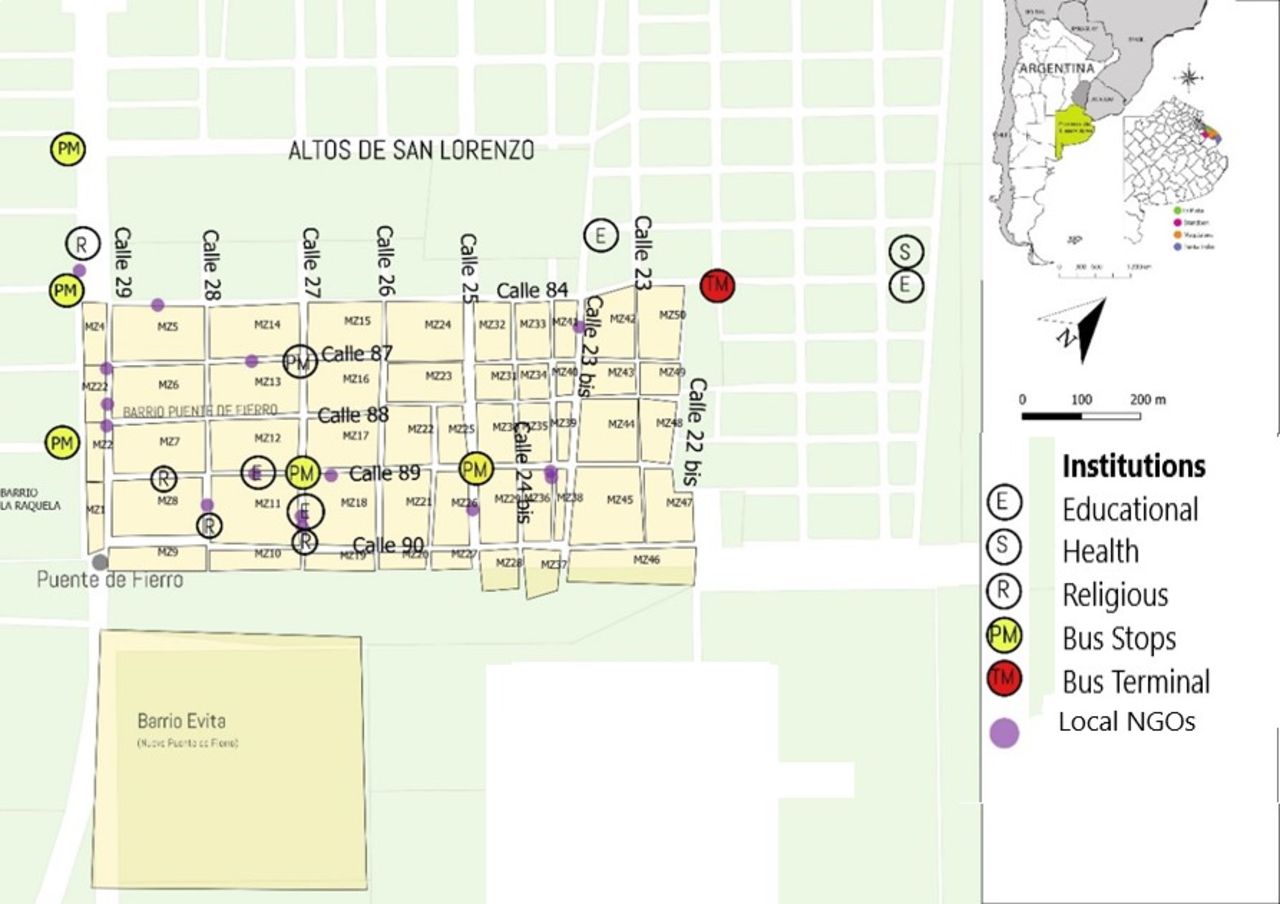
A territorial analysis was carried out through a cartography of the Puente de Fierro neighbourhood with its blocks, reference institutions and population density (figures 1 and 2).

Territorial analysis—Puente de Fierro neighbourhood.
