Article Text

Abstract
Objective Kangaroo Mother Care (KMC) is a frugal innovation improving newborn health at a reduced cost compared with incubator use. KMC is widely recommended; however, in the UK, poor evidence exists on KMC, and its implementation remains inconsistent.
Design This Systematic Review and Realist Synthesis explores the barriers and facilitators in the implementation of KMC in the UK.
Data source OVID databases, Cumulative Index to Nursing and Allied Health Literature (CINAHL), Scopus and Google Scholar were searched.
Eligibility criteria Studies were UK based, in maternity/neonatal units, for full-term/preterm children. First screening included studies on (1) KMC, Kangaroo Care (KC) or skin-to-skin contact (SSC) or (2) Baby Friendly Initiative, Small Wonders Change Program or family-centred care if in relation to KMC/KC/SSC. Full texts were reviewed for evidence regarding KMC/KC/SSC implementation.
Results The paucity of KMC research in the UK did not permit a realist review. However, expanded review of available published studies on KC and SSC, used as a proxy to understand KMC implementation, demonstrated that the main barriers are the lack of training, knowledge, confidence and clear guidelines.
Conclusion The lack of KMC implementation research in the UK stands in contrast to the already well-proven benefits of KMC for stable babies in low-income contexts and highlights the need for further research, especially in sick and small newborn population. Implementation of, and research into, KC/SSC is inconsistent and of low quality. Improvements are needed to enhance staff training and parental support, and to develop guidelines to properly implement KC/SSC. It should be used as an opportunity to emphasise the focus on KMC as a potential cost-effective alternative to reduce the need for incubator use in the UK.
- child health
- delivery of health care
- global health
- health services research
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Summary box
What is already known?
Kangaroo Mother Care (KMC) improves survival, health, somatic growth, neurodevelopment, psychoemotional well-being of stable newborns, even preterm infants, positively impacts family relationships and is cost-effective compared with incubator use. Although it is used routinely in low-income settings, no study has explored its use at scale in the UK.
What are the new findings?
This study finds that research into KMC in the UK is inconsistent and of poor quality and other less intensive techniques, such as Kangaroo Care and skin-on-skin contact are used interchangeably with KMC.
It also finds that challenges to KMC use in the UK include lack of routine training for healthcare professionals and families, national guidance and guidelines, coherent policies and a health technology assessment for its adoption at scale. Families may lack the time and space to practice KMC and neonatal care units are not fit for purpose regarding KMC implementation. Facilitators include hospital accreditation systems such as the Baby Friendly Initiative.
Given the recognised benefits of KMC in certain infant groups, there are opportunities to improve KMC uptake in the UK and reduce the reliance for incubators in stable babies, for example, through enhanced training programmes both for parents and staff, changes in the culture of care, developing coherent guidelines and changing neonatal intensive care unit design to support parents to have their own privacy when practising KMC.
Introduction
Preterm birth is one of the leading causes of mortality for children under 5 years old.1 2 In low-/middle-income countries (LMICs), incubators can be prohibitively expensive3 and place an economic burden on neonatal intensive care units (NICUs) and wider healthcare systems.4 5 Developed in 1978, in Colombia,6 Kangaroo Mother Care (KMC) has proven to be a safe and effective alternative to incubators by improving physiological responses, metabolic functions, neurological and psychomotor development, family bonding as well as reducing risk of infections.6–11 A randomised controlled trial (RCT) observed improvements in mortality in stable children receiving either KMC 24 hours a day compared with incubators care (3.1% for KMC, vs 5.5% for children in the control group).12 However, regarding small and unstable children, the benefits of KMC are still uncertain and are the focus of current research.13 An RCT observed a reduction in mortality and promoted KMC in this specific population14 while another one did not observe any reduction in mortality.15 KMC is defined as ‘(1) early, continuous, and prolonged skin-to-skin contact (SSC) between the mother/father and the baby; (2) exclusive breast feeding or breast milk feeding; (3) early discharge after hospital-initiated KMC with continuation at home; (4) and adequate support and follow– up for mothers at home’,16 which should involve continuously maintaining the kangaroo position and follow-up in a multidisciplinary KMC programme.10 17 Kangaroo Care (KC) is SSC between the newborn and the caregiver. SSC involves the placement of the naked child on the naked mother’s breast.18 While KC and SSC may be used interchangeably,19 they must not be confused with KMC.20 In comparison to incubator use, KMC can be classified as a frugal innovation by reducing costs, focusing on core functionalities, and optimising performance.6 12 16 20–22
