Article Text

Abstract
Objective To identify and summarise the digital health interventions (DHIs) implemented for non-communicable disease (NCD) management for COVID-19.
Design Rapid scoping review. Three reviewers jointly screened titles–abstracts and full texts. One reviewer screened all excluded records. Data were mapped to WHO DHI Classification and narratively summarised.
Data sources PubMed, CENTRAL, CINAHL, EMBASE.
Eligibility criteria for selecting studies Peer-reviewed primary research published between 1 November 2019 and 19 September 2021 on DHI for NCD management during the COVID-19 pandemic. Reviews, editorials, letters, commentaries, opinions, conference abstracts and grey literature were excluded.
Results Eighty-three studies drawn from 5275 records were included. A majority of the studies were quantitative in design. Forty per cent of the DHIs were implemented in the Americas. Nearly half of these DHIs targeted mental health conditions. A majority of the interventions were delivered remotely and via telephones. Zoom (26.5%), email (17%) and WhatsApp (7.5%) were the top three platforms for care delivery. Telemedicine, targeted client interventions, personal health tracking and on-demand information services for clients were the most frequently implemented interventions. Details regarding associated costs, sustainability, scalability and data governance of the DHI implementations were not described in the majority of the studies.
Conclusion While DHIs supported NCD management during the COVID-19 pandemic, their implementation has not been equitable across geographies or NCDs. While offering promise towards supporting the continuum of care during care delivery disruptions, DHIs need to be embedded into healthcare delivery settings towards strengthening health systems rather than standalone parallel efforts to overcome system level challenges.
- COVID-19
- global health
- disease management
- delivery of health care
- health services research
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Summary box
What is already known?
The COVID-19 pandemic disrupted healthcare services, those with non-communicable diseases (NCDs) were disproportionately affected due to restrictive measures imposed to prevent SARS-CoV-2 transmission.
Recent research has highlighted the role of digital health interventions (DHIs) for public health responses against COVID-19 and clinical care for COVID-19 and remote management in the context of pandemic.
Reviews found that telemedicine was the most frequently employed intervention during COVID-19.
What are the new findings?
Nearly half of the DHIs were implemented for the management of mental health/neurological disorders.
Commonly available telecommunications tools (eg, telephones, internet-based short messaging tools and video calling platforms) were the most frequently used digital health innovations for NCD management during the COVID-19 pandemic.
This review mapped the DHIs for NCD management and their need (ie, health system challenges during the COVID-19 pandemic) using WHO DHI v1.0 classification.
Targeted client communication and personal health tracking were most popular for NCD management towards addressing gaps in utilisation, access and availability posed by the disruptions to routine health services delivery.
Summary box
How this study might affect research, practice or policy?
Need for focus on equitable distribution of DHIs for NCD management.
Need for implementation research to explore sustainability of DHIs for NCD management.
Need for transparent research reporting of financial, data governance and ethical aspects of DHI.
Introduction
COVID-19 has significantly impacted health systems globally. Containing the rapid spread of the SARS-CoV-2 has placed unprecedented demands on the health systems.1 This sudden surge in demand coupled with pre-existing resource constraints and fragile healthcare delivery systems has disrupted routine healthcare services at all levels of the healthcare system.1 2 Nearly every country experienced disruption in general healthcare services, with services in low/middle-income countries (LMICs) being affected the most.3 In particular, this abrupt disruption of health services has significantly affected individuals living with non-communicable diseases (NCDs).4 5 Health systems either ceased or scaled down services due to reasons such as: fear of contracting SARS-CoV-2 infections, repurposing of the health workforce for public health response and COVID-19 care, the conversion of NCD centres to isolation zones, closure(s) of health facilities for non-emergency conditions and enforcement of physical distancing norms such as lockdowns and travel restrictions.6 7
The WHO’s rapid assessment survey in May 2020 found disruptions in 50% of NCD rehabilitative services in 163 countries during the pandemic.1 Services for management of hypertension (53%), diabetes and its complications (49%), asthma (48%), cancer (42%) and cardiovascular diseases (CVDs) (31%) were affected. Additionally, people living with NCDs are at risk of worsening of their NCDs.8 9 This was attributable to disruptions in essential NCD support and treatment services, a lack of access to appropriate management for conditions during the pandemic and a drastic decline in the utilisation of, for instance, chemotherapy services and urgent referrals.1 10–12 Furthermore, these disruptions are likely to adversely impact the achievement of multiple NCD-related targets of the 2030 Sustainable Development Goals.9 13–15 Thus, it is crucial to ensure the continuity of care for people living with NCDs amidst this pandemic, keeping in mind the interlinkages between NCDs and COVID-19.
