Article Text

Abstract
Introduction At the early epicentre of the COVID-19 crisis in the USA, our institution saw a surge in the demand for inpatient consultations for areas impacted by COVID-19 (eg, infectious diseases, nephrology, palliative care) and shortages in personal protective equipment (PPE). We aimed to provide timely specialist input for consult requests during the COVID-19 pandemic by implementing an Inpatient eConsult Programme.
Methods We used the reach, effectiveness, adoption, implementation and maintenance implementation science framework and run chart analysis to evaluate the reach, adoption and maintenance of the Inpatient eConsult Programme compared with traditional in-person consults. We solicited qualitative feedback from frontline physicians and specialists for programme improvements.
Results During the study period, there were 46 available in-person consult orders and 21 new eConsult orders. At the peak of utilisation, 42% of all consult requests were eConsults, and by the end of the study period, utilisation fell to 20%. Qualitative feedback revealed subspecialties best suited for eConsults (infectious diseases, nephrology, haematology, endocrinology) and influenced improvements to the ordering workflow, documentation, billing and education regarding use.
Discussion When offered inpatient eConsult requests as an alternative to in-person consults in the context of a surge in patients with COVID-19, frontline physicians used eConsult requests and decreased use of in-person consults. As the demand for consults decreased and PPE shortages were no longer a major concern, eConsult utilisation decreased, revealing a preference for in-person consultations when possible.
Conclusions Lessons learnt can be used to develop and implement inpatient eConsults to meet context-specific challenges at other institutions.
- hospital medicine
- health care quality
- access and evaluation
- health services research
- infectious disease medicine
- information science
This article is made freely available for use in accordance with BMJ’s website terms and conditions for the duration of the covid-19 pandemic or until otherwise determined by BMJ. You may use, download and print the article for any lawful, non-commercial purpose (including text and data mining) provided that all copyright notices and trade marks are retained.
https://bmj.com/coronavirus/usageStatistics from Altmetric.com
- hospital medicine
- health care quality
- access and evaluation
- health services research
- infectious disease medicine
- information science
Summary box
What are the new findings?
While eConsults are frequently used in the outpatient setting, this is the first report of a multihospital and multispecialty Inpatient eConsult Programme.
Our Inpatient eConsult Programme was designed to meet challenges in consultative demand and personal protective equipment shortages related to the COVID-19 pandemic.
This study demonstrated that Inpatient eConsult Programmes can be rapidly scaled to reach multiple specialties and achieve high adoption to meet increased consultation demands.
How might it impact on healthcare in the future?
Inpatient eConsults have the potential to improve efficiency and interprofessional communication in crisis and noncrisis times.
Our experience using quality improvement methodology to implement inpatient eConsults can serve as a roadmap for other institutions.
Introduction
The COVID-19 pandemic challenged the US healthcare system to rapidly adapt to care for an increased number of patients infected with the novel coronavirus. The unprecedented number of infected persons with multiorgan system failure,1 shifts and redeployment of workforce, shortages of personal protective equipment (PPE) and healthcare worker COVID-19 exposures presented new challenges in the ability to provide consultative evaluations. Based in the Bronx, with more cases per capita than any other borough of New York City,1 our medical system was the early epicentre of the crisis and saw a surge in the demand for subspecialty physicians with expertise in areas impacted by COVID-19.
The initial impetus for the development of electronic consultation (eConsult) programmes was a mismatch between supply and demand for specialty expertise in the ambulatory setting.2 These eConsult programmes facilitate patient-related communication between primary care providers and subspecialists, reduce the need for in-person encounters with patients and improve wait time to specialty expertise.3–6 Our health system successfully implemented an Ambulatory eConsult Programme in 2018 throughout our ambulatory care practices.7 During the COVID-19 pandemic, ambulatory eConsults provided a mechanism to sustain outpatient specialty care while in-person access was reduced.8
Despite widespread integration of eConsults into ambulatory care settings, there is a gap in knowledge about utilisation of inpatient multispecialty eConsult programmes. Reported use cases for inpatient eConsults include improving access to specialists for a remote hospital in a large healthcare system9 and implementation of a single-specialty Allergy and Immunology inpatient eConsult during the COVID-19 pandemic.10 Applying knowledge gained from our ambulatory eConsult experience, we conceptualised and implemented a new multispecialty Inpatient eConsult Programme in response to the COVID-19 pandemic.
