Article Text

Abstract
Background Children’s health and healthcare use are impacted by both medical conditions and social factors, such as their home and community environment. As healthcare systems manage a pediatric population, information about these factors is crucial to providing quality care coordination.
Methods The authors developed a novel methodology combining medical complexity (using the Pediatric Medical Complexity Algorithm) and social complexity (using available family social factors known to impact a child’s health and healthcare use) to create a new health complexity model at both the population-level and individual-level. System-level data from Oregon’s Medicaid Management Information Systems and Integrated Client Services database was analysed, examining claims data and service utilization, to calculate the health complexity of children enrolled in Medicaid/Child Health Insurance Program (CHIP) across Oregon.
Results Of the 390 582 children ages 0 to 17 enrolled in Medicaid/CHIP in Oregon from July 2015 to June 2016, 83.4% (n=325 900) had some level of medical and/or social complexity and 22.1% (n=85 839) had health complexity (both medical and social complexity). Statistically significant (p<0.05) differences in health complexity were observed among attributed patients by Oregon’s 16 Coordinated Care Organizations, as well as by a child’s age, county of residence and race/ethnicity.
Conclusions Given the high proportion of children with health complexity, these findings demonstrate that a large number of Medicaid/CHIP-insured children could benefit from targeted care coordination and differential resource allocation. Reports have been shared with state, county and health system leaders to drive work across the state. This paper describes the collaborative process necessary for other states considering similar work.
- health services research
- pediatrics
- child health
- population
- socioeconomic factors
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Population-level data is necessary to understand needs, drive investments and support models of care that provide best match services for a child in the context of their family’s needs and resources.1 2 Frontline provider experiences, healthcare systems and evolving research has demonstrated how much patients’ health and healthcare utilisation can be impacted by both their medical conditions and social factors.3–5 Particularly for children, their health and development are significantly influenced by their family, home and community environments.4 A child’s health trajectory and care coordination needs can vary dramatically based on these settings, including the cumulative effects of stress and trauma.6
This paper describes an approach used by the Oregon Health Authority (OHA), with consultation and technical assistance from the Oregon Pediatric Improvement Partnership (OPIP), to develop and operationalise a standardised methodology using paediatric population-level data to quantify and describe the health complexity of Medicaid/Child Health Insurance Program (CHIP) insured children. Health complexity is a concept that considers both the child’s medical and social complexity, including family factors that can impact the child’s health and healthcare use.7 The novel data and data sharing are then meant to inform efforts that can better target supports and services so that all families are equipped with the resources they need in order for their children to thrive.
Health systems have focused attention on identifying and managing populations of children and providing best match supports, care coordination, and when necessary, complex care management. Care coordination has traditionally been based on a child’s medical complexity, with goals of improving health outcomes, maximising resources and controlling healthcare costs.8 However, it is imperative to also understand the child’s and family’s strengths as well as challenges they face in their environment in order to best serve them.9–11 In this context, targeted care coordination could include social workers, systems navigators, nurses, community health workers and others.
Population management and targeted coordination services are particularly important for Medicaid agencies that insure a large number of children, are under financial restraints and need to maximise funds to provide quality care and control costs.12 13 Many Medicaid agencies use managed care contracts, risk-based contracts and value-based payment models.14–16 Within these types of contracts, it is critical to identify specific populations to receive supports intended to help control costs.17 Medicaid also partners with various state and public health agencies to address population health needs and to inform state and local resource allocations addressing health at the individual-level and population-level.14 18 19
The concept of health complexity leverages system-level data from various sectors, including healthcare and social services, and combines information at the child level. We highlight state-level findings and describe how this data has been shared, for the first time, with state, county and health system leaders to guide and inform efforts focussed on children. Lastly, we share our real-world challenges and barriers in obtaining, using and disseminating the data and priorities for future efforts to sustain, improve and scale the work.