Compared with incubator care, KMC has further benefits both on children’s health and parents’ well-being.6 12 16 23 However, other than in some other high-income countries (HICs) (Sweden, USA) implementation and adoption of KMC remain low in HICs, and in particular the UK (table 1).16 24–27
Barriers of Kangaroo Mother Care (KMC)15–18
There are definitional concerns with KMC research and the few studies that have reported on KMC in the UK on close inspection actually use KC or SSC.26 28 While the effects of KC and SSC seem positive,29 the uptake of KC and/or SSC is poor in the UK.30 Only 50% of parents have as much SSC as they want to and only 64.4% of children receive immediate SSC, a low rate compared with other European countries.31 32 Several UK initiatives have been implemented to increase the uptake of KC/SSC such as the Small Wonders Change Program (SWCP), the Baby Friendly Initiative (BFI) and family-centred care (FCC);33–40 however, the uptake of KC and/or SSC remains poor in the UK.30 A UK-based economic evaluation concluded that for every 800 children receiving KC, between £688 136 and £2 009 563 would be saved per annum.35 41 The second main component of KMC, breast feeding, reduces morbidity and the risk of necrotising enterocolitis and gastroenteritis which may lead to a cost savings of £119 084–500 696, and £34 809–67 060, respectively.35 While KMC is defined as a low-cost and cost-saving intervention,17 26 its implementation may involve, in the short run, direct and indirect costs, in terms of training and adequation of neonatal unit for the provision of this type of care. Hence, an economic evaluation of KMC in the UK is needed to observe how its benefits (eg, potential reduction in the risk of illnesses and length of stay) would reduce the economic burden of the National Health Service (NHS).
KMC is a complex intervention and its worldwide implementation is not consistent.27 Given the cost effectiveness of KMC and its benefits on stable newborns, it is striking that it has not further scaled in the UK. It seems essential to unpack the mechanisms under which KMC works in the UK and those leading to its failure. The aim of this study is to explore the available published literature to understand the barriers and facilitators in the implementation and adoption of KMC in the UK. To this end, we use a Realist Synthesis Review because this permits an examination of how an intervention works and leads to its outcome, depending on the context,42 43 asking ‘what works, for whom, under which circumstances, in what respects, and how?’.42 44 It provides an improved knowledge of the intervention and allows the researcher to make the most appropriate decisions to enable the intervention’s success.45
Methods
The methodology is presented in five steps: (1) define the review scope, (2) develop initial programme theories, (3) search for evidence, (4) select and appraise evidence and (5) extract and synthesise data.43
Define the review scope
The uptake of, and evidence for, KMC in the UK is poor26 and no study has been conducted only and specifically on KMC implementation and its potential barriers and facilitators in the UK so far. Therefore, this study aims to address this gap. As there is discrepancy in the definition of KMC,20 the literature on KC or SSC was also explored.
Develop initial programme theories
Based on detailed review of international literature, including high-income, middle-income and low-income countries, six programme theories were defined as enhancing KMC uptake and nine programme theories were defined as ‘rival’ programme theories, that is, limiting its uptake (table 2).
Programme theories based on international literature (high-income countries (HICs) and low-/middle-income countries (LMICs))
Search for evidence
Electronic databases (Embase, Global Health, Health Management Information Consortium (HMIC), Medline, Midwives Information and Resource Service (MIDIRS), APAPsycInfo, CINAHL, Scopus) and Google Scholar were searched in May 2021 (see online supplemental appendix 1 for respective search terms and strategies). The search terms were based on (1) the context/country, (2) the method under study, and (3) preterm infants and parents as well as their synonyms. The common inclusion criteria were that studies had to be UK based, in maternity and/or neonatal units, and for full-term and/or preterm children. First, titles were reviewed, and selected studies were related to either (1) KMC, KC, or SSC or (2) BFI, SWCP or FCC. Second, the abstracts were reviewed and retained if related to (1) KMC, KC or SSC or (2) BFI, SWCP or FCC if in relation to KMC, KC or SSC. Full texts of eligible studies were reviewed for evidence regarding the context, mechanisms and outcomes of the KMC/KC/SSC approaches. Further articles were identified from reference lists of included articles. As there is very little evidence on KMC in the UK, non-peer-reviewed research was also included (online supplemental appendix 2).
