Article Text

Statistics from Altmetric.com
Summary box
What are the new findings?
The innovative use of community health teams equipped with ‘offline-first’ mobile health apps enabled the Padayon subscription service to deliver target outputs in terms of patients enrolled, BP and RBS tests provided, and prescribed medicines delivered.
The impact of Padayon on patient outcomes also supports the potential of this new digital health model, particularly the improvements in systolic and diastolic BP control for members compared with the baseline.
How might it impact on healthcare in the future?
Equipping networks of community health workers and members with ‘offline-first’ platforms and mobile health apps can overcome traditional access barriers for non-communicable diseases (NCDs) in low-income and middle-income countries.
Integrating coaching, screening and medicines into a simple subscription service delivered by ‘digitised’ community members has the potential to significantly improve health outcomes in low-connectivity, low-resource settings.
There is patient willingness to pay for digital subscription services for diabetes and hypertension even in populations on an average daily income of $3–7 per day.
Quality health data can be collected through community teams with ‘offline-first’ platforms, enabling remote patient monitoring and analysis for population-level precision healthcare.
Introduction
Non-communicable diseases (NCDs) account for 41 million global deaths every year, equating to 71% of global deaths overall. Of the 41 million deaths, 29 million occur in low-income and middle-income countries (LMICs).1 However, health system services for prevention, education, screening and treatment of NCDs remain inaccessible to billions of people living in rural regions in LMICs. The WHO has reported that over half the world’s population lack access to the basic health services they need.2
Digital health has the potential to address the gaps and weaknesses of traditional health systems.3 Unfortunately, many digital health services do not work in regions with low internet connectivity and low digital literacy.4 Approximately 3 billion people lack internet connectivity at all.5 The growth in virtual healthcare during the COVID-19 pandemic has been primarily in affluent, metropolitan areas.6 Digital health needs to better serve the low-income, rural populations at risk of NCDs.
A new digital health model, Padayon, for diabetes and hypertension was designed to address this challenge across LMICs. The focus was the municipality of Pototan, Western Visayas, in rural Philippines. The prevalence of type 2 diabetes among adults in the Philippines is estimated at 7%, comprising almost 4 million cases and accounting for 6.5% of mortality across total deaths in 2020. Cardiovascular disease is the single largest cause of mortality in the Philippines, accounting for 33% of total deaths.7 There are significant health system weaknesses in Pototan, where residents live on an average income of $3–7 per day and over an hour from healthcare providers. There is a lack of access to basic screening such as random blood sugar (RBS) testing, with a comprehensive panel for diabetes at a private clinic costing 10 times the residents’ daily wage. Residents must travel over an hour to pharmacies and buy medicines for at least $30 per month.8 There are also shortages of health workers in Pototan, with a doctor to population ratio of 1:78 298 compared with the WHO benchmark of 1:1000.9 10
The objective was to address these needs and improve the outcomes for the Pototan population by harnessing ‘offline-first’ health technology (applications that can be used without internet connection and synced when back online) and community involvement.
The specific aims were the following:
To evaluate the effectiveness and scalability of the ‘offline-first’ digital health intervention in managing diabetes and hypertension in low-resource settings.
To assess the impact of the intervention on patient outcomes for diabetes and hypertension.
% change in systolic/diastolic blood pressure (BP).
% change in RBS.
% change in knowledge of diet and nutrition.
% change in understanding of diabetes and hypertension complications.
% member retention rate.
Overall lives improved (definition: patients able to put their previously uncontrolled systolic/diastolic BP numbers and/or RBS numbers into target range in at least one point during the programme).
Methods
This new digital health model was designed, built and implemented through a public–private sector partnership involving social enterprises Medtronic LABS and reach52 with Pototan municipal health providers.
Medtronic LABS designs and implements tech-powered, community-based healthcare delivery models for NCDs. One of their models, Prerna, is a comprehensive healthcare delivery model for people living with or at risk of type 2 diabetes, hypertension and comorbid diseases. The model integrates social and clinical interventions in a group-based setting, close to home. Medtronic LABS hypothesised that the Prerna model might work in other contexts.
reach52 is building stronger health systems and expanding access to health services across LMICs. Its ‘offline-first’ HealthTech platform enables a full set of health services for low-connectivity markets run by community members and health workers. Analysis of data collected alongside qualitative research reinforced the high-risk factors for diabetes and hypertension in the Pototan population, as well as the poor access to education, testing and affordable medicines.
Medtronic LABS worked with reach52 to adapt the existing Prerna model to the Philippine context. ‘Padayon’ (meaning keep moving forward) is a fully integrated health solution for low-income patients providing coaching, testing and medicines in one accessible subscription service. The service overcomes access barriers through a combination of ‘offline-first’ technology and community involvement. Patients paid out of pocket to enrol as members in a 12-week intensive service for $20 (approximately one-third of the typical cost for medicines and screening) and continue on a monthly subscription for $8 per month.
Research design and recruitment
This community-based observational study was conducted in Pototan, Western Visayas. Patient consent to enrol in Padayon was provided.