This unprecedented situation has demanded novel solutions, adaptations or innovations in care delivery mechanisms to minimise in-person contact at the health facilities and promote remote care.9 16 Reviews and WHO documents consistently highlight the need for innovations to respond to the (increasing) NCD burden during, and following, the COVID-19 era.1 17 This pandemic has spotlight digital technologies as a vital tool to innovatively support the response efforts to COVID-19.18 19 Additionally, our previous work has highlighted the importance of, and opportunities for, digital technological solutions to ensure a continuum of care for people with NCDs.20 21 Many reviews on digital health interventions (DHI) for NCD management have focused on a subset of NCDs (eg, the use of telemedicine for mental health or neurological disorders22 23), a specific time period within the pandemic (eg, technologies implemented in the first COVID-19 wave17) or a subset of DHIs (eg, use of smartphones to ensure continuity of care during this pandemic24). There is a need to build on these efforts and broaden the horizon of our understanding of technological innovations for NCD management during health emergencies such as COVID-19 pandemic.
In such a situation, we assessed that a scoping review was an appropriate and important first step to (1) comprehensively review, and map from, the breadth of available literature the DHI implemented during this pandemic for the management of various NCDs, (2) map the range and functionalities of the DHI and (3) to identify the gaps to inform future research efforts.25–28 The rapid nature of the review will provide a timely and relevant response to the call for the ‘Innovations in Non-communicable diseases’ supplement by BMJ Innovations. This call highlighted the need and importance of understanding innovations for this pandemic.29 We thus designed a rapid scoping review with an objective to identify, map and summarise, in a timely manner, the global DHI for people with NCDs during the COVID-19 pandemic.
Methodology
Design
A rapid scoping review was considered the most appropriate review design given the scope of the research question (ie, to identify and list all the DHIs for NCD management for COVID-19 pandemic), its relevance to the contemporary context globally and importance of summarising evidence within the limited timeframe.30–33 The timeframe of the review was 2 months; this timeframe included review conceptualisation and design, execution and manuscript writing. The review was conducted in accordance with a protocol. A rapid review approach streamlines the steps of a traditional systematic review to produce timely and contextual evidence.33 Rapid reviews have gained popularity and recognition to inform policy, and aid in health system strengthening within quick timeframes.30 34
Eligibility criteria
Primary peer-reviewed research on digital health innovations for the management of NCD designed or adapted for the COVID-19 pandemic were eligible. All studies except reviews, editorials, letters, commentaries, perspectives, opinions, reports, conference abstracts and grey literature were eligible for inclusion. Only published English-language studies conducted on humans were included.
Population
Persons diagnosed with or living with an NCD, irrespective of the diagnostic criteria used.
Intervention
Any DHI related to NCD management. Keeping in mind the broad and dynamic nature of DHIs, we adopted the DHI definition used in the WHO Classification of DHI v1.0 as a ‘discrete functionality of digital technology that is applied to achieve health objectives’.35 36 The WHO Classification of DHI v1.0 was subsequently used to map the functionalities of the DHIs included in our review.36
Comparator
Any comparator including the standard-of-care, an alternate intervention or ‘do nothing’ scenario for NCD management. Studies without comparators were also eligible for inclusion.
Outcome
Our objective was to list the innovations meant for the management of NCD during the COVID-19 pandemic. Thus, we did not limit studies by type of outcomes or outcome measures. We operationally defined innovations as an umbrella term to include any novel intervention or solution implemented to overcome health service challenges during the COVID-19 era.
Settings
All settings including clinic/hospital, community or population, schools and so on were eligible for inclusion in the review.
Study context
DHIs should have been published between 1 November 2019 to the date of conducting searches, that is, 19 September 2021. Additionally, the DHIs should have been either designed for, or deployed during, the COVID-19 pandemic.
Management of NCD(s)
Studies should have included one or more of the following components to be eligible: ‘treatment, referral, monitoring, support, follow-up, palliative care’.23
Exclusion
Grey literature, and studies related to vaccines, biologicals, pharmacological products, biomarkers, diagnostic studies, therapeutic trials, predictions, simulations, infection control, management of COVID-19, protocols, preprints and burden of disease.
Searches
A broad search strategy was first developed for use on PubMed (PK and SM independently, modified after pilot-testing with the team) and subsequently adapted to the other databases (SM). Electronic searches were conducted on 19 September 2021 on PubMed, EMBASE (Ovid), CINAHL (EBSCo Host), Cochrane Central Register of Controlled Trials (CENTRAL). The final search strategy was a combination of free text, Medical Subject Headings and database specific subject headings for three domains of search—NCDs, management, innovations or interventions. The full electronic search strategies for all databases can be accessed on Open Science Framework.37 Searches were managed on EndNote V.X9.38
Study selection
Records were distributed among PK and NG for study selection. Screening was performed on Rayyan.28 Screening decisions were ‘include’, ‘exclude’ or ‘maybe’ (when in doubt). Study selection was performed on Rayyan in two sequential stages: title–abstract (Ti-Ab) followed by a full-text review. Excluded Ti-Ab and full texts were screened by SM. Ti-Ab that were marked as ‘maybe’ or where there were conflicting decisions between PK/NG and SM were taken forward to full-text review. Disagreements in the full-text review were resolved through discussions with MG and OJ. The rapid review timeframe precluded the process of contacting authors of studies for additional information. Thus, studies requiring additional information for the decision of inclusion were excluded. To ensure quality within the rapid review timeframe, independent screening for 30 records was performed by the screening team.