Supplemental material
Select and appraise evidence
Results were exported on the 14 May 2021 and duplicates were removed on EndNote. After the first screening, studies were organised regarding their main topic of investigation (KMC/KC/SSC/BFI/SWCP/FCC). Full-text screening was applied to the selected studies. The Critical Appraisal Skills Programme (CASP) checklist, recommended by Cochrane and the WHO for qualitative synthesis, was used to assess the quality of the studies.46
Extract and synthesise data
A data extraction form was created to extract pertinent information of the included studies such as the context, the mechanisms and the outcomes (online supplemental appendix 3). The aim was to clarify and assess the programme theories previously defined with the studies’ findings and to understand ‘what works, for whom and under which circumstances’.42
Results
Kangaroo Mother Care
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow chart presents the screening and selection process for KMC articles. After the first screening, 17 studies were retained in the KMC category, from which 13 studies were removed. The remaining four were selected for the analysis (figure 1.).

Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow chart—Kangaroo Mother Care (KMC). KC, Kangaroo Care; SSC, skin-to-skin contact.
The included studies involved one controlled trial,28 one review26 and two commentaries.47 48
All included studies aimed to analyse KMC26 28 47 48 but only Donald provided an accurate definition of KMC26 and also explored the benefits of SSC, using its evidence to provide information on KMC.26 Platonos et al did not include KMC in their methodology but, instead, SSC.48 The other commentary used references both on KMC and SSC to provide information on the KMC benefits.47 Finally, the controlled trial only includes SSC in the KMC definition.28 While all four studies aimed to explore KMC, (1) they provided either an incomplete or inappropriate definition (2) KMC’s findings were based on SSC/KC evidence and (3) KMC, KC and SSC were used interchangeably. A summary of the link between the context and mechanisms to explain the observed outcomes from the included studies is presented below with the full data extraction available in online supplemental appendix 3.
Context
Two studies provided information on context while the two others did not.28 47 Donald focused on a woman, separated from her child, without opportunity for early SSC.26 Platonos et al, explored the participation of the Imperial College Healthcare NHS Trust Neonatal Service in the global ‘Kangaroo Challenge’, inspired by the Sunnybrook Children’s Hospital in Toronto, Canada.48
Mechanisms
Two studies implemented specific tools such as written guidelines, training programme, informative tools for the parents and KMC-trained nurse to achieve their goals.28 48
Outcomes
Education and clear guidelines/policies are essential to enhance KMC practice and enabled an important increase in the number of hours performing SSC.26 48 In the UK, different guidelines promote SSC.47 The results of the fourth study were not displayed.28
Programme theory analysis
The included studies were critically appraised, using the CASP qualitative checklist as well as the RCT checklist.26 28 47 48 The quality of each of the studies was based on question 8 for both checklists.46 While only one of the studies had a high level of quality,48 two had moderate level of quality,28 47 and one had a low level of quality.26 The detailed checklists can be found in online supplemental appendix 4. Because all studies mixed the terms KMC, KC and SSC when providing information/evidence on KMC,26 28 47 48 it was difficult to develop and extract a strong conclusion on the barriers and facilitators of KMC. There was a lack of appropriate and relevant information to properly conduct a Realist Synthesis Review for KMC. Indeed, (1) none of the four included studies was specific to the KMC method/definition, (2) none provided information about strategic implementation in the UK, (3) none explored the potential barriers to KMC’s implementation, and (4) most of them used worldwide references to provide evidence and were thus not specific to the UK. Therefore, trying to understand ‘what is KMC, how does it work, for whom, in what circumstances, in what respects, and why’, in the UK, was not possible.
KC/SSC
As KC/SSC is a main component of KMC and aims to improve breast feeding (the second main component of KMC) we expanded our inclusion criteria to include KC/SSC as a proxy to understand the implementation challenges of KMC.16 Studies on both KC and SSC categories were included as the NHS guidelines use these two terms interchangeably.19 One hundred twenty-eight studies were retained but 105 were removed as not fulfilling the inclusion criteria. The remaining 23 studies were included for the analysis (figure 2; online supplemental appendix 5).