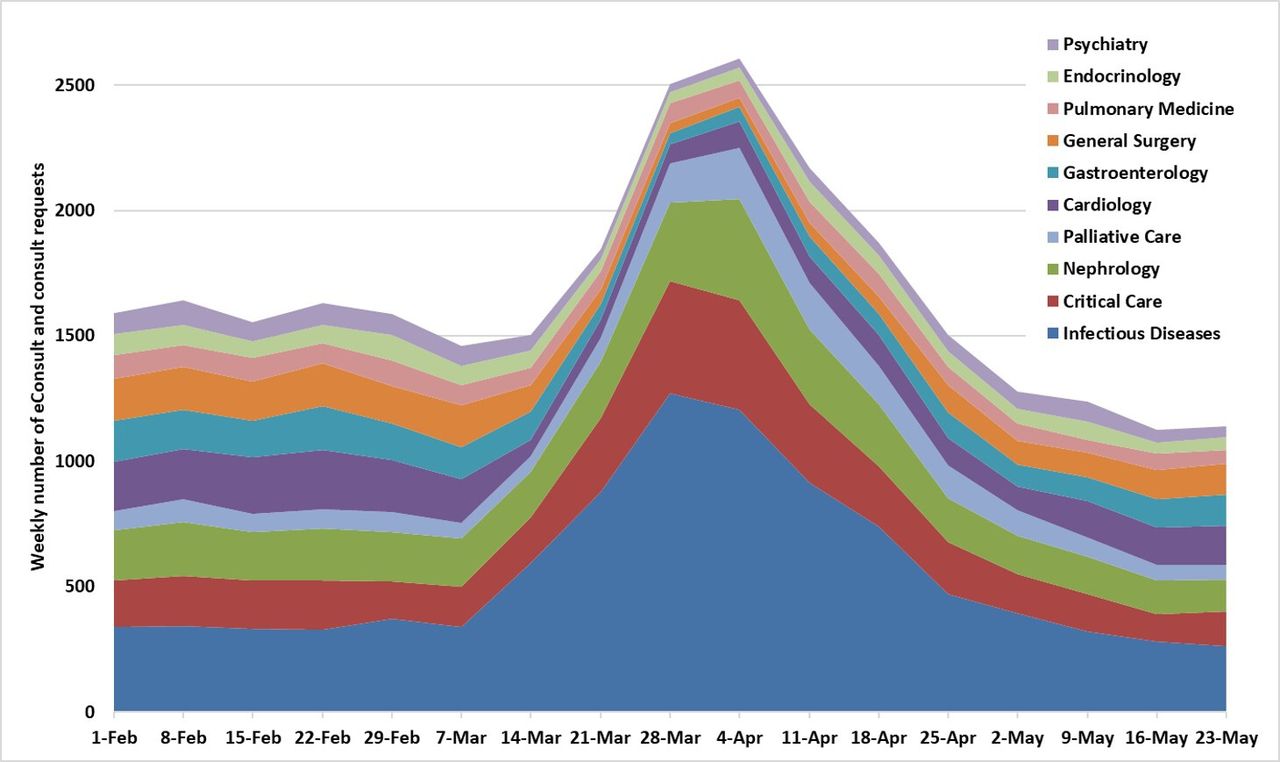
During the pandemic, our healthcare system increased inpatient capacity by greater than 50% and our system experienced rapid shifts in all aspects of hospital operations. A declaration of a stage 3 pandemic emergency status resulted in the deployment of residents, fellows and attending physicians from outside of hospital medicine and general internal medicine to assume frontline care of patients with COVID-19.11 Physicians experienced furloughs for COVID-19 exposure and increased childcare responsibilities from school closures. Compared with prior to the pandemic, there was an increase in demand for specialty consultations for infectious diseases, nephrology, critical care, palliative care (figure 1). We also had to incorporate evolving medical knowledge about the best treatment options for patients with COVID-19.

