Article Text

Abstract
Objectives Telephone consultations are frequently used in the outpatient setting in order to avoid unnecessary travel and to reduce hospital visit-related costs for patients. However, they are limited by the absence of non-verbal communication in contrast to video consultation. Little is known considering the possible advantages of using video consultation in comparison to telephone consultation according to both patients and healthcare providers.
Methods Patients with colorectal diseases were asked to choose between a telephone consultation or a video consultation for their next appointment at the outpatient clinic of a tertiary referral centre. Willingness to use video consultation, value of non-verbal communication, patient satisfaction, provider satisfaction and user friendliness of the video connection technology were measured using questionnaires.
Results None of the included patients ever had a video consultation before with a healthcare provider. Nonetheless, 22/50 preferred a video consultation over a telephone consultation. Patients who preferred a video consultation underlined the benefits of providing visual feedback to both patients and healthcare providers. Moreover, healthcare providers felt they were better able to assess the patients’ healthcare condition.
Conclusion For patients who value both verbal and non-verbal interaction and feel comfortable with the use of video consultation, video consultation is the preferred contact modality. Shared decision making should be used to choose the preferred interaction modality. For patients with low digital skills, support might be needed or video consultation may not be the preferred choice.
- surgical oncology
- gastrointestinal diseases
- colorectal surgey
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
At the surgical outpatient clinic, patients with colorectal disease can be complaint free after surgery for prolonged periods of time. For this category of patients, physical examination and interventions are unlikely to occur during scheduled follow-up consultation.1 Moreover, there is no evidence specifically advocating the importance of face-to-face clinical examination.2 Hence, face-to-face consultations requiring travelling to the hospital may not be necessary if a satisfying alternative can be offered.3 4
Telephone consultations (TCs) with a healthcare provider is an alternative. TCs are frequently used to facilitate low key access to healthcare; including short follow-up calls in the outpatient setting.5 As such, TC permits avoiding unnecessary travelling, reducing patients’ expenditure.6 However, in some instances TC as a contact modality may be insufficient to patient or provider. For example, when valued information can only be derived trough visual interaction. This can range from information obtainable via visual feedback, such as relating to one’s facial emotions, to actual visual inspection of patients’ wounds, stoma or drains in situ.7
Video consultation (VC) offers the same advantages as TC in terms of reducing hospital related inconveniences, but does allow the use of non-verbal communication. High patient satisfaction with VC is reported in literature for patients receiving outpatient medical specialist care at home.8–10 To date, little is known as to the patient’s relative advantage of adding visual interaction when compared with TC. Although it may be believed that VC is in popular demand by patients, their willingness and ability to accept VC as contact modality over TC has not been investigated before in an academic setting. Neither has their satisfaction using VC in such a setting yet been evaluated.11
The aim of this study was to address patients’ perceptions towards the use of VC as a contact modality to allow visual feedback in patients at the outpatient colorectal clinic choosing voluntary for either VC or TC. The research questions were: (1) How many patients are willing to use VC? (2) What is their perception towards the added value of non-verbal communication of both groups (VC and TC)? (3) How satisfied are healthcare providers using VC as an alternative to TC? and (4) How is the user-friendliness of the VC connection rated by patients using VC?
Material and methods
Study design
This cross-sectional survey study regarding the implementation of VC at the surgical outpatient clinic was performed at a tertiary referral centre between October 2017 and June 2018. A total of 50 surgically treated patients with colorectal disease were included. Their written informed consent was obtained. Within VC implementation studies, it is common to not randomise participants to mimic standard clinical practice. As such, ‘shared decision making‘ was used to allocate patients to either the VC or TC group based on indicated preference (convenience group sample).
Participants
Patients aged 18 years or older with colorectal diseases having had surgery, scheduled for a TC in follow-up at the outpatient clinic were considered eligible. Reasons for consultation were: discussing overall progress, discussing a result, discussing a treatment or discussing a complaint. Exclusion criteria were: patients without access to Internet, patients without a smartphone, tablet or computer and patients who did not or were not willing to activate their electronic patient portal, as the VC contact was offered via the electronic patient portal of the hospital. All colorectal surgeons working at the outpatient clinic were included to evaluate their opinion on VC.