Methods
With support from Lucile Packard Foundation for Children’s Health, OPIP built off work led by the Center of Excellence on Quality of Care Measures for Children with Complex Needs (COE4CCN)8 20 21 and learnings from consultation to Kaiser Permanente Northwest (KPNW) in developing a paediatric complex care model22 to operationalise indicators of medical and social complexity. These efforts helped identify specific factors that can impact children’s health, whereas many current models are more widely used for adults. OPIP also facilitated three meetings of public and private stakeholders invested in child health to obtain feedback about the proposed data methodologies and data sharing activities. These meetings included health system leaders, policymakers, representatives from Coordinated Care Organizations (CCOs) that OHA contracts with to provide managed care to a majority of publicly insured children, child and family advocates and parents of children with varying levels of health complexity.
The OHA Health Analytics, Health Systems and Policy and Transformation Centre teams obtained and analysed data to generate aggregate reports.
The medical complexity component was operationalised using the Pediatric Medical Complexity Algorithm (PMCA).23 OHA examined services over a 3-year period using the ‘more conservative’ version of the algorithm due to the high quality of Oregon’s Medicaid Management Information Systems (MMIS). Children are grouped into one of three categories: (1) Complex with chronic conditions; (2) Non-Complex, with chronic conditions; or (3) Healthy, which are co-linear with cost (as complexity increases, so does cost).
The social complexity indicators were anchored to the COE4CCN definition of social complexity: “A set of co-occurring individual, family or community characteristics that can have a direct impact on health outcomes or an indirect impact by affecting a child’s access to care and/or a family’s ability to engage in recommended medical and mental health treatments.”24–26 The COE4CCN identified factors from the literature and their studies that were correlated with worse outcomes or higher healthcare costs.25–28 In collaboration with the Department of Human Services (DHS) Office of Reporting, Research, Analytics and Implementation (ORRAI), the Integrated Client Services (ICS) database was accessed to determine which factors could be collected for Oregon’s pediatric Medicaid/CHIP population. ICS database contains individual-level data about clients served by most DHS and OHA programmes to create an inter-agency view of clients and services to support budget planning and forecasting analysis. These include: (1) DHS programmes—Ageing and People with Disabilities, Child Welfare, Developmentally Disabled, Self-Sufficiency and Vocational Rehabilitation; (2) OHA programmes—Alcohol and Drug, Contraceptive Care, Family Health Insurance Assistance Program, Healthy Kids Connect, Medical Assistance Programs, Mental Health and Women Infants and Children; (3) Department of Corrections; and (4) Oregon Housing and Community Services.
With input from stakeholders at meetings in November 2017 and April 2018, OPIP and OHA examined the factors identified by COE4CCN and determined there to be 12 indicators of social complexity that were accessible in the MMIS or ICS databases: five based on information specific to the child and seven based on service utilisation or enrolment information for one or both parent(s). Children were linked to parents using vital statistic data when possible, and the prevalence of parent-level indicators any time during the child’s lifetime or prenatal period was assessed. A summary count of the total number of indicators identified for each child was then calculated. For about 20% of children, it was not possible to link the child to either parent. Therefore, these children only have data available for the five child-level social complexity indicators. A detailed description of the source for each variable can be found in the publicly available OHA data dictionary.29
The medical and social complexity variables were then used to create a novel nine-part health complexity categorical variable, where children are categorised by levels of medical complexity combined with levels of social complexity. For this reporting construct, the social complexity indicator count was collapsed into three categories: (1) no indicators, (2) 1 to 2 indicators or (3) 3+ indicators identified. The decision to create this grouping was threefold: (1) need for manageable categories for aggregate reports; (2) because of overlapping categories for child and parent factors (ie, both child and parent on Temporary Assistance for Needy Families (TANF)), having 1 to 2 social indicators could represent the same factor, therefore 3+ indicators mean the child has at least two different categories of social complexity; and (3) to align with the literature on the cumulative effect of multiple factors is associated with worse health outcomes.30 31 The three PMCA categories for medical complexity are then combined with the three categories of social complexity to create a matrix of nine categories of health complexity.
Results
Table 1 provides an overview of the medical and social complexity indicators developed, data sources used and population-level findings for the 390 582 Oregon children ages 0 to 17 insured in Medicaid/CHIP from July 2015 to June 2016. For medical complexity, 24.4% (n=95 272) had either a complex chronic condition or non-complex chronic condition (table 1).