Weekly consult demand (eConsult and traditional in-person consult orders) for the 10 most frequently requested specialties before, during, and after the patient surge related to the COVID-19 pandemic.
We aimed to provide timely specialist input to all consult requests during the COVID-19 patient surge by offering a new Inpatient eConsult Programme. This implementation study evaluates the reach and adoption of inpatient eConsults compared with traditional in-person consults. We hypothesised that after implementation and scaling of inpatient eConsults, frontline hospital providers would increase inpatient e-consult requests as an alternative to in-person consults. Our experience rapidly developing and implementing an Inpatient eConsult Programme while simultaneously responding to new patient needs can inform care at other institutions facing challenges with meeting inpatient consult demand.
Methods
Study design and setting
This quality improvement initiative and implementation study took place from February to May 2020 at our institution, an academic medical centre with multiple hospital locations serving mostly publicly insured patients and a tertiary referral centre for lower New York State. This study was approved by the Montefiore/Albert Einstein Institutional Review Board.
Intervention
In March 2020, anticipating an influx of COVID-19-related questions, the Division of Infectious Diseases worked with the information technology department and the Ambulatory eConsult Programme leadership to develop an inpatient eConsult workflow. An eConsult is an interprofessional communication care modality provided by a consultative physician, which includes a written report to the patient’s treating physician or other qualified healthcare professional.12 These services take place without in-person or video evaluation of the patient by the consultant and include eConsult-specific documentation and billing considerations. The requesting provider needs to obtain and document verbal consent from the patient or healthcare proxy for the use of eConsults. The consulting physician should document (1) the reason for consultation, (2) findings from the medical records, (3) further evaluation and/or treatment recommendations and (4) the time spent reviewing the record and speaking with the requesting physician (if applicable). We worked with our professional services and information technology teams to implement the billing codes associated with these interprofessional services into the inpatient workflow: CPT 99451 if only written communication, 99 446-9 if both written and verbal communication with the requesting team. If the patient requires an in-person evaluation within 14 days of the eConsult, the eConsult is no longer a billable encounter. Key elements of inpatient eConsults and comparison with traditional in-person consults are outlined in table 1. Faculty participating in e-consults accrued work relative value units as part of their clinical compensation plans.
Comparison of traditional in-person subspecialty consultative programme and new Inpatient eConsult Programme
The Inpatient eConsult for COVID-19 order was added as an alternative to the pre-existing in-person consult order for infectious diseases. When a primary team identified a need for specialty expertise, they could order either a consult or an eConsult. EConsult orders from multiple hospital locations populated a single eConsult list that was reviewed by a newly created eConsult specialist team. These specialists used an eConsult note template that allowed for a free text response to the eConsult question and a statement of time spent providing the service. Primary teams could review completed eConsult notes in patients’ electronic medical record in the same section as in-person consultation notes. To facilitate system learning and standardisation of medical care, a COVID-19 admission order set was created, which included the Inpatient eConsult for COVID-19 order. Feasibility was tested by piloting inpatient eConsults for this one subspecialty.
As the number of hospitalised patients with COVID-19 rapidly grew, there was a need to conserve PPE and reduce potential in-hospital spread of COVID-19. To help alleviate these shortages, we expanded the inpatient eConsult programme, led by physicians with expertise in patient care, administration, quality improvement, documentation and coding and clinical informatics. We identified other specialties that could benefit from an eConsult option: specialties with increased demand or specialties that could answer questions without direct patient interaction for the first cycle of eConsult options.