Data extraction
Data were extracted using a spreadsheet that was pilot-tested on five included full-text records by SM and PK on Google Sheets. Only the most essential study and innovation characteristics were extracted. Data items for charting included: study ID, study objective, study design (quantitative/qualitative/both), country of implementation, settings, NCD(s) targeted, type of innovation, brief details of intervention and comparator (summary/title of DHI, mode(s) of delivery, platforms and devices for delivery of DHI, security, financial aspects) and funding support (yes/no, partial/complete). The countries of implementation were categorised according to the WHO regions.39 Study designs were further categorised as observational or interventional.
DHIs were mapped to the WHO’s Classification of Digital Health Intervention v 1.0. categories 1.0 (Client), 2.0 (Healthcare providers), 4.0 (Data Services) by MG.36 The need of DHI was mapped to the Health Systems Challenges by MG, as recommended in the WHO DHI Classification document.36 Data items were labelled as ‘unclear’ when there was inadequate information for that field. Due to the rapid nature of the review, no author contact was performed to acquire additional information.
Data synthesis and reporting
Results are summarised narratively using frequencies and percentages (MS Excel, Google Sheets), and supplemented with tables and figures (map, graphs). Tableau Desktop Public Edition V.2021.3.1 was used for summarising and mapping countries of DHI implementation.40 An overall summary of the characteristics of studies is followed by description of DHI according to the targeted NCD(s) domains. We included neurological, neurodevelopmental and mental health conditions