Data methodology, data sources and findings of the medical and social complexity indicators
For social complexity, 38.9% (n=155 048) had three or more social complexity indicators (figure 1). The most common indicators were significant poverty indicated by the access of TANF (40.6%, n=158 650), parental access of mental health services (40%, n=156 221) and parental access of substance abuse services (29%, n=113 124) (table 1). Twenty per cent of children were not able to be linked to either parent and only have data available for the five child level social complexity indicators, which likely leads to an underestimate of family factors.

Distribution of number of social complexity indicators. The data findings presented are based on the Medicaid/CHIP Medicaid Management Information System and Integrated Client Services data accessed for Oregon’s children 0-17 years old enrolled in Medicaid/CHIP from July 2015 to June 2016. CHIP, Child Health Insurance Program.
Table 2 provides a summary of the state-level health complexity findings. While only 3% (n=11 637) of children have both high medical complexity and high social complexity (category 1, in green), over 85 000 children ages 0 to 17 have health complexity with some level of both medical and social complexity (categories 1,2,4, and 5, in green). Conversely, only 16.6% (n=64 682) of children were in category 9 (in white) with no medical or social complexity based on system-level findings.
Nine-part health complexity variable and state-level findings for children enrolled in Oregon Medicaid/CHIP
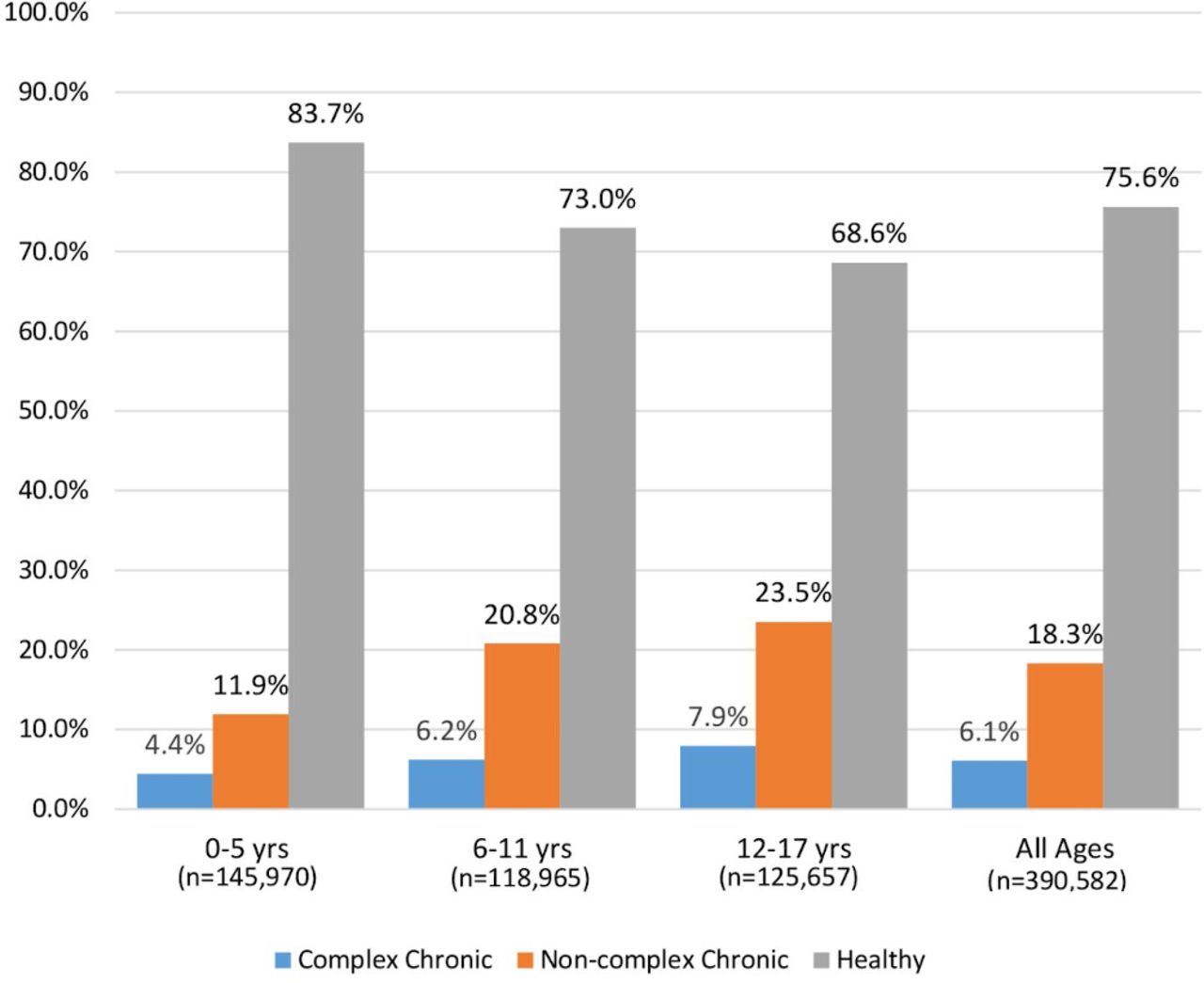
The rates varied by age of child, county of residence and race/ethnicity. Figure 2 highlights the differences in medical complexity findings by age of child. Children ages 0 to 5 tended to be healthier than children ages 12 to 17. Likewise, younger children tended to have fewer social complexity indicators than older children across all 12 indicators (table 3).