A unique feature of our programme was the creation of eConsult orders for defined questions rather than a specialty. Physicians in the divisions of Allergy and Immunology and Rheumatology recognised a need for a unified approach for questions about COVID-19-related cytokine release syndrome, which led to the creation of a specialised eConsult order for cytokine release syndrome managed by physicians from both those divisions. The creation of such interdisciplinary teams allowed for better clinical care and created a network for research collaborations.
Implementation of the new eConsult specialty orders was accomplished in using the Model for Improvement quality improvement framework (eg, plan, do, study, act).13 New specialty eConsult orders were implemented in cycles based on interest and readiness of subspecialty divisions. After each cycle, we evaluated utilisation and solicited feedback to make programme improvements. Table 2 displays the timeline of activities related to developing, implementing and refining components of the Inpatient eConsult Programme. Each subspecialty designated a physician-champion to assist in disseminating information to their division and managing subspecialist schedules for answering eConsult questions. Based on subspecialty and frontline physician feedback, we made frequent adaptations to the intervention. Changes to the programme workflow included creating note templates with required documentation, allowing participation of physicians-in-training such as fellows, as well as incorporating billing using interprofessional communication charges. All process changes were communicated daily via e-mail and conference call updates to frontline medicine teams.
Timeline of development and implementation of Inpatient eConsult Programme
Implementation measures and analysis
We used the reach, effectiveness, adoption, implementation and maintenance (RE-AIM) implementation science framework to assess the inpatient consult programme.14 This framework provides ways of measuring key factors involved in evaluating interventions for impact and application. We focused on the dimensions of (a) reach: how many specialties participated and reasons why or why not, (b) adoption: the proportion of consultation requests using eConsults after implementation and (c) maintenance—trends in eConsult use over time.
To assess adoption and maintenance, we used a run chart analysis to evaluate the weekly proportion eConsults per all specialty consults requests (eConsult and traditional in-person consult request) for all specialties participating in the Inpatient eConsult Programme. A run chart allows the evaluation of the impact of different interventions and tests of change over time.13 15 There are probability-based rules to objectively analyse a run chart for evidence of nonrandom change in a measure based on alpha level of p<0.05. A shift is identified if six or more consecutive points either all above or below the median and a trend is identified if five or more consecutive points all going up or down.15
To assess reach, specifically, barriers to and facilitators of using eConsults, we solicited early and ongoing general feedback about the programme from physicians from subspecialties, hospital medicine and general internal medicine. A group e-mail chain was started for physician leads from each participating eConsult subspecialty in which the Inpatient eConsult Programme leadership requested collaborative feedback to make iterative workflow improvements. Daily and weekly conference calls were held for frontline physicians from hospital medicine and general internal medicine during which information about the Inpatient eConsult Programme was shared and physicians had opportunities to share their experiences and offer suggestions for improvement.