under the broad category of mental health. Results of WHO DHI classification mapping, and according to WHO region of implementation have been summarised under respective NCD domains. The reporting of this review has been informed by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews guidelines.41
Results
Study selection results
We identified 5275 records through the search strategy. After removing 765 duplicates, 4510 titles and abstracts were screened. Of these, 679 records proceeded to full-text screening, of which 50 full texts were inaccessible. Of the 629 full-text records that were assessed for eligibility, 83 were included in the review as per the inclusion criteria (see online supplemental file for the list of included studies). The reasons for exclusion included: wrong article type/study design (63.3%), wrong population (9.4%), pre-COVID-19 implementation (7.03%), wrong interventions (6.03%) and wrong outcome/inadequate information on outcomes, for example, user experiences without providing details of innovation (5.7%). The results of study selection are outlined in figure 1.
Supplemental material
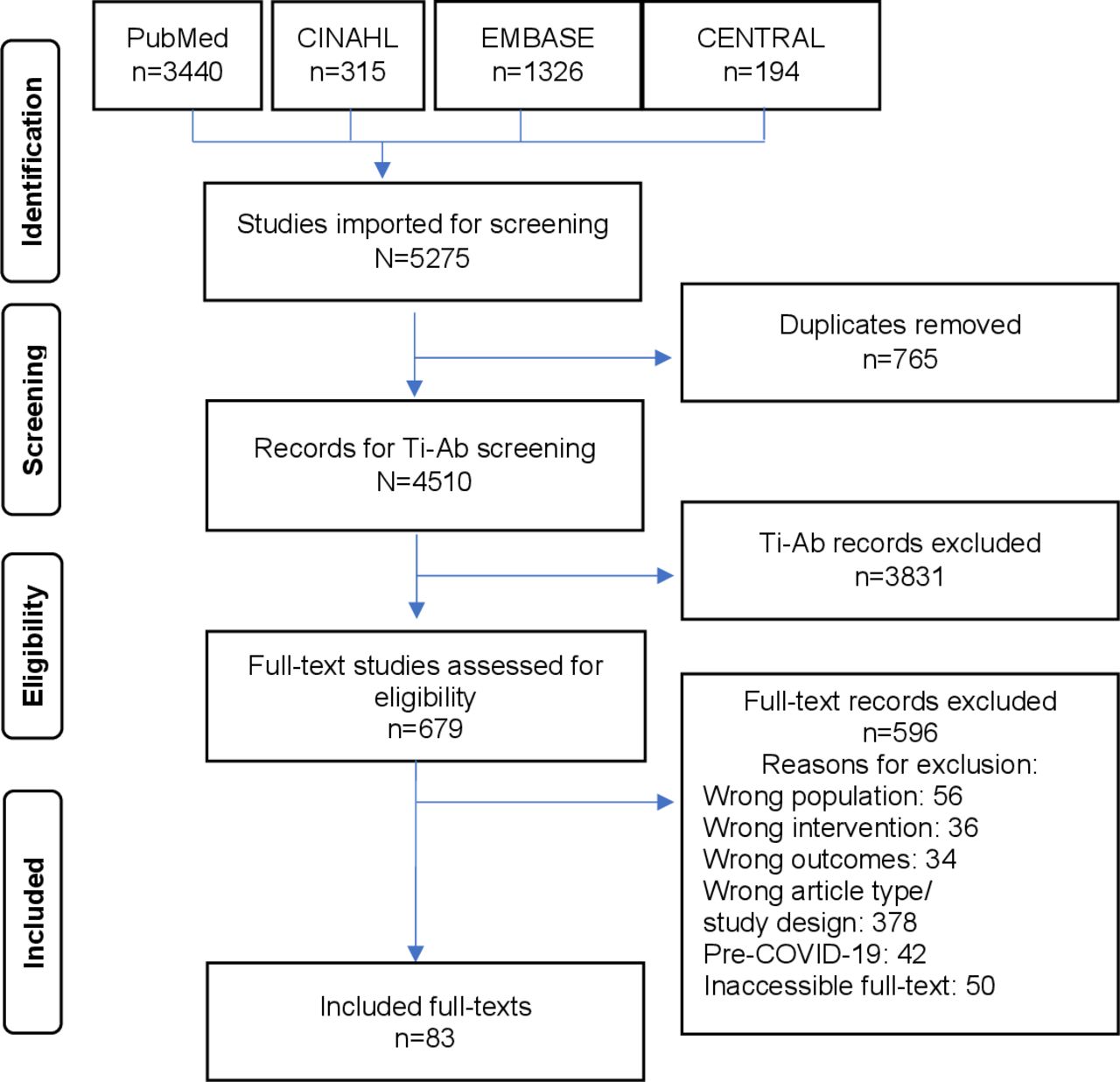
PRISMA flow diagram depicting the selection of studies in our review. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Characteristics of digital health innovations for NCD management during COVID-19
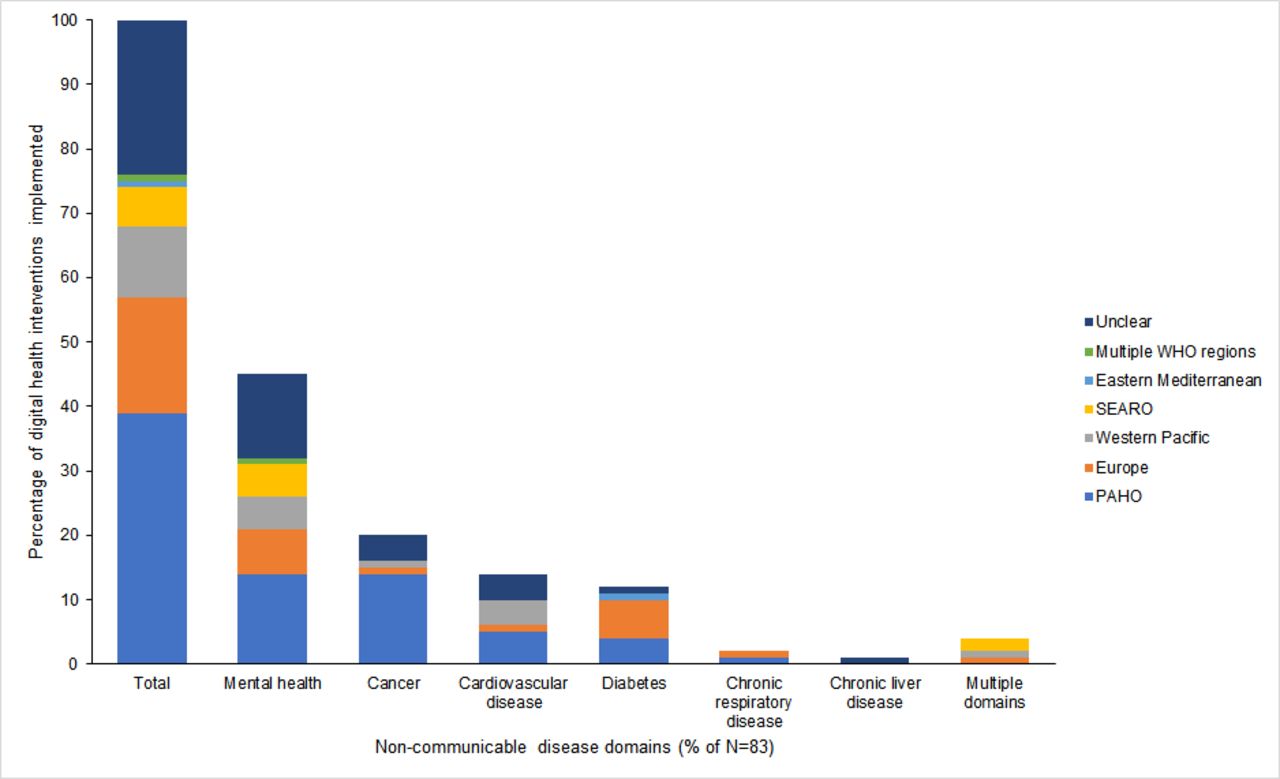
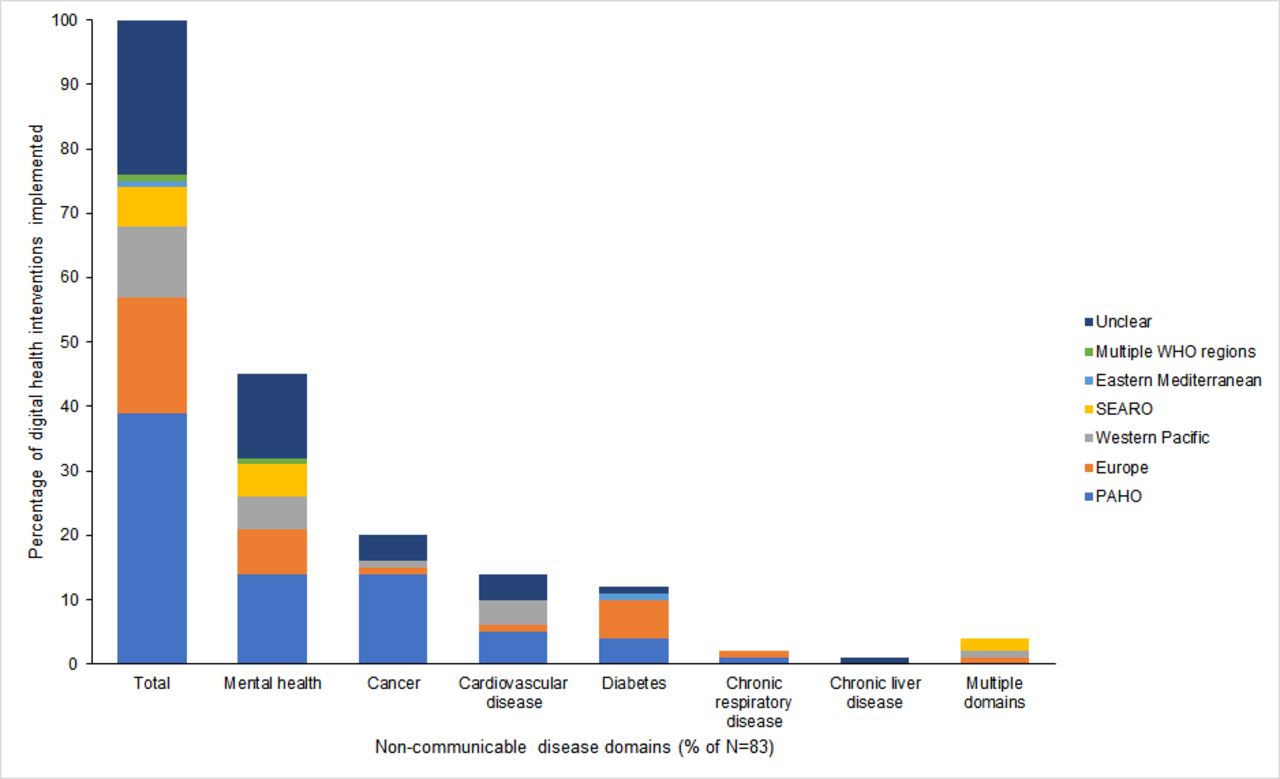
Of the 83 included studies, 76% (n=63) were published during 2021. Fourteen studies were designed as interventional studies. The region of the Americas accounted for 40% (n=33) of the DHIs implemented (figure 2). Only one DHI was found to have been implemented across all WHO regions. The region