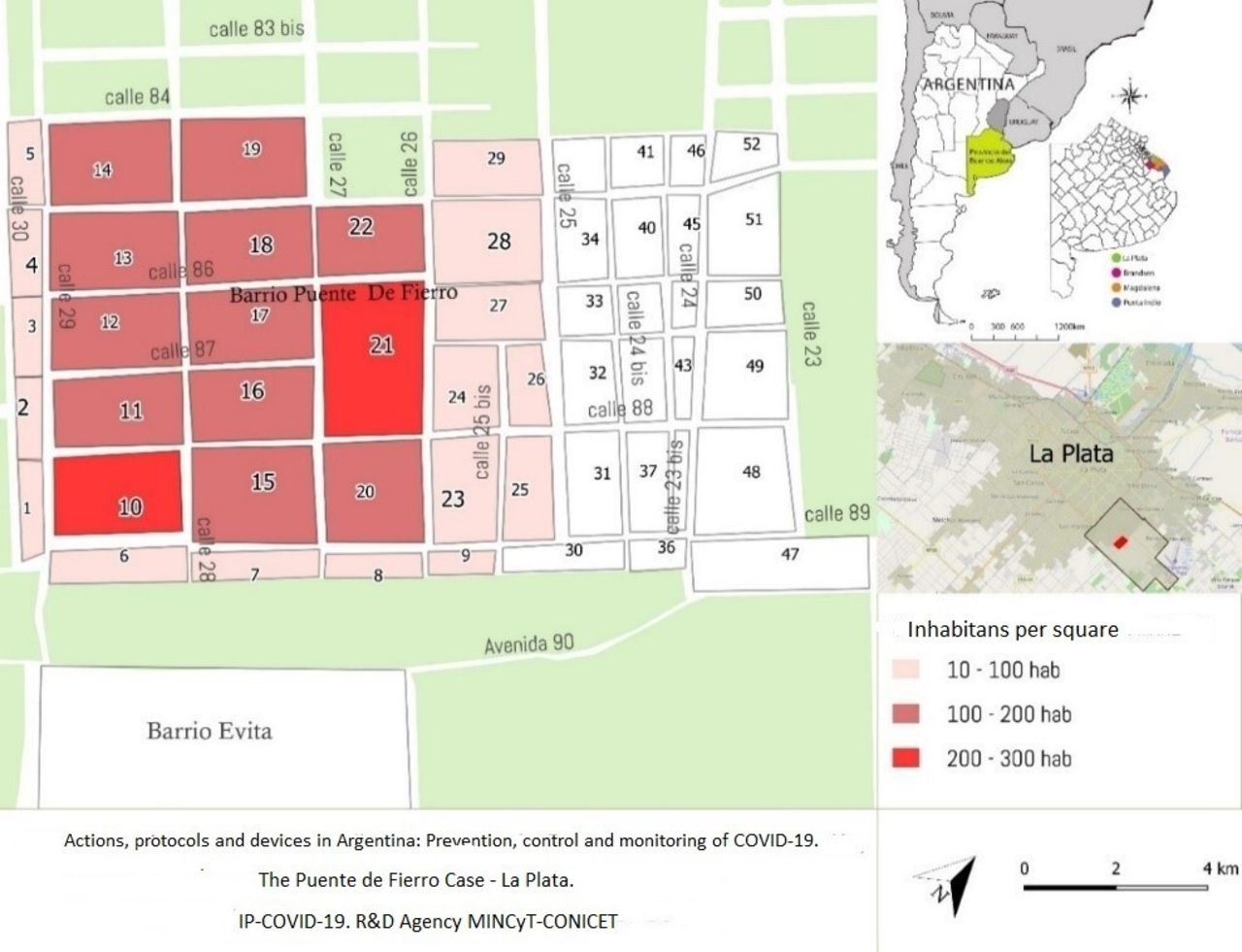
Inhabitants per block. Puente de Fierro neighbourhood.