Results
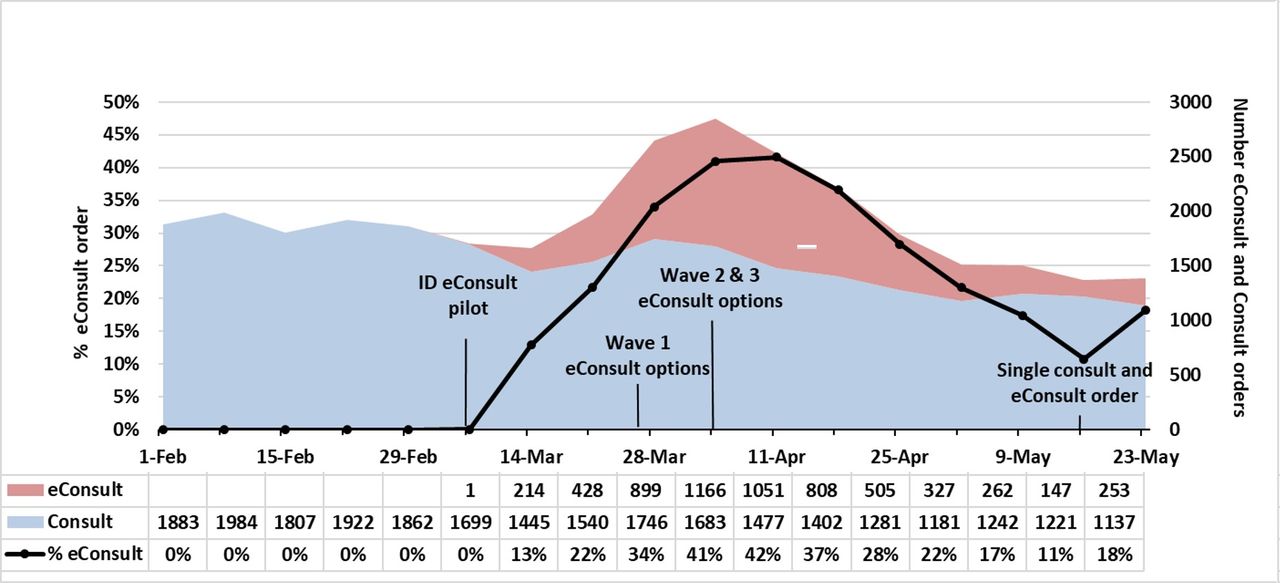
From February to May 2020, frontline physicians ordered 6061 eConsults and 26 512 traditional in-person consults. During the study period, there were 46 available subspecialty consult orders and 21 subspecialty eConsult orders. Our first patient with COVID-19 was diagnosed early March 2020 and by May 2020 all internal medicine sub-specialties and many other subspecialties were participating in the Inpatient eConsult Programme (table 2). For subspecialties participating in eConsults, the number of traditional in-person consult orders per week trended downward beginning the week beginning 28 March 2020 and shifted below the median the week begining 11 April 2011. The number of eConsult orders per week initially trended upward, peaking the week beginning 4 April 2020 and subsequently trended downward (figure 2). The proportion of eConsults per all consult orders trended upward from 0% the week beginning 7 March 2020 to a peak of 42% the week beginning 11 April 2020 followed by a decrease and eventual plateau below 20% (figure 2).

{kind=link}
{kind=link}
eConsult and traditional in-person consult orders over time during the implementation of the Inpatient eConsult Programme in the context of the COVID-19 pandemic. The weekly proportion of eConsults per all consult orders is shown on the primary axis in black, the combined weekly frequency of eConsult (in red) and in-person consult (in blue) orders is shown on the secondary axis.
Feedback from frontline physicians and subspecialists highlighted some of the benefits of the new Inpatient eConsult Programme. For frontline physicians, this included timely responses to questions well suited to eConsults, such as those about antibiotic choices, insulin administration or anticoagulation. For subspecialists, eConsults required less time than an in-person consultation, allowing them to evaluate more patients. Subspecialists also had increased flexibility to answer questions outside of typical hours, between other clinical duties or while at home due to COVID-19 exposure, recovery or increased childcare responsibilities.
Critiques about the programme also influenced improvements. At the onset of the programme, primary teams could decide which type of consult to request. We saw inconsistent adoption of the eConsult order, with some frontline physicians making case-by-case decisions of when to use the option, some using only eConsults and others unaware of the eConsult option. We allowed specialist to use their discretion in mode of response to consultation request, as subspecialists doing consultations recognised that many traditional in-person consult orders could be answered using the eConsult pathway. However, frontline physicians observed that some of the subspecialty consultation requests that were converted to eConsults would benefit from in-person evaluations. To address these issues, a single consult order was developed within which requestors can specify whether they require a traditional in-person consult or eConsult. Subspecialists will honour the request for in-person consults; however, they can decide to perform an in-person consult regardless of the selection from the ordering team. This has remained the consultative services ordering pathway at our institution.