of implementation was unclear in 20 studies (24%). The country of DHI implementation has been summarised in a Tableau Dashboard.32 Most of the studies (n=71, 85.5%) were quantitative in design (table 1). Nearly one-third of the studies used a comparator to assess the impact or client experience of the DHI (table 2).
Characteristics of studies included in the rapid scoping review (n=83)
List of digital health innovations implemented in various countries
{kind=link}
{kind=link}
Digital health innovations implementation for the management of non-communicable diseases (NCDs) in various WHO regions.
Telemedicine was the most frequently used DHI for NCD management during this pandemic (n=77, 93%), followed by targeted client communication (n=49, 59%) and personal health tracking (n=24, table 3). All the 83 DHIs addressed one or more challenges faced by health services delivery systems during the COVID-19 pandemic. Innovations in DHI occurred as a result of the following: DHIs designed and implemented for the COVID-19 pandemic; implementation of pre-COVID-19 DHIs that were underused or optional for NCD management; modifications in, or adaptations of, pre-COVID-19 non-DHIs; and scaling-up of existing DHIs during the COVID-19 pandemic. Some solutions were rapid and pragmatic adaptations that were never implemented prior to the onset of this pandemic. These DHIs thus responded to the urgent demand posed by the government-imposed mobility restrictions to contain the spread of SARS-CoV-2. Most DHIs were innovations aimed at improving utilisation or access (n=61, 73%), and/or availability of health services for NCDs (n=51, 63%). A relative majority of the DHI (65.1%) were funded (partially or entirely) (see online supplemental file).