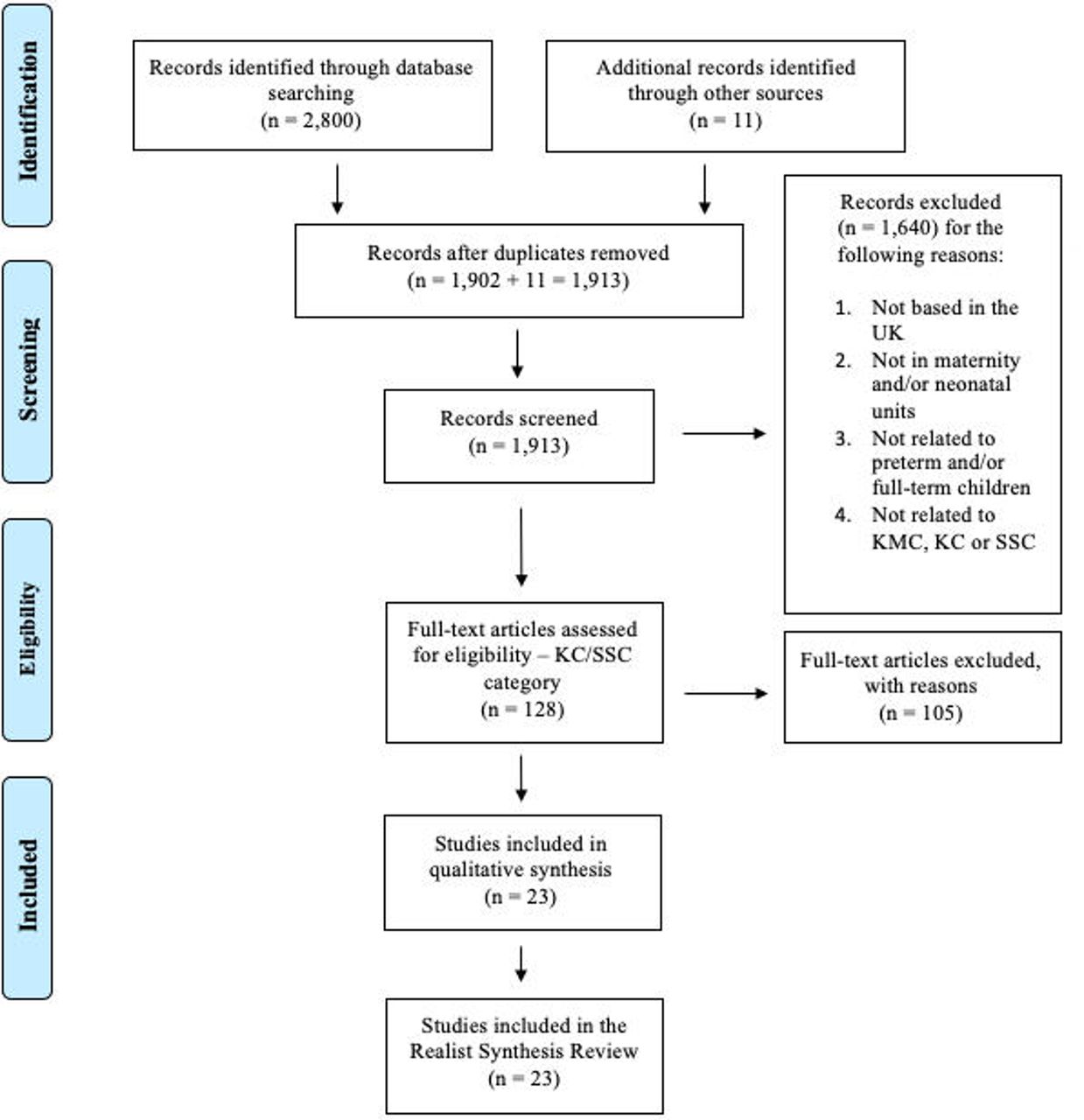
Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow chart—Kangaroo Care (KC)/skin-to-skin contact (SSC). KMC, Kangaroo Mother Care.