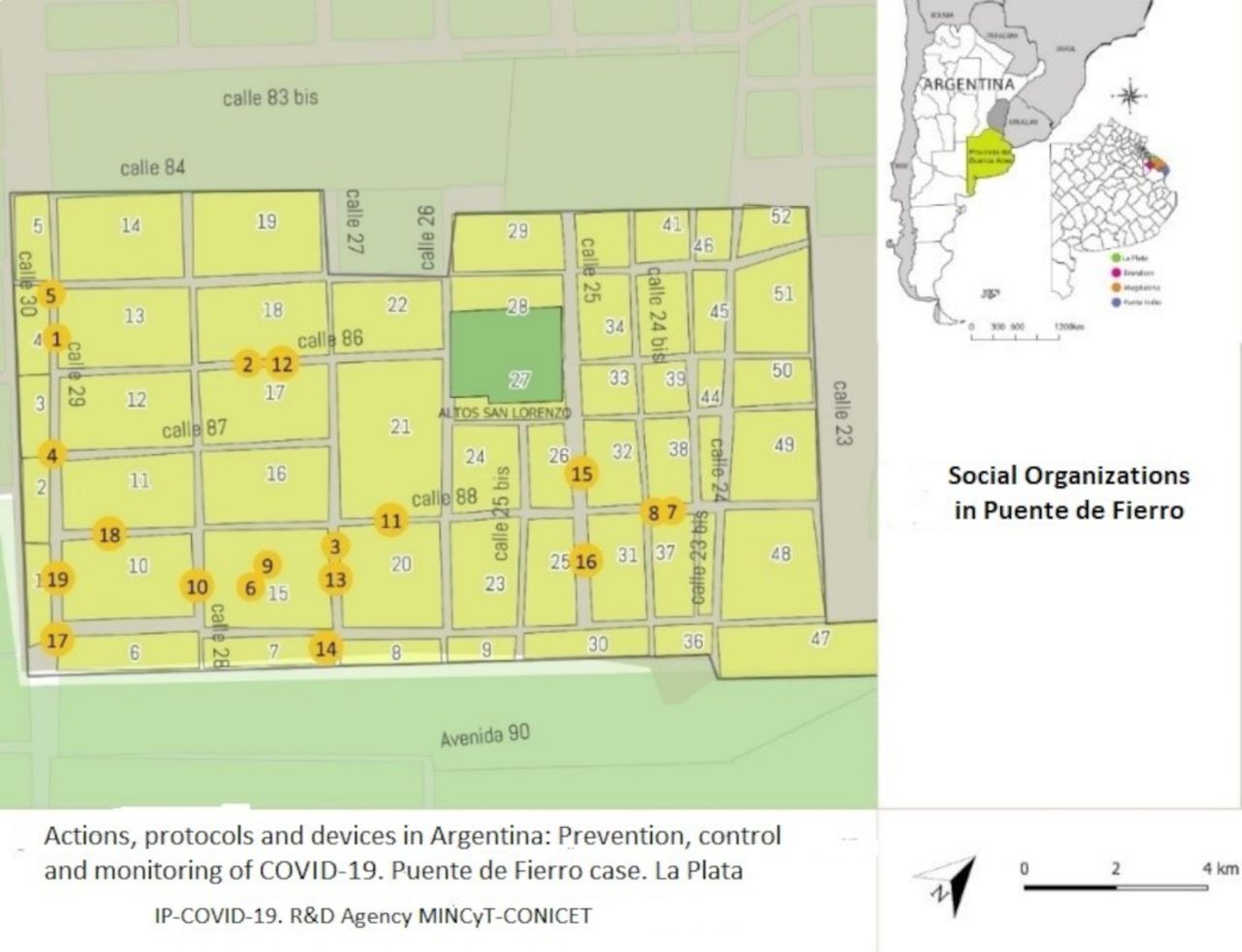
The neighbourhood organisations within the Puente de Fierro were included in the project and they accompanied the development and implementation of the management model and the consolidation of the self-care network (figure 3).

Neighbourhoodsocial organisations.
These organisations were: the ‘El Refugio Comedor y Guardería Civil Association’ with a presence in the neighbourhood since 1998; the ‘Cultural Center of Development and Work’ since 2000; the ‘María Claudia Falcone Organization’ since 2001; the ‘Movement of Civil Entities 31 March’ and the ‘Southern Region Civil Association’ since 2005; the ‘La Nueva Estrella School Support and Dining Center’ since 2006; the ‘Las Chaques Sports Group’ since 2012; ‘The Civil Association Amar a Nuestro Niños de Altos de San Lorenzo’; the ‘Los Hermanos Dining Room’; the ‘Los Chicos del Puente’ dining room and the ‘Integrative Neighborhood Center La Patriada’ since 2018; and other social organisations in the neighbourhood that worked together with the project, but with less participation: ‘CTD Aníbal Verón’; ‘Agrupación La Cámpora’; ‘Sowing Hope Group’; ‘Justice and Freedom Movement’; ‘Los Angelitos Dining Room’; ‘Bolivian Plurinational Community’; ‘8 October JD Peron’ group. All of these neighbourhood organisation were integrated ‘the Neighborhood Assembly’ (figure 3).