Platforms used by DHI implemented (n=83)
Delivery modalities of DHIs
A relative majority of the DHIs for NCDs were delivered remotely (n=52, 63%). A minor proportion of DHIs was delivered in-person (n=3, 4%). More than one-third used a combination of both the online and in-person modes either for all of the participants or for a segment of the participants (n=28, 34%). Among the remotely delivered interventions, 13% offered an optional in-person face-to-face service delivery component. The predominant rationale for including face-to-face delivery included: study protocol-related procedures (eg, overseeing the installing of the app), physical assessments (eg, walking tests), specific components of the intervention (eg, outdoor group exercises), drug dispensing, clinical exceptions, patient preferences, technological barriers, or as deemed necessary by the providers. Results of the delivery modalities of DHIs are summarised in online supplemental file.
Studies typically described a combination of various software platforms and devices (table 3 and online supplemental file). The three most frequently used software platforms for health services delivery geared towards NCDs were conventional communication tools such as Zoom (n=22, 26.5%), email (n=14, 17%) and WhatsApp (n=6, 7.2%). Twelve DHIs (14.5%) integrated online platforms with their electronic health/medical records or hospital information system . Telephones (including smartphones) were the most frequently used device (n=65, 78.3%) to deliver the DHI. Customised/NCD-management specific apps/platforms were the DHIs implemented across 34 studies (41%). Use of DHI components such as the platform, type of software, compatible devices were inadequately described in 10%, 9% and 7% of DHIs, respectively.
Financial sustainability and data governance
Specific information around the costs of the innovation and its implementation such as operational, maintenance and associated personnel costs were not described clearly across 64% (n=53) of the studies. A small proportion of these DHIs (10%) was offered as free to the patients, including those that were funded (eg, by the Ministries or implementing institutions). Information on data governance, in specific data security-related aspects of the DHI were not clearly described in more than half the studies (59%, n=49). The remaining studies described basic measure around health information and data security such as use of encryption, software solutions for security, compliance with guidelines (eg, Health Insurance Portability and Accountability Act, General Data Protection Regulation). However, specific details around data governance of these DHIs could not be ascertained across most of the studies, even for those that mentioned using a secure or privacy-compliant platform.
Digital health innovations for specific NCDs
Details of DHI implementation and classification according to the WHO DHI classification v1.0 are summarised in table 4 and the online supplemental file. In terms of the specific NCDs targeted, the following were the priority implementations.
Summary of mapping of studies to WHO DHI classification V 1.0
Mental health conditions
Forty-six per cent (n=38) of the DHI related to the management of mental health conditions, neurological or neurodevelopmental diseases. More than one-third of the studies aimed at mental health conditions were implemented in the Americas (n=12). The location of implementation was unclear in 30% (n=11) of the studies (table 1). These innovations covered a broad range of conditions such as neurological or neurodevelopmental disorders, depression, dementia, Parkinson’s disease/Parkinsonism, chronic post-traumatic stress disorder, eating disorders, chronic epilepsy (including childhood epilepsy). The specific mental health condition was unclear in as many as 40% of the studies. Telemedicine was the most frequently used intervention (n=35, 92%). Fifty-five per cent of these DHIs incorporated targeted client communication; 16% had client-to-client communication and personal health tracking provision; 26% had on-demand information services to clients and 3% reported on client financial transactions. Regarding data services, 13% provided services for data collection, management or use and 3% had data coding services.
Cancers
Of the 17 DHIs (20.5%) for cancer/oncology management, the majority was implemented in the Americas (71%), followed by the European and Western Pacific regions (n=1 each, 6%). A majority of the DHIs were implemented for breast and lung cancers. All DHIs that were implemented for cancers used telemedicine. Half of the DHIs incorporated targeted client communications; 18% used personal health tracking and 12% incorporated client financial transactions. Six per cent of the DHIs provided services for data collection, management or use. Nearly 25% of the DHIs incorporated prescription and medication management.
Cardiovascular diseases
Thirteen per cent (n=11) of studies related to DHIs for CVD management, of which the locations of three studies (27%) were unclear. More than one-third of the DHIs were implemented in the Americas (n=5). Among the DHIs for cardiovascular conditions (n=11); coronary heart disease and heart failure were commonly targeted conditions. A majority of the DHIs used targeted client communication (82%) and personal health tracking (64%). All of the CVD-related DHIs incorporated telemedicine. Thirty-six per cent of the DHIs incorporated prescription and medication management. Nine per cent of the DHIs provided services for data collection, management or use, and location mapping.
Diabetes
Of the 10 DHIs (12%) implemented for type 1 and/or type 2 diabetes, half of the DHIs were implemented in Europe and one-third (n=3) in the Americas region. A relative majority of the studies used targeted client communication (70%) and personal health tracking (60%). One-third and one-fifth of the DHIs also used untargeted client communication and client-to-client communication, respectively. Telemedicine was used in 80% of the DHIs. Data collection, management and use, and data coding were incorporated in 40% and 10% of DHIs, respectively.