Pre–post cohort interventions,36 49 mixed-method study,50 qualitative study,51 participatory action research approach,52 53 interpretative phenomenological approach,54 literature review,55 56 surveys,30 57 58 audits59 60 and commentaries38 48 61–67 were included. The study population included (1) staff from neonatal and maternity units,36 50 51 58 60 64 65 (2) mothers in maternity units,54 63 (3) the whole family in neonatal and maternity units,38 48 56 59 (4) both parents and staff from neonatal and maternity services,49 52 53 55 57 62 67 or (5) no specific population.30 61 66
While some studies focus on SSC,48 49 51–56 60 61 63–66 others focus on KC.30 58 Certain authors also defined these two methods as being synonymous.36 38 50 57 59 62 67
A summary of the context, mechanisms and outcomes is provided below. The full data extraction form on these components is presented in online supplemental appendix 6.
Context
While all included studies referred to the UK, some focus on NICUs48 50–52 57–61 67 and others on maternity units.36 54 55 63
Mechanisms
Studies highlighted barriers in the implementation of KC/SSC which are the lack of training,50 51 58 lack of guidance/guidelines/policies,50 51 58 62 lack of confidence,50 58 60 fear,58 poor trained staff availability,50 time constraints,60 65 phototherapy,64 no guidance on humidification51 67 and instability of the child.51 58 Other barriers were perceived such as unwillingness from parents,51 58 difficulty to change the currently well-implemented routine of care,65 66 and inappropriate environment with lack of comfortable chairs and no private spaces.50 51 58 65 Finally, mothers may face different sociocultural barriers in the KC/SSC practice such as being culturally different (too rich or from ethnic minority),30 65 and having a blood phobia or being concerned to be dirty in front of family.54 Partners may also feel jealous of the mother–child bond, and this might make mothers feel guilty to practice such method.56 Midwives might have prejudices and may see breasts as being sexual which might further prevent the proper KC/SSC implementation.55 56 KC/SSC practice decreases from north to south in the UK with increasing hospital-based deliveries.30 66 67 Regarding enablers, the Bliss Baby Charter audit tool,59 61 informative tools for parents,48 63 training for staff and parents,48 51–53 59 63 67 SWCP,36 38 49 67 promotional/educative tools,48 52 53 59 63 67 written guidelines,48 67 comfortable chairs,67 multidisciplinary approach involving parents in ward discussions67 and the creation of a multidisciplinary team with trained staff are all facilitators in the implementation of KC/SSC.59
Outcomes
Eleven studies presented their outcomes in terms of increased KC/SSC practice.36 38 48 49 52 53 57 59 61 63 67 Three studies observed an increase in knowledge, confidence and number of trained staff.36 38 57 Finally, different studies proposed improvements such as to enhance training programmes, implement educational/informative tools both for staff and parents, apply changes in practice, remove any prejudices, improve the environment (reclining chairs, private spaces), and implement clear and coherent policies.50 51 54–56 58–60 62 65 66