The study population comprised patients with hypertension and diabetes. To be included in the programme, the following participant criteria for Padayon was defined to enrol target patients who would benefit from the subscription service:
Diagnosed with hypertension, with systolic BP of at least 130 mm Hg and/or diastolic BP of at least 80 mm Hg.
Diagnosed with diabetes, with RBS higher than 200 mg/dL and haemoglobin A1c (HbA1c) level at 6.5% or higher.
Require antihypertensive and/or oral antidiabetic medications, with diet and exercise no longer enough to control their conditions.
The flow of recruitment of participants can be seen in figure 1.

Recruitment flow.
For analysis, basic data on age, sex, height, weight, diet and physical activity were collected from the members through the reach52 access app. Patients had their diagnostic measurements for RBS and systolic/diastolic BP logged into the app on a biweekly basis through the 12-week intensive period and then on a monthly basis through the maintenance period. The evaluation of impact on knowledge of diet and nutrition and complications was monitored through a self-administered survey.
12-week intensive service
Enrolled members participated in a 12-week intensive service combining in person and virtual coaching, BP and RBS testing, and delivery of patients’ prescribed diabetes and hypertension medicines directly to their barangays (villages).
An overview of the intensive service can be seen in figure 2.

Intensive service overview. BP, blood pressure; RBS, random blood sugar.
In person and virtual coaching
Public health nurses were equipped as ‘health coaches’ to provide biweekly in person coaching sessions on diabetes and hypertension at rural health units.
Between the sessions, members were provided with mobile learning resources and set tasks, such as new dietary and exercise habits. A Facebook community group was established on a low-data version of Facebook to enable members to share learnings and provide peer support.
Screening and remote monitoring
Members received a biweekly test for BP and RBS in their barangays from the Padayon health coaches and barangay health workers. Health coaches and barangay health workers were equipped with a diagnostic toolkit and ‘offline-first’ mobile health (mHealth) apps to capture screening results and enable remote monitoring. The apps were designed with a simple user interface and to work on basic Android operating systems. With its ‘offline-first’ functionality, barangay health workers could conduct screenings and capture the readings offline and then sync data when back at an online location.
Affordable medicines
Community members were equipped as ‘agents’ with mHealth apps to manage the orders and delivery of affordable medicines. The agents visited members door-to-door to process biweekly medicine orders based on prescriptions scanned into the mobile. Once back online, the agents synced the data and orders were submitted digitally to partner pharmacies to process for delivery into the communities. The agents were compensated through commission for every medicine order successfully processed and delivered, supporting the United Nations Sustainable Development Goal 8 (decent work and economic growth) as well as United Nations Sustainable Development Goal 3 (good health and well-being for all).
Monthly maintenance service
At the end of the 12-week intensive service, the goal was to continue to support the members in keeping their diabetes and hypertension under control. Making new habits simple to continue is important in influencing behaviour change.11 The solution was to equip the barangay health workers as community agents with the ‘offline-first’ mobile platform to provide continued education, testing and affordable medicines to members at their homes on a monthly basis.
The agents coordinated with pharmacy partners to collect and distribute prescribed medicines during their monthly visits. During the visits, they also reinforced the coaching and entered the results of the BP and RBS tests into the app. These data could be shared with the Pototan municipal health officer, integrating community-based care with rural, public health systems.
Results
I’ve had Diabetes for 30 years now. It has been a challenging journey, especially the burden of medicine costs and there are a lot of foods that I must avoid. I’m really happy that Padayon arrived in our barangay and gave us easier access to blood pressure and sugar checks, affordable medicines, and Diabetes education. (Padayon member, 64 years old)
The innovative use of community health teams equipped with ‘offline-first’ mHealth apps enabled the Padayon service to effectively deliver target outputs in terms of patients enrolled, BP and RBS tests provided, and prescribed medicines delivered.
The impact of the intervention on patient outcomes also demonstrated the potential of this early-stage innovation, in particular the change in systolic and diastolic BP control for members compared with the baseline (tables 1 and 2).