Other NCDs
Two (2.4%) and one DHI (1.2%) were implemented for chronic respiratory and liver diseases, respectively. Four DHIs (5%) were implemented for more than one NCD domain, half (n=2) of which were implemented in the South East Asian Region (SEAR). All multiple NCD-related DHIs used targeted client communication, while 50% of DHIs for respiratory conditions used client-to-client communications. Telemedicine was used by all respiratory-related and liver-related DHIs compared with 75% of the implemented DHIs for multiple NCDs. Half of the DHIs for multiple NCDs used prescription and medication management. Data collection, management and use services were used by half of the DHIs for both respiratory and multiple NCDs.
Discussion
This rapid scoping review identifies and summarises the attributes of digital health innovations implemented for the management of NCDs during the COVID-19 pandemic. The most frequently targeted NCDs related to mental health, neurological or neurodevelopmental conditions. Telemedicine was the most frequently implemented intervention. Telemedicine or telehealth has been widely used during this present COVID-19 pandemic for its long-lasting ‘remote’ care continuity solutions for NCDs such as cancer,42 mental health43 and spiritual support for critical or end-of-life situations.44 A scoping review on technologies for any health condition in the first COVID-19 wave similarly found telemedicine as the most frequently implemented technology (85%).17 The demand for innovations was amplified multifold during this pandemic, especially because of the mobility restrictions imposed by the governments to contain the spread of SARS-CoV-2. This in turn adversely affected the continuity of care for people living with NCDs.
Using the WHO DHI classification helped us identify the key elements that are likely to impact the large-scale DHI implementation including financial aspects, sustainability and broader data governance requirements for overcoming regulatory restrictions across geographies. The WHO DHI classification v 1.0 is vital to categorise technologies implemented to support needs of the health system and is especially useful for evidence synthesis approaches among others.36 Despite some challenges in broader application and/or adoption by particular stakeholders involved in clinical care,45 mapping the DHIs to their corresponding health system challenges promotes an understanding of the deployments and their needs.36 This endeavour can provide a shared language to inform planners, decision makers and researchers about the ‘functionalities of digital health implementations’ for NCD management,25 especially for rapid implementation in health emergencies such as the COVID-19 pandemic. We found that targeted client communications, personal health tracking and on-demand health information services for clients were the three most frequently used client interventions. This is expected since our review focused on management of special groups of people, in particular, those diagnosed with NCDs. The latter two interventions reflect the need for continuation of monitoring and supportive services—a critical component of continuum of NCD care during the COVID-19 pandemic. The pandemic has also resulted in significant lifestyle changes for people living with NCDs, especially among those with diabetes and with risk factors of cardiovascular diseases.12 Interventions for self-management will be important to mitigate the worsening of existing conditions due to, for instance, limited opportunities for outdoor physical activities due to the closure of parks and gymnasiums.12
We found that commonly used communication tools were the most frequently used interventions for health services delivery during the pandemic for the management of NCDs. As found in our review, repurposing of the available communication channels (eg, Zoom, WhatsApp, telephones) to ensure continuum of care during the COVID-19 pandemic.17 We additionally found emails to be a popular medium for health services delivery and continuum of care. Innovative practices need not be always inventive in nature; advances that are initiated and evaluated rigorously in other jurisdictions add to the evidence base of effective public health programmes in order to be scaled-up and implemented more widely. Rapid deployment of novel health innovations during public health crises has been described previously.46 47
Our review noted that telemedicine was the most commonly used digital health innovation for NCD management during the pandemic. This is no surprise as telemedicine offers multiple advantages, particularly relevant in this COVID-19 pandemic, that Dorsey et al refer to as its 5 Cs: ‘accessible care, increased convenience, enhanced comfort, greater confidentiality, reduced risk of contagion’.48 However, some of the challenges they and the telemedicine literature highlight hold relevance to our findings broadly. These have to do with technological barriers, digital literacy, financial and security aspects.17 42 48–52 We found an inequitable regional distribution in DHI implementation with most implementations in the Americas, especially the USA. This is similarly reported in other studies and possibly reflects the technological advancement of the countries and the regional SARS-CoV-2 burden.1 17 Furthermore, studies in our review either required segments of the population facing technological barriers to continue with in-person visits, or provided technological support (ie, donated or funded). Additionally, financial and security challenges exist particularly when DHIs collect, manage, store or transmit client health information; a majority of the DHIs in our review incorporated one or more of these functions. However, the majority of the DHIs in our review did not adequately address or report these design aspects.