Programme theory analysis
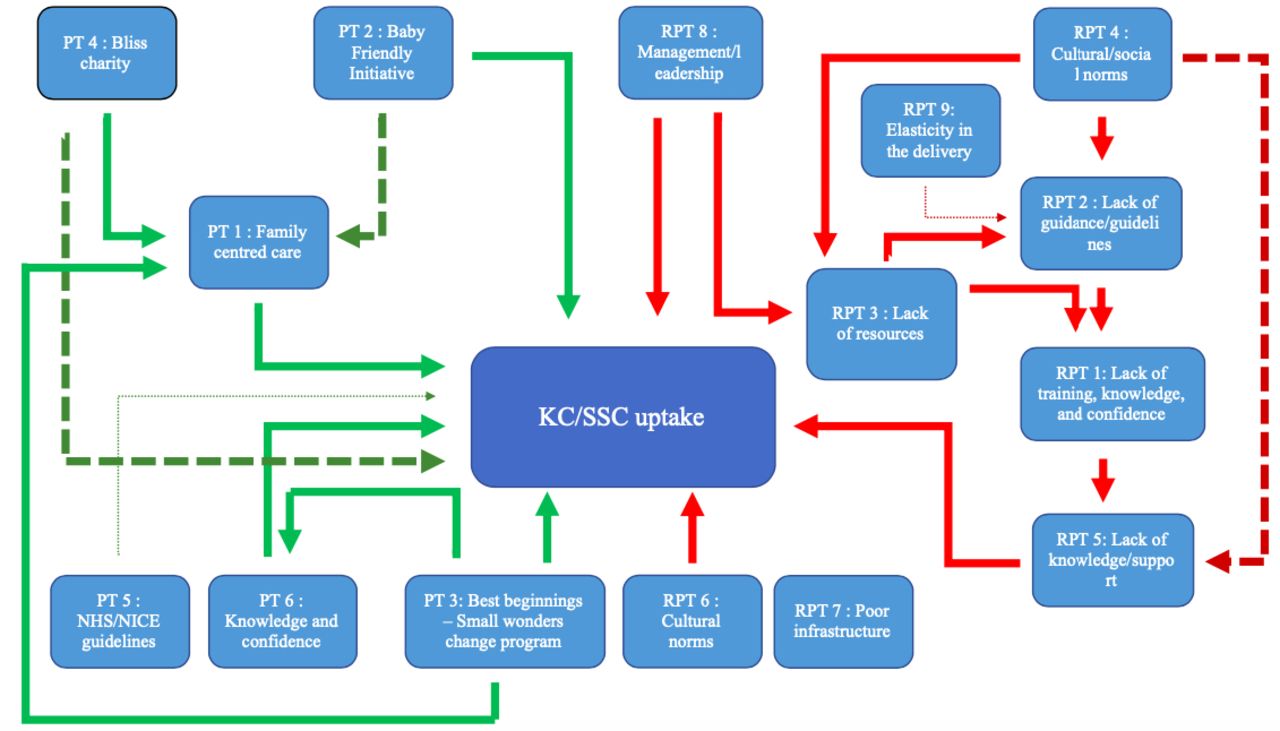
Using the same programme theories as for KMC but focusing on KC/SSC (figure 3), only the most supported/relevant programme theories are described below, with a complete description available in online supplemental appendix 7.

{kind=link}
{kind=link}
{kind=link}
Programme theory analysis—Kangaroo Care (KC)/skin-to-skin contact (SSC). Large dark green/red dotted lines: positive/negative impact on KC/SSC, added after having analysis the findings with the programme theories. Thin dark green/red dotted line: findings not highlighted in the analysis of the included studies. Normal lines: no change. The findings of the included studies confirm these hypotheses. The green/red lines are positively/negatively impacting KC/SSC uptake. NHS, National Health Service; NICE, National Institute for Clinical Excellence; PT, programme theory; RPT, rival programme theory.
Programme theory 1: family-centered care (FCC) and programme theory 4: Bliss charity
Several included studies confirm this theory, adding that FCC enhances the practice of KC/SSC.48 52 60 61 To encourage and promote FCC in neonatal units, Bliss charity has developed the Bliss Baby Charter audit tool which aims to enable units to define areas that need improvement. This tool, by enhancing FCC, improved the rate of KC/SSC practice.59 61 This charity also developed guidance and informative tools on KC/SSC to strengthen the practice of KC/SSC.48 62 67
Programme theory 2: BFI
Two studies observe that BFI accreditation, by promoting KC/SSC through the fourth and seventh steps, improves the uptake of this practice.63 65 Moreover, as FCC is a guiding principle of BFI, it encourages further the families to practice KC/SSC.50
Programme theory 3: best beginnings—SWCP
Findings from three studies confirm that the SWCP, involving an educative DVD for parents and staff as well as workshops, increases the confidence and knowledge of parents and staff and hence, improves the KC/SSC practice.36 38 49
Programme theory 6: knowledge and confidence
Different interventions, involving educational programmes (specific training, SWCP, educational sessions), have increased the practice of KC/SSC.36 48 52 53 57 59 Indeed, an increase in the knowledge and confidence has been observed to enhance the intention of staff to promote and initiate KC/SSC.36 68 Parental knowledge on KC/SSC is also paramount to improve the uptake of such method.38 48
Rival programme theory 1: healthcare workers: lack of training, knowledge and confidence
Knowledge and confidence play an essential role in the implementation of KC/SSC practice.50 Such skills are lacking in staff who have not followed a KC/SSC training and, hence, it limits its appropriate integration.50 Staff perceive the lack of training as an important barrier in the implementation of KC/SSC.50 51 62 No study indicated that attitudes towards reverse innovation and LMICs may act as a barrier in KC/SSC implementation in the UK.