Study protocol
The study-coordinator approached eligible patients by telephone to inform them about the study. If patients were willing to participate, verbal informed consent was obtained and noted. After verbal informed content was obtained, participants were allocated to either the VC group or the TC group based on their expressed contact preference.
VC group
For all patients allocated to the VC group, a test consult with the study coordinator (EZB) was scheduled. During this test consult, additional logistic information was provided about the upcoming VC with the caregiver. The quality of the VC connection over Wi-Fi/4G was checked as well. When no connection could be established using videoconferencing, the study coordinator would reach out to the participant by telephone to try and coach the patient until it did work. When a reliable connection could be established and the participant wished to proceed with a video consult, a VC with their caregiver was planned, replacing the scheduled TC. After the VC, participants automatically received a questionnaire via the electronic patient portal.
Healthcare as usual
Patients who preferred the regular TC appointment above a VC were scheduled for TC with their caregiver, as per usual practice. No contact with the study coordinator was scheduled before this TC. The trial questionnaire was sent digitally after their consult using SurveyMonkey. This online survey tool was considered to be compliant with privacy legislation as the study was completed before the new General Data Protection Regulation (GDPR) legislation became effective.12
VC equipment
Software enabling secure VC connection (VIDYO (VIDYO, Hackensack, New Jersey, USA)) was integrated with EPIC Hyperspace 2017, which is the electronic hospital record (EHR) of use. For patients, the video connection was readily accessible via MyChart, which is part of the EPIC13 electronic patient portal, by using their own stand-alone desktop computer, laptop, tablet or smartphone.
The VC was scheduled in the caregivers EPIC portal following outpatient agenda workflow. To access and start the actual VC, surgeons started the real time video connection by clicking the ‘connect to video’ button, within the appointment scheduled in their own outpatient agenda using the EHR (figure 1). In this phase, it was not yet possible to record the VC, as our goal was to first establish a successful and safe implementation of real time VC’s. Because the video software was integrated within the EHR, confidentiality was ensured through standardised regulations of the hospital following the prior and current GDPR guidelines, with a protected personal two-factor verification login portal.

Video connection at the outpatient clinic (surgeon) and on a smartphone (patient). Permission of all pictured individuals was obtained.
Data collection
Patient characteristics
Demographic data such as age, gender and diagnosis were collected from the EHR.
Evaluating patients’ perception towards VC
A study-specific questionnaire was designed based on a review of literature and adjusted in consultation with medical specialists and an epidemiologist. The 21-item questionnaire consisted of two parts. The first section was related to personal questions regarding information on the personal use of Internet and video calls. The second section consisted of questions comprising patients’ perception and satisfaction regarding the treatment method and specifically the perception towards the use VC for their consultation. The answers were collected using a 5-point Likert response mode (totally disagree to totally agree). Open text field allowed patients to further elaborate on their choices. The questionnaire is available as online supplemental file 1.
Supplemental material
Evaluating provider satisfaction with VC
The participating surgeons completed a 9-item questionnaire at the conclusion of each consult to assess satisfaction, benefits or perceived benefits of the TC or VC and efficiency of the consult. Five items were assessed on a 5-point Likert-scale (range: ‘totally disagree’ to ‘totally agree’), four items were yes or no questions and one question was open ended.
Usability of the used VC technology
To assess the usability of VC, the validated System Usability Scale (SUS) was used.14 The SUS is an effective tool to measure usability, easy for study participants to use and provides a single score which is clear to understand. Based on a 10-item questionnaire, answered on a 5-point Likert scale, it provides a score from 0 (negative) to 100 (positive). The questionnaire contains alternating positive and negative items. A SUS score between 68 and 80.3 is considered as ‘good’ usability.
Statistical analysis
Data are presented by their means and SD when normally distributed, or by their median and IQR in case of a non-normal distribution. Categorical data are presented in frequencies and proportions, χ2 test was used to test the level of significance. To test whether there was a difference in baseline characteristics between both groups, the Mann-Whitney U test was performed as data was not distributed normally.
Statistical significance was considered when the calculated probability (p) was smaller or equal to an α of 5% (p≦ 0.05). IBM SPSS V.25 was used for statistical analyses (IBM).