The restrictions imposed by the government, in the context of the COVID-19 pandemic, severely limited the possibilities of the caregivers to circulate freely on public roads. Hence, the limitations of the members of Puente de Fierro Community to free circulation was significantly affected even the usual contact between families inside the neighbourhood, the normal functioning of non-governmental social organisations (NGOs) and the community communication in certain situations (such as the presence of symptoms or signs of COVID-19 in some family member).
The interviews carried out, as part of the PAR techniques, revealed the multiple inequalities and the difficulty of complying with the main measures of care in the pandemic.
‘It’s easy to say stay at home and wash your hands,’ but in a little a poor home with only 4 wall and no floor, that has six boys, with only one water-tap, is hard. If you don't provide what is necessary to the children, it is very difficult to stay indoors and follows the government slogans like… wash your hands, stay inside… Our family members integrate the Emergency Committee, making the popular pots, trying to distribute the public resources with justice. We are talking about basic need such as eating, cleaning, soap and bleach. You have to live here to understand us. RF. Woman, 63 years old, member of a Civil Association of the Puente de Fierro neighbourhood
This situation of quarantine and prolonged isolation affected the normality of community activities, since there was a lack of coordination of actions between the local health authorities, their social help and support with people living in the neighbourhood.
Actions carried out to strengthen neighborhood social networks
One of the first strategies, developed to accomplish with the objectives of the study, was to strengthen the networks that already existed in an incipient way in the neighbourhood in which the ‘intervention’ was carried out.
With the members of the ‘Puente de Fierro’ organisations and professor and student from the National Universities, a ‘permanent participatory territorial work round table’ (MTP) was held in order to agree common guidelines for the prevention of COVID-19. In this MTP, several actions were developed.
Connectivity between members of MTP was assured by promoting programmed virtual meetings. In this sense, personal computers and mobile phones were provided by our team to each organisation (NGO). The app developed by the university was uploaded in those phones and computers. Leaders of NGO were responsible to share the app with each member of the team.
Specific trainings were generated to provide a rapid response to suspected or positive cases of COVID-19 as well as to other problematic situations. Guidelines were agreed for the transfer of NGO members requiring medical assistance.
It was planned a fare distribution and exchange of food and essential goods between organisations to attend to those members of the community temporarily most affected.
It was created a network to provide medicines to patients with chronic diseases who had lack of treatment and had no access to these goods. These treatments were delivered to each home of those members of the community who needed them, in order to guarantee the treatment continuity.
The Permanent participatory territorial work round tables, as well as the active WhatsApp groups, allowed a permanent interaction between the neighbours and members of the project. A guard of 24 hours a day, 365 days a year was installed. In this way, the most important problems related to the pandemic and the emerging situation in the neighbourhood were promptly attended.
The topics covered in the MTPs round tables, as well as in the WhatsApp groups, were fundamentally oriented to the prevention, control and monitoring of COVID-19, and also to access to food.
From the MTPs and virtual communications, the most urgent and important problems, as well as the structural needs of the neighbourhood, were identified and agreed to take care of them. It should be noted that the health problems were not in the neighbourhood’s priorities at the beginning of the project, even in the context of a pandemic. The government regulations in this regard (quarantine) made visible other problems that were structural in themselves, such as precarious housing, lack of jobs, unstable popular economy and food deficit, that became people priorities. Due to the pandemic situation, all the usual structural problems in the neighbourhood were added to the ‘new’ health problems caused by COVID-19 and to the measures adopted to prevent contagion.
Based on the systematisation of the themes and agreements of the PSA and the MTP permanent round table work with neighbours and referents of social organisations, the planned actions were focused on the following structural needs: food, work; education, information and communication; neighbourhood urban infrastructure and healthcare and attention. They took on greater relevance from the milestone of the pandemic and the isolation measures that erupted with the informal economy and made visible the needs of: information and supplies for the prevention of COVID-19; supplies and equipment for community kitchens and common food areas; internet connectivity and lack technological tools to be connected with others in the contexts of a quarantine.