Rival programme theory 2: healthcare workers: lack of guidance/guidelines
The lack of clear guidelines is an important barrier to implement KC/SSC.50 51 62 65 67 Without robust policies, staff lack information on timing, intensity, frequency and optimal environment which limits the integration of KC/SSC in the routine of care, and especially for high-risk babies.58 Therefore, there is a crucial need to implement strong guidance to enhance KC/SSC practice for all newborns with a special emphasis on high-risk babies that need intensive care as they are the majority in the UK high-settings neonatal units.51 62 65
Rival programme theory 4: healthcare workers: cultural/social norms
A barrier in the implementation of KC/SSC in practice is the difficulty to change the already well-implemented routine of care.55 65 66 According to some reports, preconceptions from midwives on nudity and on the sociocultural background of mothers may limit the willingness/choice of mothers to practice KC/SSC.54–56 While early bathing may be considered as a cultural norm limiting the opportunity for SSC, none of the included reports confirmed this issue.
The CASP ‘qualitative checklist’ was used to appraise the studies however not all the checklist questions were applicable. The quality of each of the study was based on question 8.46 For each of the programme theories, the level of quality is represented in the table 3. As PT 5 and RPT 15 were not supported by any included evidence, the level of quality was not applicable (N/A). The detailed checklists as available in online supplemental appendix 8.
Quality levels of the programme theories
Discussion
The four included studies on KMC did not permit a full review of the programme theories due to insufficient information and muddled definitions of the intervention used. Expanding the search to include KC and SSC found that lack of education, knowledge, confidence and clear guidance/guidelines are barriers in its implementation. Similar challenges are observed in other contexts/settings such as in the USA.69 70 Enablers included BFI, SWCP and FCC to strengthen KC/SSC practice, which is also observed in other countries.71 72
The disparity in the KMC definitions is a global issue.20 Indeed, even in Sweden, where KMC is well implemented in the routine of care,60 the KMC definition varies considerably.73 74 While the benefits of KMC are well known, particularly in stable children, the null finding regarding the barriers and facilitators on its implementation in the UK highlights how essential further work is needed to research its use in the UK. Both the NHS and the Bliss charity define KC and SSC as being synonyms.75 76 Clear definitions should be used for all studies related to either KMC, KC or SSC, within the UK and generally. Further work is needed to understand the timing, frequency and intensity of the KC/SSC, especially in clinically unstable and high-risk babies who need intensive care and humidification.54 55 58 60 63 65 66 BFI guidance, aiming to improve breastfeeding rates, has been developed at the national level in the UK, including recommendation that KC/SSC that should be practised as soon as possible and for as long as possible.63 However, only BFI hospitals follow these guidelines, preventing a consistent national integration of such practice.54 The lack of local guidelines, developed by the trust or by charities, undermines the spread of this intervention.62 Including KMC recommendations into BFI guidance as it already involves the KC/SSC and the breastfeeding components is an important opportunity. NHSE/I should develop a consistent guideline, for all services, to ensure that KMC practice is further integrated in the current healthcare system, as well as in healthcare educational programmes.16 26
Workplace culture is an important barrier for KC/SSC implementation and emphasis should be put on training programmes to overcome this challenge.65 Currently, there are few training programmes in England and none in Northern Ireland on KC/SSC.58 However, when educational tools are implemented as an intervention to improve such practice, results are positive.67 Improvements are needed to develop standardised training programmes and incorporate them further into neonatal/maternity services as well as to use this opportunity to educate both parents and staff on KMC, allaying fears or concerns that midwives or parents may have.54 We found evidence to suggest that parents’ knowledge, availability, and willingness to practice KMC is an important barrier.51 58 As they are the main drivers in its practice and that it asks for important commitment, it could be expected that it is a considerable challenge. This barrier may be further enhanced by poor staff knowledge, confidence and support.58 Educational training for parents and staff should be ensured and the promotion of KMC could be initiated from the moment mothers register in antenatal clinics. Including other HCWs in KMC promotion is important to ensure that parents have enough support without increasing the time pressure on nurses/midwives.27
The barriers of lack of guidance and specific training programmes are even more important when related to high-risk babies who need intensive care and where uncertainties remain regarding the timing, duration, and intensity of KMC for this population.51 58 As UK neonatal units are principally treating high-risk babies, guidance and training, while necessary, may not be sufficient to promote KMC in the UK. Other cultural/societal challenges (such as families with other children to take care of, working obligations, poor/far access to the units), may limit parental visits and, hence, the opportunity to practice KC/SSC/KMC.27 Moreover, neonatal units may not be designed with KMC in mind and therefore might not be suited to have a bed next to the baby which limit the possibility of parents staying as much as they want to.27 77 Creating mother–baby units for preterm children would potentially provide the needed privacy for mothers/fathers/caregivers to practice KC/SSC/KMC.27 The concept of ‘Mother-NICU’ units, where caregivers have a bed and chair at their disposal to enable immediate/intensive KMC, has been successfully implemented in Ghana, India, Malawi, Nigeria and Tanzania trial14 and Estonia.78 However, this will require significant investment and should be subject to a cost-effectiveness analysis. Use of KMC for unstable babies requires more evidence and research for use in the UK.