Results
Patient characteristics
The baseline characteristics of both groups were comparable regarding age, gender and clinical diagnosis. None of the participants had any previous experience using VC in healthcare. Twenty-two out of fifty (44%) of patients indicated to prefer a VC over a TC to contact their healthcare professional. After the test consultation, all patients in the VC group wished to proceed with the VC. Patients who used VC for personal use felt significantly more comfortable in choosing VC over TC than patients who are not familiar with VC (p<0.001) The baseline characteristics are presented in table 1.
Baseline values and characteristics regarding the (personal) use of video calling of the study sample
Patient perceptions towards the use of VC
Patients’ responses to the questionnaire statements are shown in figure 2. The VC group that experienced the visual interaction expressed a highly positive attitude towards their perceived benefits of visual feedback.
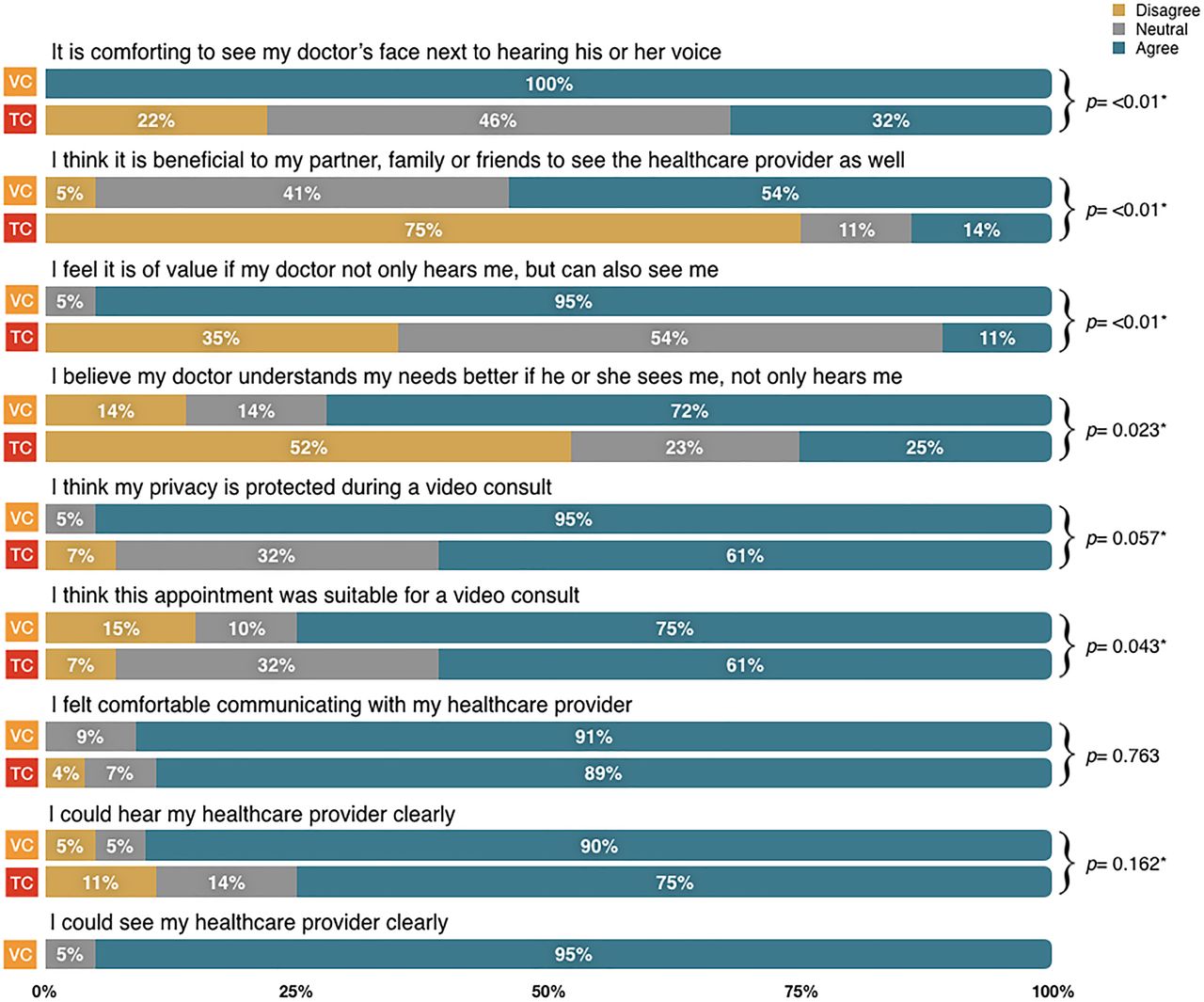
Results of the questionnaire completed by patients after a video consultation (VC) or telephone consultation (TC). Categories ‘totally agree’ and ‘agree’ were pooled as were ‘totally disagree’ and ‘disagree’. *p<0.05. χ2 test was used.