Social complexity by age of child
{kind=link}
{kind=link}
Pediatric Medical Complexity Algorithm findings: by age of child. The data findings presented are based on the Medicaid/CHIP Medicaid Management Information System and Integrated Client Services data accessed for Oregon’s children 0-17 years old enrolled in Medicaid/CHIP from July 2015 to June 2016. CHIP, Child Health Insurance Program.
Public reports of the data at the state-level, CCO-level and county-level were disseminated on the OHA website.28 Each CCO received two data components: (1) Aggregate Report: Showing findings for the population of children attributed to the CCO and (2) Child-level Data File: For children attributed to the CCO, three sets of variables: (1) PMCA category; (2) Three social complexity count variables listing the child, family and combined total; and (3) Nine-part health complexity categorical variable.
Discussion
State, community, and health system leaders have used the data to inform their understanding of and work needed for children.
State-level policymakers
OPIP and OHA leadership presented the data to several policymaking entities, including Governor Kate Brown’s Children’s Cabinet, Oregon Health Policy Board (OHPB), Early Learning Council (ELC) and Title V Leadership. Child health complexity data was available to policymakers and community-level stakeholders during the development of the 2020 to 2024 contracts of Oregon’s CCOs and helped inform OHA’s priorities for children’s health and policies, including a focus on behavioural health and social determinants of health. The OHPB selected child health as one of their priority areas. System-level leaders are considering how to use the data to inform rate setting, value-based payment models and investments in resources that serve children with health complexity.
The data was also provided to the ELC to inform their development of ‘Raise Up Oregon: A Statewide Early Learning System Plan’ for 2019 to 2023.32 Within this strategic plan are ways leaders from early childcare and education, K-12, health, housing and human services—together with families, communities, and public and private sectors—can work together to improve outcomes for young children.
Data for community leaders
Facilitated by OPIP local county-level public health agencies, Early Learning Hubs,32 and people working on community-level health improvement plans, have used the data to identify priorities for cross-sector, population-based efforts. For example, investments were made by the Early Learning Hub of Central Oregon, public health and the Central Oregon Health Council for a 2-year effort focussed on young children including piloting specific strategies to build health and resiliency in young children that have high social complexity and developing behavioural health strategies that are dyadic, including both the caregiver and child. At community-level meetings, stakeholders have raised significant concern about the lack of capacity and resources to address the high levels of health complexity observed. The data has also identified the needs of children and the relative inequity of available resources in rural regions and of specific cultures, races and ethnicities.
Data for CCO leaders
Following OPIP-facilitated learning sessions with CCOs, in which parents of children with various levels of health complexity and leaders of complex care management models shared their experiences, the data has been used in several different ways. These activities include: (1) Using the data to stimulate conversations with contracted partners, community-level leaders and patient and family advocates; (2) Comparing children identified via the health complexity data with those already receiving CCO-supported complex care management services, examining gaps and creating targeted care coordination investments; (3) Examining the data by the primary care home to which the child is attributed and considering the implications for investment and supports; (4) Advocating for and hiring paediatric case managers and system navigators to better care for their attributed population; (5) Using the data to highlight the need for trauma-informed and culturally-responsive resources; (6) Identifying populations for secondary assessments, in an effort to identify strength and resiliency factors and to determine care needs; and (7) Financing care coordination models that engage hospital systems and tertiary centres as the data highlighted that children with high medical complexity are likely receiving the majority of their care in those centres.