Discussion
We rapidly developed, implemented and achieved medical centre-wide adoption of inpatient electronic subspecialty consults in response to the COVID-19 pandemic using a continuous quality improvement framework. When offered eConsult orders as an alternative to traditional in-person consult orders in the context of a surge in patients with COVID-19, frontline physicians used eConsult orders and decreased use of traditional in-person consult orders. As the demand for consults decreased and PPE shortages were no longer a major concern, eConsult utilisation also decreased, revealing a preference for in-person consultative care when possible; however, eConsults have remained a part of clinical care. While there are a few reports of inpatient eConsults used in settings of remote hospital locations or for single specialties,9 10 to our knowledge, this is the first report of implementing a multihospital multispecialty Inpatient eConsult Programme.
Successful implementation of the Inpatient eConsult Programme was facilitated by collaboration between interdisciplinary teams motivated by a sense of urgency. Because we had experience implementing our Ambulatory eConsult Programme,7 we were able to quickly bring together team members from information technology, professional services, billing compliance. Specifically, we had buy-in from subspecialty physicians familiar with delivering this type of indirect patient care. Those without experience performing eConsults may be concerned about the time commitment of responding to eConsults in addition to regular clinical demands. In our system, we did see an increase in total consultation requests; however, we believe this was driven by increased patient volume related to COVID-19 rather than induced demand for eConsult questions. Additionally, subspecialists in our system report that prior to eConsults, they were answering comparable ‘curbside questions’ outside of the electronic health record and appreciated having this work formalised. Similar to our ambulatory experience, we found that some specialties and questions lent themselves better to eConsults than others. Particularly, high-yield specialties included Infectious Diseases for the expertise needed to navigate the evolution of evidence-based medicine for COVID-19, nephrology for kidney failure and initiation of renal replacement, haematology for COVID-19-related coagulation disorders and Endocrinology for assistance with glycaemic control either as a direct result of COVID-19 infection or from steroid-induced hyperglycaemic. Less well suited for eConsults were urgent requests for Gastroenterology and mental health questions requiring psychiatric interviews. Despite the ability for primary teams to take and upload pictures of skin findings, we also found that eConsults were challenging for Dermatology or Wound Care questions.
Limitations of this study include the inability to rigorously collect feedback from physicians and patients during the period where eConsults were most used. Because staff were coping with extraordinary tasks, they were unlikely to participate in questionnaires or focus groups. Thus, we are not able to evaluate response rate and thus do not know whether the feedback we received can be generalised to the experiences of everyone at our institution. Additionally, there may be recall bias for physician-reported feedback such as time spent completing an eConsult compared with an in-person consult. However, iterative, informal feedback and flexibility led to continuous improvements to achieve widespread and acceptable utilisation of this new way of delivering indirect patient care in the inpatient setting. We faced challenges of disseminating information to a growing and changing group of physicians both working at the frontline and providing consultations leading to inconsistent use of both the eConsult order and eConsult note template. This may have resulted in misclassification of the type of consult orders with how they were completed by the specialists (eg, a traditional in-person consult order to Infectious Diseases could have been completed by the specialist without seeing the patient). We also grappled with new ethical considerations such as thinking about which team members would be at risk or be able to avoid risk of exposure to a contagious respiratory disease.
Conclusion
A robust Inpatient eConsult Programme allowed us to continue delivering timely patient care in the context of increased demand for subspecialty expertise and shortage of PPE during the COVID-19 pandemic. We believe that inpatient eConsults have the potential to improve efficiency and interprofessional communication even in noncrisis times. There is still much to learn from the Inpatient eConsult Programme such as evaluating financial sustainability, educational ramifications for medical trainees and quality of patient care. We have returned to predominantly traditional in-person consults; however, we retained eConsult for value-added questions, which may not require in-person evaluation. Inpatient eConsults remain an important model to deploy if we face another COVID-19 surge. We hope that our experience with development and implementation of inpatient eConsults can serve as a roadmap for other institutions.
Footnotes
Twitter @SharonRikinMD
Contributors SR, IG and EJE made substantial contributions to conception and design of the work, acquisition and interpretation of data for the work, drafting and revising the work.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Data availability statement Data are available upon reasonable request. Deidentified participant data may be available upon reasonable request from study author srikin@montefiore.org.