Patients in the VC group gave significantly higher scores than the TC group when asked if it would be; nice to receive visual feedback for the patient or family, if it is of value for the healthcare provider to see the patient, next to hearing their voice and whether the doctor is better able to meet their medical needs.
For both groups the communication with their healthcare professional was clear. Patients in the VC group felt just as comfortable communicating with their healthcare professional compared with communicating during a TC. Almost all patients in the VC group thought their appointment was suitable for a VC. Within the TC group, 17 out of 28 patients thought their appointment could be replaced by a VC. Both groups reported confidence in the protection of privacy during a VC.
Both groups were highly satisfied with their consultation 8.6 (SD=1.098) vs 8.5 (SD=0.882). Patients in the VC group indicated that they would like to use VC again in the future. In the TC group, 9 out of 28 patients would like to use a VC in the future and 11 patients might use a VC in the future. In retrospect, 5 (20%) patients would even replace the TC for a VC. None of the patients in both groups requested additional follow-up after their consultation requiring physical attendance at the hospital.
Reasons for choosing a VC were; seeing the healthcare provider, contact being more personal and trying out new technology. Reasons for choosing a TC were; hesitation to use technology, VC not offering added value or expecting a short telephone call without unforeseen news.
Healthcare providers satisfaction towards the use of video as consultation modality
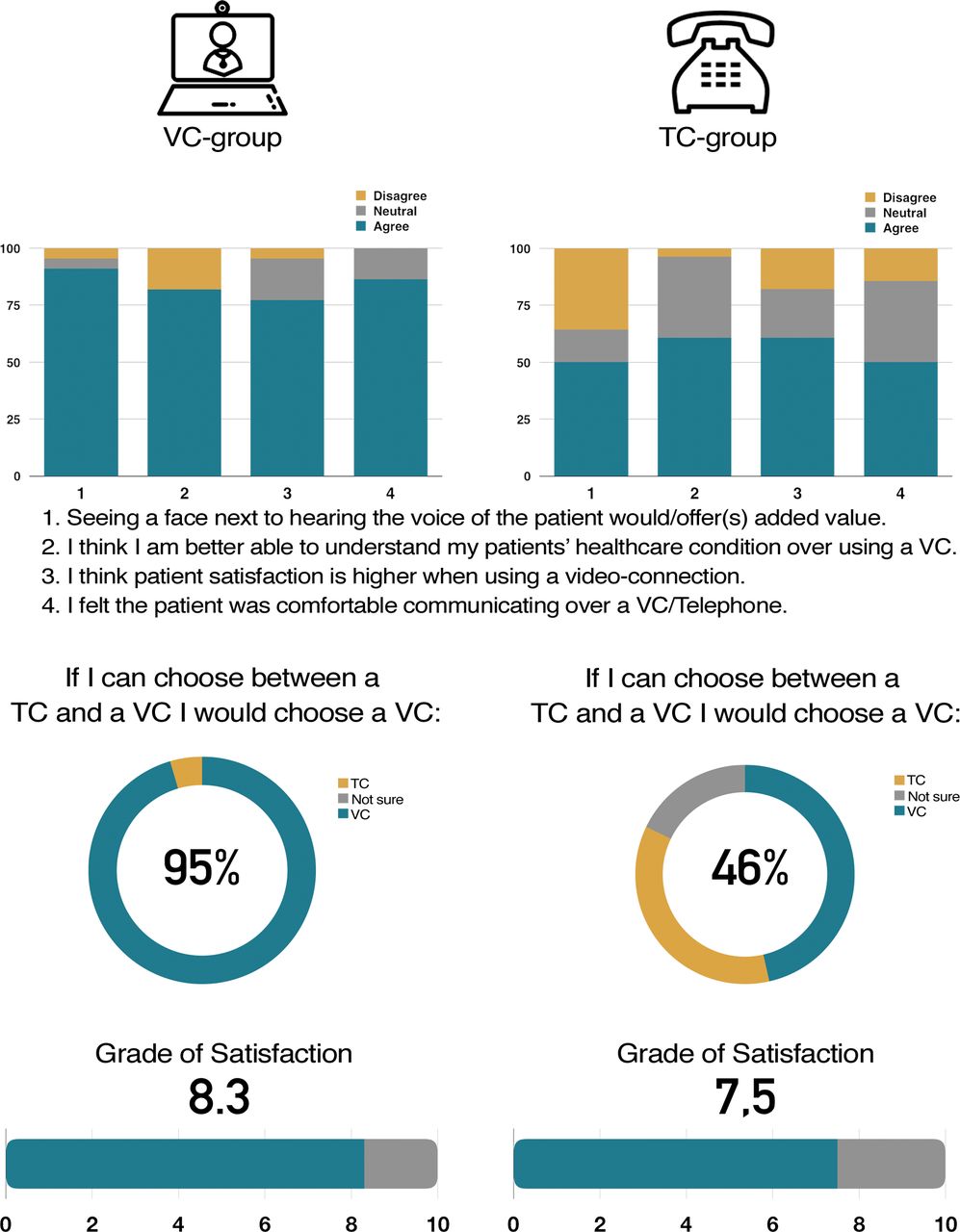
Within the TC group, surgeons thought the addition of visual feedback would have been beneficial in 14/28 of the consultations. Yet, for patients in the VC group, surgeons perceived the addition of visual feedback as beneficial in almost all patients (20/22) and felt they were better able to assess the condition of the patient. Surgeons felt a VC took none to a little extra time in comparison with a TC. Even then, in retrospect, in 21/22 from the VC group and in 12/28 patients from the TC group surgeons indicated they would choose a VC over a TC for this appointment.