Challenges/learnings
Since the inception and dissemination of the health complexity data, there have been some challenges and learnings.
Data is limited to enrolment and service utilisation
The system-level data is limited to enrolment and service utilisation, which represents an incomplete view of the needs of children and families. Second, patients who do not or are not able to access services may appear less ‘complex’. Data is limited to events within Oregon and children born outside of Oregon could not be linked to their parents via birth certificate documentation.
Need to enhance a focus on strength and resilience
High social complexity may indicate a need for enhanced resources or care coordination, but may also reflect the resiliency and navigation skills of families in seeking services they need. Learning is needed from children and families who are in support-services and thriving, despite their high social complexity. To reduce the risk of traumatising, marginalising or stigmatising communities with high rates of social complexity it is necessary to use a trauma-informed approach when reviewing data, as well as addressing needs for culturally and linguistically responsive services.
Need for ongoing and enhanced family and youth engagement
While a significant effort was made to gather family partner feedback through the development and implementation of this work, we feel this should be an even stronger priority going forward to understand individual-level and community-level needs and resiliency.
Conclusion
Oregon is still in the beginning phases of maximising the use of this system-level data and improving the data’s accuracy, relevance and meaningfulness to guide investments and resources. Efforts are currently underway to address the challenges and barriers noted.
What is measured is what is focussed on, and the health complexity data has engaged system leaders to think about the needs of children and to consider the impact of their environment on their health and healthcare use. The health complexity data has also stimulated conversations on best match care coordination and complex care management models for children that address these factors. OHA is considering how the health complexity data can inform approaches to state-level reporting of metrics that drive improvements in inequities and address disparities in care, including gaps in service availability to address socially complex families.
Policy level improvements and payment models are needed to align priorities and resources with a health complexity-informed approach. This could include value-based payment models that support family-based approaches to care. Health complexity-informed, differential payment models could greatly improve care for a vulnerable population of children.
As we continue to explore how to use the system-level data to address children’s social determinants of health in healthcare, it is important to maintain a focus on the overarching goal: that families are equipped with the resources they need for their children to thrive. To achieve this goal, authentic family engagement will be critical. Oregon has found that leadership support, wide-spread dissemination and varied stakeholder use of the data have created engagement and interest in continuing this work. With the up-front establishment of the health complexity model, analysis processes and data agreements completed, sustainability is more likely. All states with quality MMIS systems can replicate the medical complexity component of our work, and those with versions of ICS could replicate the process of identifying social complexity indicators and create a health complexity model for their paediatric population.
Acknowledgments
We would like to thank Brooke Latze-Davis and Madelynn Tice for their assistance in the literature review, formatting and editing of this manuscript.
References
Footnotes
Contributors CPR led the conceptualisation and development of this paper and was involved in all components of the article. She was the Principal Investigator on efforts specifically focussed on the development of the health complexity methods and supporting health system use of the metrics. JC oversaw the OHA Health Analytics team that conducted the medical complexity analysis and disseminated the reports, provided suggestions for edits to the article and approved the inclusion of the data findings and information about OHA uses of the data. LC co-led the development of the article structure and framework and led the writing of specific components of the article. LC was involved in all aspects of OPIP-led efforts. VS provided suggestions for edits to the document and oversaw the team within OHA Health Analytics who worked on the health complexity data. ACC provided suggestions for edits to the document and led the work within Office of Reporting, Research, Analytics and Implementation that related to the use of the ICS data. CWC provided suggestions for edits to the document and was a member of the OHA Health Analytics team. DS provided suggestions for edits to the document and was a member of the OHA Health Analytics team. DH provided suggestions for edits to the article, approved the inclusion of the data findings and information about OHA uses of the data and led several policy efforts and presentations to policymakers described in the article. All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Funding This study was funded by Lucile Packard Foundation for Children’s Health.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available in a public, open access repository. Data are publicly available on the Oregon Health Authority website.