Of the total number of 725 systematised actions that were carried out by the project, the following ones were pondered:
One hundred and fifty-six actions, were destinated to mitigate the need for education, information and communication
One hundred and twenty-four actions were used to mitigate the need for healthcare and attention.
Ninety-seven actions were focused on ‘neighbourhood urban infrastructure’ needs.
Sixty-five actions were used to mitigate the need for lack of daily food.
Forty-eight actions were destinated to help people with lack of job.
In addition:
One hundred and five actions were focused on the needs associated to pandemic restrictions such as providing supplies and equipment for ‘communal kitchen’ and ‘free food areas’.
Ninety-eight actions were used to mitigate the needs associated to COVID-19 information and lack of supplies for COVID-19 prevention.
Nineteen actions were used to mitigate the lack of technological tools to communicate and interacts with other members of the community.
Thirteen actions were destinated to attend the needs related to the lack of internet connectivity in the neighbourhood.
The referents agreed on the importance of social organisation and the union to face the common difficulties of the pandemic in a context of high social and environmental vulnerability.
We realized with the referents who we interact for many years, that unity is our strength and that if we all get together in the same cause, the neighborhood will move forward. This project has demonstrated us the advantages of the union, here in Puente de Fierro.
More popular pots and communal kitchen remained open during pandemic. To have more continuous operation than we had before due to the great demand of needs, we had to better organized food distribution. We organized ourselves with other communal kitchen, so that there is at least one of them open every day. Woman, 38 years old, referent to the social organization of the Puente de Fierro neighborhood
Access to food
The Argentine state, in order to mitigate the social and economic effects of the pandemic, created new social aid tools and increased the ones that already exist. Social support for families was strengthened through the programmes: ‘Emergency Family Income’ (‘IFE’); Emergency Assistance to Work and Production (‘ATP’); the Universal Child Aid ‘AUH’, Food card (‘Alimentar’); ‘Food Bank (‘Banco Alimentario’); or ‘Food Bags (‘Bolsones Alimentarios’) that subsidise food and products for the most vulnerable families.
The ‘Alimentar’ card is an instrument that the national state gives to mothers or fathers with children up to 14 years of age or to pregnant from 3 months of gestation. Basically is ‘money’ in a card that people can use to purchase food in stores that has card readers devices. Although it exists a national law no. 27.253 that obliges all businesses stores and shops to have card readers, the precariousness and informality of stores in vulnerable neighbourhoods, leads to lack of these devices, forcing beneficiaries to move outside the neighbourhood to be able to do use of them.
The ‘Food Bag’ is a food aid that has been delivered in La Plata every fortnight to 64 000 beneficiary families during the quarantine from 11 points of the city, none of them near Puente de Fierro, that is why the beneficiaries living in this neighbourhood lacked from accessing this service.
82 days of quarantine have passed. You are telling me that in 82 days the government did not think of a solution. They said to us ‘Stay at home’, but if I don't have to eat, how am I going to stay at home? 58 years old neighbour, comment said during n°44th Permanent Working Table Meeting
The ‘Food Bank’ is an aid that supports 161 social organisations with ‘community kitchens’ that daily provides meal service to members of vulnerable sectors of society. More than 20 400 people from the region attended to these organisations during pandemic situation. Referents from each ‘community kitchen’ must go monthly to one of the ‘distribution centres of Food Bank’ in order to be provided by food. Unfortunately, the closest distribution centre is located several kilometres from Puente de Fierro neighbourhood, an aspect that, without the possibility of having transport for food transfer (because of interruption of public buses due to the quarantine); this access was impossible.
Facing these situations, our work team proposed an intervention that consisted in a management model that was implemented within this project.
This model included a new paradigm was to move essential good towards the people, instead of making the people move to obtain those benefits.
Hence, new procedures were implemented by researchers of the project, in order to assure transport of ‘Food Bag’ and ‘Food Bank’ to the neighbourhood (Plaza in Streets 29 y 89). That is why, one member of the community was helped to regularly obtained food from classical ‘distribution centre’ and then these goods were delivered among community members by a new distribution centre inside the neighbourhood or in situ to each one of community kitchens in Puente de Fierro. The rule was ‘food moved, while people rested at home’. In this way, it was avoided unnecessary transfer of people during COVID-19 quarantine’.