End of 12-week intensive service
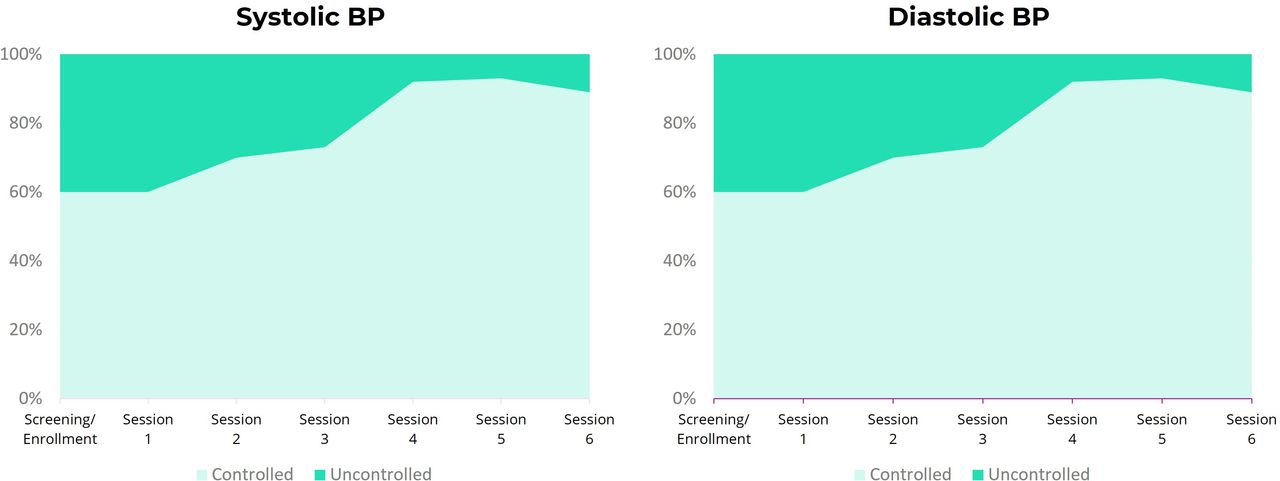
Impact of intensive service on systolic and diastolic blood pressure (BP) of enrolled patients.
End of 12-week monthly maintenance service

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Impact of intensive service on knowledge of diet, nutrition and diabetes complications of enrolled patients
While it was not a key performance indicator, it should be noted that use of virtual coaching resources provided to members’ mobile phones and the Facebook community group was lower than anticipated. The barrier was that less than 20% of the enrollees had mobile access to even the basic low-spec version of Facebook.
Discussion
‘Task-shifting’ involves the redistribution of tasks from highly qualified health workers to health workers with shorter training and fewer qualifications to make more efficient use of the available human resources for health.12 The need for task-shifting is emphasised by the predicted 18 million shortage of health workers worldwide in 2030.13
Padayon demonstrated the benefit of task-shifting to community health teams with ‘offline-first’ mHealth apps on diabetes and hypertension management in low-resource settings.
This type of model can also be more sustainable and scalable as it equips members of communities as health workers or agents to provide education, testing and medicines for their communities rather than through traditional healthcare professionals and facilities.
However, the challenge of low digital literacy should not be underestimated—2.9 billion people in the world still have not used the internet.14 As well as increased digital education for the communities, there is the opportunity for greater involvement of caregivers to help older household members access these services.
The enrollment and retention outputs illustrate that low-income patients are willing to pay for subscription services (comprising coaching, testing and medicines), providing the price is affordable. In this intervention, the subscription price was subsidised so there remains the need for more cost-effective solutions for medicines and tests needed in LMICs.
Limitations
There was no random control group incorporated in the study as given the very low diagnosis rates (diabetes at 3%, hypertension at 14%) in Pototan this currently would be of limited use. An additional benefit of Padayon was to establish the groundwork for future random control trial studies in diabetes and hypertension in the region.
Due to the expensive price of HbA1c tests for low-income populations, only RBS levels (and BP) were tracked for enrolled patients with diabetes. As there is an inherently large variance in RBS levels in any given day, there is a lack of clinical literature correlating its usage as a predictor of future complications compared with HbA1c.
The population in Pototan faces typical access to healthcare barriers for rural populations in LMICs,2 but it should be noted that reach52 has operated health services in the municipality since 2018. Padayon may have benefited from established trust in this population compared with implementing Padayon in completely new populations. However, compared with more rural, disconnected municipalities, the Pototan rural health unit still receives some supply of oral antidiabetic drugs from the Department of Health, although intermittently, which may have reduced enrollment in this population.
Conclusions
The results achieved by this Padayon early-stage innovation demonstrate the value of ‘task-shifting’13 to community health workers and informal healthcare providers equipped with ‘offline-first’ mHealth applications, and the potential for such scalable community-based model in overcoming the access barriers of traditional primary healthcare providers.
The community-based health teams were effective in engaging, screening and enrolling 80 low-income residents into the Padayon service and managing the monthly and biweekly testing and medicine delivery across the 6-month period.
The impact of the digital health intervention on outcomes also supports the potential of the model, particularly the improvements in systolic and diastolic BP control of the members compared with the baseline.
Padayon also illustrated its potential as a sustainable solution managed by local and community health teams, with continued subscription to the service during the maintenance phase.
With relatively low usage of digital resources by the patients, further work is needed to identify how to accelerate the digital literacy of communities in low-resource settings so they can benefit fully from health technologies in the future.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants. We have approval to implement and report on this pilot health service from the Pototan local government unit and municipal health officer. The early-stage innovation report is based on this pilot. Approval to implement this intervention (including ethical considerations) was provided by the local government unit in Pototan. This ethical approval was sought from the local authority due to lack of existing academic or health infrastructure in Pototan. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
With thanks to the Pototan local government unit and Pototan municipal health officer, Doctor Rodina Mondragon, for their collaboration on this new model in the Pototan municipality.
Footnotes
Twitter @Rich_Bryson
JP, AS and RB contributed equally.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests All authors are also employees of reach52 and Medtronic LABS.
Provenance and peer review Not commissioned; externally peer reviewed.