Out of all patients, surgeons felt that for 33 out of 50, the use of a video-connection is more helpful in meeting the needs of their patients, resulting in a higher patient satisfaction. The overall grade of satisfaction with VC among surgeons was 8.3 (SD=0.842) in comparison with 7.5 (SD=0.576) for a TC. Surgeons’ responses to the questionnaire statements are shown in figure 3. None of the surgeons had previous experience with VC prior to this study.
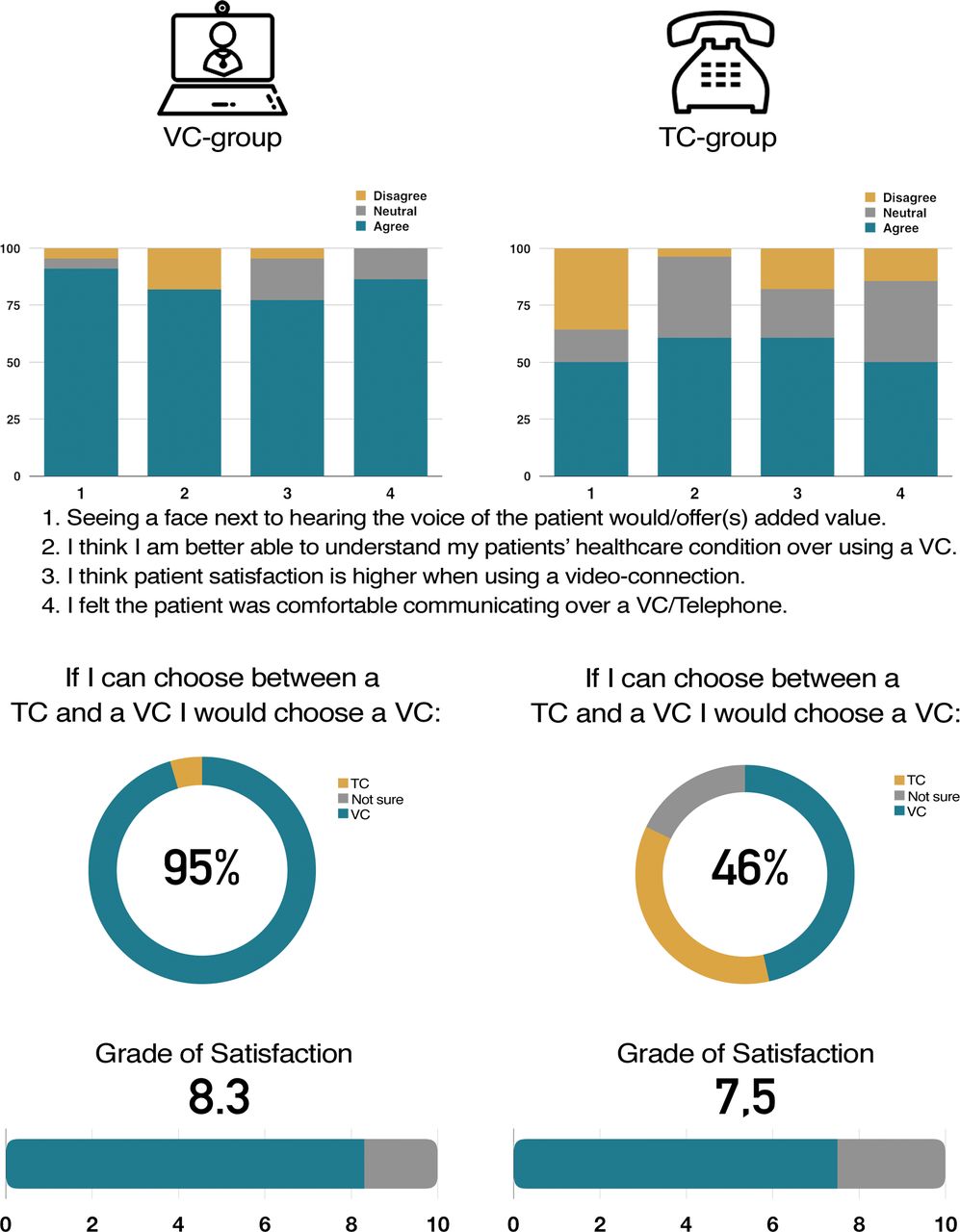
Results of the questionnaire completed by surgeons after a video consultation (VC) or telephone consultation (TC). Answers were provided on a 5-point Likert scale and are presented in percentages. Categories ‘totally agree’ and ‘agree’ were pooled as were ‘totally disagree’ and ‘disagree’.
Usability of the VC connection
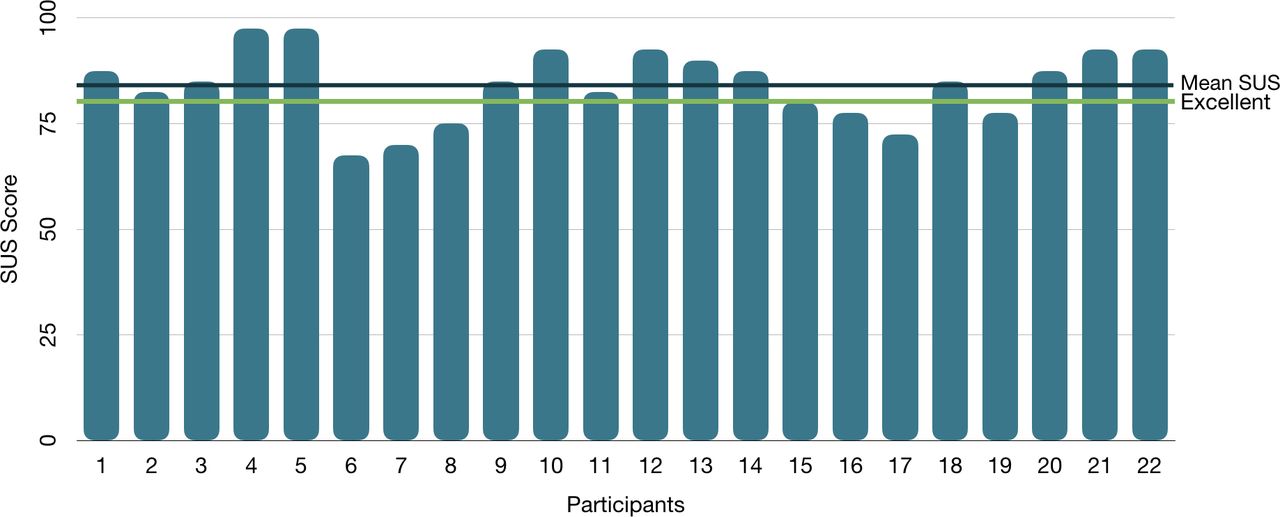
The overall mean score on the SUS was 84 (SD=8), which correlates with an excellent grade of usability. Out of all participants, 6 out of 22 (27.3%) rated the usability as good (SUS score 68–80.3) and 16 out of 22 (72.7%) rated the usability as excellent (SUS score >80.3). The SUS scores are presented in figure 4.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Results of the System Usability Scale (SUS) completed by patients in the video consultation (VC) group after the VC.