Also, an administrative support that was provided to informal stores in order to have virtual payment devices for food cards reading and also for other types of debit/credit cards. So far, half of the informal food stores have already this benefit.
A survey performed after quarantine demonstrated that 91.7% of the inhabitant enrolled in the project admitted that had accessed in a regular and promptly way to ‘food state benefits’, while ‘Altos de San Lorenzo’ accessed in 54.7% in the same period to those goods.
CESS: identification and monitoring of COVID-19 cases
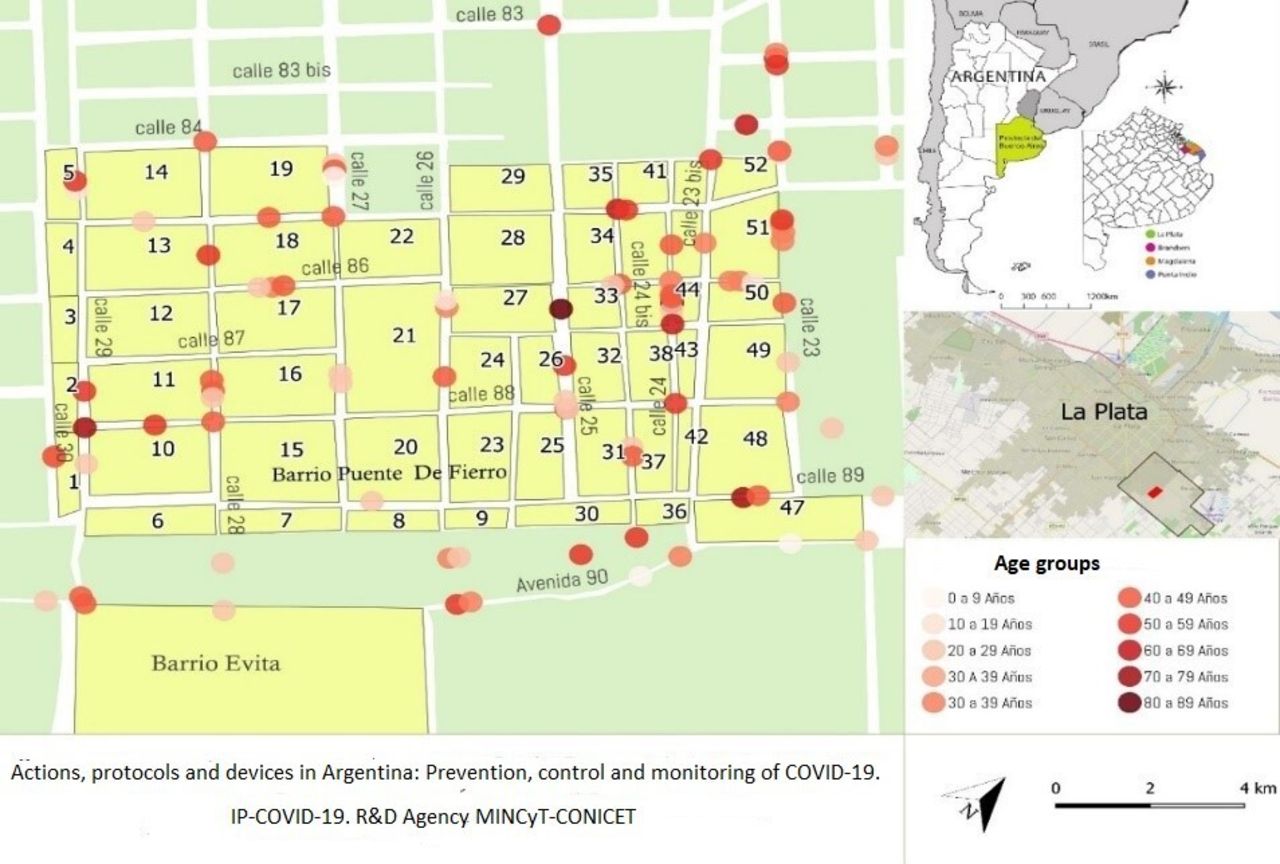
In those patients in whom contagion by COVID-19 was confirmed, mild or moderate cases were identified. Members of research team collaborated to detected isolation conditions. If the living place was appropriated, the patient remained at home, and our team provided food support, helped with administrative procedures and delivered medicines during the quarantine. If housing was inappropriate, our team helped to transfer patients to the government’s isolation centres (GIC). On the other hand, in severe cases, the transfer of patients to the nearest health establishments was performed by the ministry of health. When the members of the community were transferred either to GIC or to a hospital, our team provided daily reports of each patient to their family and friends in order to avoid public circulation during the quarantine period (figure 4).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Confirmed COVID-19 cases (grouped by age groups).