The absence or presence of (access to) reliable technology, finances, digital literacy and motivation, thus determine inclusion and uptake for many DHIs.53 Needless to say, a complete shift to telemedicine without addressing the above challenges will only worsen existing inequities in access and disease outcomes.17 42 50 51 53 Digital technologies are increasingly being recognised as critical innovations to strengthen health services delivery systems.54–56 Thus, it becomes imperative to address the above aspects for scalability and continued uptake, considering the widespread use and integration of telemedicine in routine NCD care.49 COVID-19 restrictions made digital solutions necessary in many social sectors, and this society-wide transition is poised to significantly change the ways in which whole societies engage in, and enact health.57 Despite years of consistent efforts for the mainstreaming of DHIs, the health service delivery disruptions during this pandemic forced the health systems to pivot towards digital innovations for NCD-focused care delivery.58 This review highlights the considerable capacity for health systems to undertake this shift. However, sustaining these interventions beyond mere pilot projects has been a long-standing challenge for digital health implementors.59
Regular monitoring and evaluation of digital health innovations is the first step towards ensuring effective and safe DHI implementation, and several toolkits are available for this purpose.60 In the long term, embedding DHIs within healthcare delivery systems is a promising approach for their sustainabilty,61 and DHIs can effectively support integrated care models for NCDs.62 The WHO’s framework on Integrated People-Centred Health Services outlines an approach to institutionalising DHIs within digitally augmented, comprehensive care through supportive policies, sustainable financing, a suitably trained workforce and reliable infrastructure.63 It is also important that the DHI interoperates seamlessly with other DHIs within the broader digital health ecosystem, highlighting the importance of coding languages and interoperability standards.64
Finally, we bring attention to the use of the term ‘health innovations’, defined by the WHO as one that ‘aims to develop and deliver new or enhanced health policies, systems, products, technologies, services and delivery methods to improve people’s health’.65 Innovations are multifaceted in nature and are continuously being prototyped, piloted and deployed at scale or adapted to cater across services for a long time in tune with the healthcare sector challenges. A consensus across the literature is that to be an innovation would mean for it to be ‘patient-centric’ and to bring in ‘something new or significantly different from other solutions in the field’.65–72 Many studies in our review loosely referred to the need and/or use of innovations, and were limited by an inadequate description of ‘innovation’. On the other end, elaborate accounts brought clarity regarding the need, design (eg, using service design methods) and implementation of novel solutions. We thus support the call to researchers to explicitly define the need and design of their innovations in order to prevent a dilution of its meaning.70
This is the first rapid scoping review identifying global digital health literature for NCD management during the COVID-19 pandemic, and mapping it to WHO DHI Classification, to the best of our knowledge. While expediting the review, we incorporated measures for quality assurance for the review. Search strategies, screening protocol and data abstraction template were developed based on standard scoping and rapid review guidelines and literature review,17 30–33 73 74 pilot-testing, multiple discussions within a team experienced in content and methods. To minimise selection bias, we standardised procedures, trained and calibrated the team, and had one reviewer screen all excluded records. Mapping of studies to WHO DHI classification was performed by review members experienced in digital health and the WHO DHI classification tool (MG and NG).51 We used a comprehensive search strategy to minimise the risk of missing potential inclusions. However, we acknowledge that potentially relevant studies may have been missed because of the rapid nature of the review (eg, author contact for additional information, screen reference lists of included studies, seek grey literature/non-English language studies/ conference abstracts).
Conclusion
This review outlines the considerable progress made in digital health service delivery for NCDs during the COVID-19 pandemic, while noting the potential challenges to scale-up and wide spread adoption of DHI for NCD management. Health systems, despite their constraints, have made considerable efforts to continue service provision despite systemic disruptions. We have highlighted the important role of commonly available telecommunication tools for NCD management during the COVID-19 pandemic. Broadly, DHIs offer a promising and sustainable approach to NCD management. However, the distribution of DHI implementation for NCD management has not been equitable geographically or across NCDs, with certain regions (such as the Americas) and NCDs (eg, mental health conditions) documenting far more innovations than others. As the pandemic wears on, it is important that the diffusion of such innovations for NCD management reach those in LMICs where the need for them is greatest. This presents a noble and worthwhile agenda for more research and implementation of DHIs for NCDs as the health systems gear towards building back better beyond the COVID-19 pandemic.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Ethics approval
This study does not involve human participants.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @MurthyShruti, @MyronGodinho, @GudiNachiket, @Oommen_john
Contributors OJ conceptualised the study in consultation with BMJ Innovations team. NG and OJ developed the concept note. SM coordinated the review. All authors jointly developed the protocol. SM and PK developed and pilot-tested the search strategies, with significant contributions from MAG, NG and OJ. SM ran the searches, managed data and retrieved full texts. PK and NG screened titles-abstracts. PK, SM and NG screened full texts. SM also screened excluded titles-abstracts and full texts. MAG and OJ resolved disagreements. SM and MAG developed the data charting sheet. All authors revised it critically. SM, MAG and PK charted data, assisted by NG. SM analysed the data. SM, MAG, PK and NG jointly wrote the first draft. SM, MAG, AJ and OJ critically revised subsequent drafts for intellectual content. All authors read and approved the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Disclaimer Views expressed in this article solely belong to the authors and do not necessarily reflect those of the organisation/institutes that the authors belong to.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.