The findings exposed in this review may not accurately represent experiences, rather, it reflects what has been published. Indeed, there has been progress towards a supportive environment for KMC in the UK. First, the cultural practice of bathing the baby right after birth in the UK is becoming less important and is even often delayed in order to promote early SSC.79 Second, the Royal College of Nursing has included the need for KC training in the UK.80 Finally, replacing incubator care with KMC might be unrealistic in the UK as there will always be a place for their use in unstable babies where, for example, humidity, intubation and ventilation are required. Indeed, it may require a complete restructuring of NICUs architecture, drastic improvements in the duration and financial support of parental leave, and important changes in the UK culture where parents would be able to commit 24 hours per day with their babies on their chest. While incubators will probably always be part of the preterm baby’s routine of care, particularly for unstable babies, there are still opportunities to increase the research and practice around KMC to enhance its use and reduce the constant reliance on incubator care, while improving newborn and parent well-being. As a reverse innovation,81 being used extensively in other HICs (eg, Sweden)74 KMC offers significant potential for the UK.
Other HICs such as the Nordic countries, where KMC has been implemented in routine care, should be taken as example to help understand what the facilitators would be to enhance KMC practice within the UK.26 74 Various evidence exists on the strategies needed to properly increase the KMC implementation including focussing on parents’ knowledge, parents’ support, nurses’ training and confidence, and the facilities provided by healthcare systems (such as private spaces, opportunities to stay overnight and flexible visit policies).24 41 74 Moreover, embedding KMC in the national programme of maternal and newborn care would enable to have appropriate policies and guidelines, both necessary for a proper KMC implementation.24 41
This paper is the first to systematically review the opportunities and challenges of implementing KMC and KC/SSC in the UK; however, it does have several limitations. First, KC/SSC was used as a proxy to better understand KMC implementation. Studies that incorporate KMC as part of a wider programme of neonatal care, such as Family Integrated Care, may have been missed in our search. Second, KC and SSC have been used as synonyms, based on the NHS and Bliss definitions,75 76 and most of the included studies used these terms interchangeably. Third, the CASP checklist used was not always applicable and not all components could be answered. Finally, non-peer-reviewed papers were included which may limit the quality and robustness of this review.
Conclusion
No evidence was found regarding the barriers and challenges to scaling KMC in the UK suggesting that it is a poorly researched area. KC/SSC had to be taken as a proxy to better understand the barriers and facilitators to KMC. There are opportunities through hospital accreditation systems to embed KMC as a standard of care where adequate training, culture change and education is available to support mothers and clinical staff, and potentially in reducing reliance on incubator use for this well-established and cost-effective method for stable preterm babies. A clear definition for KMC use within the UK is needed to develop guidelines that are essential to improve newborns’ health. Putting KMC at the centre of a Mother-NICU investment programme will provide the needed space and privacy to practice this important intervention.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors GS designed the study, performed the database searches, screened, abstracted and analysed the data for relevant articles identified, completed the first draft, and revised subsequent drafts for important intellectual content and is the guarantor for the study. MS proposed the study, provided feedback on search terms and search results and revised all subsequent drafts for important intellectual content. CB revised subsequent drafts for important intellectual content. MH proposed the study, provided feedback on search terms and search results and revised all subsequent drafts for important intellectual content. All authors read and approved the final manuscript.
Funding The authors received no funding for this article. MH is supported in part by the NW London NIHR Applied Research Collaboration. Imperial College London is grateful for support from the NW London NIHR Applied Research Collaboration and the Imperial NIHR Biomedical Research Centre.
Disclaimer The views expressed in this publication are those of the authors and not necessarily those of the NIHR or the Department of Health and Social Care.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.