During the study period, 142 confirmed cases of COVID-19 were identified and georeferenced among community enrolled in the project. Four deaths were observed among the population of Puente de Fierro. When epidemiological data extracted from ‘Puente de Fierro’, neighbourhood was compared with the other neighbourhoods of La Plata, it is demonstrated that COVID-19 positive rate was 2.3/100 000 vs 3.6/100 000 inhabitants comparing Puente de Fierro with other suburbs with the same socioeconomically conditions and the ‘fatality rate’ was 2.8% vs 3.6%, respectively.
Actions to favour the access of the population to benefits of the local, provincial and national public administration during the pandemic period (documentation, collection of social assistance, supplies, cleaning of spaces)
In the initial survey, it was detected that among the members of Puente de Fierro Community, 32 individuals born in Argentina and 18 migrants lack of personal ID. Our group installed temporal mobile offices of the Ministry of Justice and ANSES (Pension Fund) in the neighbourhood (every Fridays during the study period) in the common space ‘Plaza’ of streets 29 and 89). ID was provided to all 40 people without personal identification. Also in 45 cases, old retired people without benefits were provided with retirements or pensions arrangements; in 16 cases, legal advice was performed, 13 consultations related to family issues were performed and in 3 cases of situations of gender violence was taken cared.
Regarding the supplies for the prevention of COVID 19, in a first exploration, the community had a total lack of either hygiene general elements and of specific materials COVID19 prevention. Hence, various actions were carried out inside and outside the network community to mitigate these shortcomings. Efficient intermediation was achieved to obtain chinstraps/masks, alcohol, bleach and protective masks from government’s institutions, and subsequently distributed these materials among the population.
Finally, lighting street devices, fumigation and cleaning task of common spaces were managed.
In 122 cases where severe chronic disease treatments were interrupted, medication was provided at patient’s home in order to assure adherence to those chronic disease therapies.
Degree to which the population complied with isolation measures during quarantine
The street mobility was reduced in 82.9% of basal activity. This point was demonstrated by mobile phone app uploaded by certain inhabitants designated as ‘study cases’.
The survey performed after quarantine also demonstrated hat 84.3% of the population of Puente de Fierro, while only 39.2% admitted that they respected government’s recommendations of staying at home during that period. The main reasons given for non-compliance with the guidance were: need to move to collect subsidies and state aid, going to the bank, food purchases, healthcare.
Discussion
The COVID-19 pandemic affected humanity in multiple ways, and its consequences will surely be remembered for a long time.19
On the other hand, preventive measures regarding limiting commercial and labour activity of the population in order to reduce the movement of people and interpersonal contact have caused serious socioeconomic consequences among the inhabitants of the countries affected by pandemic situation.20
These consequences have been mitigated with social aid measures from the state public decisions performed by the different governments. Argentina has been one of the countries with quick reflexes to propose tools that would allow families to tolerate the prolonged isolation imposed by the national authorities. State aids represented by various programmes were created or increased because of pandemic.21 However, the mere existence and availability of these potential benefits should not be considered as synonymous of direct access of the population to those assets, since this process must be finished when it is ensured that these goods reached all beneficiaries.
Although public policies can be easily executable in most sectors of the population; it exists areas, usually settlements and marginalised neighbourhoods of cities, that have certain characteristics like poor urban design, inhabitants with particular culture and interpersonal relationships; that can complicate the correct distribution of goods and services. Therefore, these situations must be taken into account in order to achieve the desired institutional objectives. Puente the Fierro is one of these thousand neighbourhoods on Argentina that has particular attributes that complicates the arrival of public programmes.
The experience of Puente de Fierro demonstrated how in special and complex situations such as the COVID-19 pandemic or its prevention measures; the offer provided by the public government becomes useless and dependent on the ability and willingness of own community members to reach the target population. The food cards, the administrative management of requesting or renewing identity documents, the complaint of violence suffered against the person, the initiation of job retirement procedures, the access to shops that accepts subsidy cards are all situations that require the transfer of people living in suburbs to urban areas where the devices to achieve access are located; and in times of pandemic, where free circulation the individuals with non-essential jobs is restricted, such access is impossible.