Discussion
The quality of care for patients in the outpatient setting has many dependencies. In current times, social distancing while preserving quality of interaction, is one of them. Personalised outpatient hospital care needs to respect patient’s wishes, limitations and clinical requirements. Setting up such access, while respecting these needs, is believed to be key in modern healthcare.15 Therefore, we explored the use of VC at the outpatient clinic based on patients’ preferences.
In line with other studies, almost half of the patients preferred to communicate with their surgeon over a video connection instead of over the telephone.16 17 Patients who received a VC were highly satisfied and underlined the beneficial aspect of visual feedback to both the surgeon and the patient. Most importantly, they felt the surgeon was better able to understand their medical condition because of visual cues.
Often TC is used as a means of informing patients about the results of diagnostic tests. Depending on the outcome of the results, visual cues for both patients and healthcare providers may be an important aspect of communication. This may affect the decision to use a VC or TC.18
In a National survey study among 987 Dutch patients, reasons to choose a VC over a TC were follow-up after hospital admission and after in-hospital treatment, discussing a treatment and discussing news with a negative outcome.16 The ability to use non-verbal communication and contact being more personal were considered important factors in their preference for VC. As expected, patients chose TC over VC in case of discussing good news. The absence of non-verbal communication was not considered a barrier in when there was good news to discuss, illustrating the effect of the degree of importance of visual cues.19
A limitation of this study is the study design. Patients were assigned to either the TC group or the VC group based on their own preference, mimicking standard clinical practice, but including the risk that our study population is not representative concerning the usability of our VC system for the population studied. Although, we did not find a statistical significant difference in the reported experience with technology between both groups, this could lead to higher usability results. In addition, this study did not include a formal comparison in complexity of consultations between both groups, and we did not assess return consultations concerning unresolved issues. However, our study was not about increasing the quality of detecting recurrent disease or improving surveillance. This study provided insights in patients’ willingness and satisfaction with VC to eliminate the disadvantage of the lack of visual feedback during a TC.
Since the outbreak of SARS CoV-2 and the associated disease COVID-19 in December 2019, new models of care like VC have gained significant attention.20 21 This, in order to preserve the provision of healthcare while avoiding face-to-face contact between clinician and patient.22 As a consequence, healthcare professionals are dependent on either TC or VC. Now, more than ever, providing patients the option of VC is important in order to continue the delivery of qualitative patient care.23–25 The results of this study can be used to aid healthcare providers, together with shared-decision making, to determine whether VC is a good alternative option, when face-to-face contact is not possible.
Future studies should focus on the specific impact of visual cues during VC on patient outcomes and how VC can be optimally implemented to maximise both patients and healthcare provider benefits. Especially, oncology patients may benefit, as their diagnosis comes with uncertain prospects and difficult decisions. Receiving complex medical information over the telephone might be undesirable but not uncommon. For patients, the non-verbal communication (eg, eye contact, smiling and body movement) of a healthcare provider is likely to improve a good surgeon–patient relationship.26 For healthcare providers, visual cues of patients are important to address patients’ worries or uncertainties which otherwise might have been missed.27
Conclusion
Surgical patients with colorectal disease are positive about VC. The use of non-verbal communication during a VC appears to offer important benefits over TC during follow-up care at the outpatient clinic. VC can be used when visual feedback is desirable, but might not be worth the effort in case of communicating a test result with good news. In times of social distancing, as with the current COVID-19 pandemic, healthcare providers are more dependent on visual cues advocating the use of VC.
Acknowledgments
The authors wish to thank the following persons for their contribution in the conduct of this study: N. Ignjatovic, E. Kok, R.M. Kunze, F. Meerman, C. Zwemmer-Fokker, the e-Health team and all those who have contributed to, and were part of, the implementation of video consultation.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @estherbarsom, @marliesschijven
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Obtained.
Ethics approval All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. This is an observational study. The medical ethics committee exempted this study from approval and a formal ethics approval was waived.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available on reasonable request.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.