This study aimed to demonstrate how an intervention model created by a university volunteers together with the own members community beneficiary of the project, was able accomplished with quarantine and preventive isolation measures ordered by the country’s authorities; through the development of actions addressed to improved access to the goods provided by the State (economic aid, food, medical care) without living the neighbourhood and homes.
With these measures, inhabitants from Puente de Fierro were able to duplicate the unnecessary movements and to comply with government regulations. The positive externality of these actions was the reduction of COVID-19 infections by 36.2% and deaths by 22.3% among this population when compared with the control group (population from the neighbouring town).
In this sense, it is demonstrated by the results obtained that ‘healthcare’ is a good barometer to measure the way of whom public policies are accomplishing with its commitments. ‘Health is a historical–social process that includes diseases and illnesses, their social ways of caring for them, as well as the complex network of care that a society possesses. Health is relational care processes and their ways of managing them’.22 It is also known ‘as the ability to face and overcome the conflicts and adversities that the environment presents us’.23 Unfortunately, people often internalised their unfavourable situations that they have had in life since their birth, associating them with ‘normality’, aspect that avoid to develop capacities of perceiving risks and to promptly identify conflict situations that must be faced and solved. COVID-19 pandemic has exposed the unfair situation that socially vulnerable people had to face. Because of the quarantine, the normal activity of the society was interrupted, hence, government’s policies were aimed at reducing the negative impact by increasing budget items towards economic and social aid for those who have the least in society. However, the benefits provided by official programmes do not contemplate the particular locations in which the beneficiaries live. It is useless to have a stagnant supply of goods and services, when they are not appropriate distributed among those who need them. As seen in this study, suburban neighbourhoods such as Puente de Fierro have particular characteristics that must be taken into account when executing public policies. In the case of COVID-19, the main government slogans to avoid contagion was to limit the movement and transfer of people on the streets. These measures were well accepted in homes that have basic services, internet and the possibility of requesting food and other goods by delivery at home. However, in precarious housing, where the walls are made of cardboard and there is no floor, with lack of basic services, and in whom aid programmes are not reaching, it is difficult to comply with isolation measures, thus putting contagion control at risk.
The presented project applied a new management model to perform public programmes in socially vulnerable neighbourhoods in order to mitigate COVID-19 pandemic consequences. In addition, this model also helped for strengthening and consolidating community neighbourhood networks that function as liaison structures with the state system and with other public institutions and organisations outside the neighbourhood.
This fact provides sustainability and continuity to the project, since ties have been strengthened between the Puente de Fierro Community and the formal Local and National State Institutions that will last beyond the university’s conclusion of its participation.
It has been demonstrated how contagion could be reduced comparatively with other suburban neighbourhood, with the sole fact of guaranteeing that the population can access essential goods without having to move outside the neighbourhood. Also, how an early warning system for symptoms of contagion allowed proper handling of suspected cases and confirmed cases, by bring the system to people, instead of people having to move to meet the health system.
The results of the implementation of this model of management of pandemic in the neighbourhood allow us to validate it, as a pattern of control, monitoring and prevention of the harmful effects of COVID-19. This model might also be replicable in other health problems, and in other popular neighbourhoods in Argentina and other countries of Latin America with similar conditions, particularly in those urban agglomerations, which register occupation and territorial appropriation, with socially vulnerable circumstances such as the one observed in this work.
Data availability statement
Data are available in a public, open access repository.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
Footnotes
Contributors GHM and HB: study design. LM and GMat: data analysis. The rest of the authors contributed to developed community intervention actions. GHM is the author responsible for the overall content as the guarantor. The guarantor accepts full responsibility for the work.
Funding This project was carried out with the support of the National Agency for Scientific and Technological Promotion of Argentina. R&D Project IPs 415-440-650-763.
Map disclaimer The depiction of boundaries on this map does not imply the expression of any opinion whatsoever on the part of BMJ (or any member of its group) concerning the legal status of any country, territory, jurisdiction or area or of its authorities. This map is provided without any warranty of any kind, either express or implied.
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methodology section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.