Article Text

Abstract
Introduction Sustained high compliance with hand hygiene prior to patient contact in a neonatal intensive care unit (NICU) could reduce the spread of pathogens and incidence of bloodstream infections of preterm infants. These infections are associated with high mortality, morbidity and additional costs. Behaviour change interventions to promote hand hygiene, such as education, have only temporary beneficial effect on compliance. Our aim is to develop a technical intervention that supports a sustainable behaviour change for appropriate hand hygiene among NICU healthcare professionals.
Methods Students from different disciplines incrementally designed and evaluated solutions in co-creation with healthcare professionals of a NICU in a teaching hospital.
Results A prototype of the ‘Incubator Traffic Light’ system for neonatal incubators was developed, that is, a touchless alcohol-based hand rub (ABHR) dispenser with integrated colour display and incubator door sensor with lights. The system provides visual feedback to support healthcare professionals’ compliance with the prescribed 30 s drying time for ABHR. After 30 s, green lights indicate that the incubator doors may be opened. In the event that doors are opened without dispensing ABHR or earlier than 30 s, blinking orange lights and a display message urge the person to close the doors. The system documents compliance data in a web-based database.
Conclusions We developed a sophisticated technical intervention to support hand hygiene compliance. It is ready for clinical tests that should prove that the system contributes to sustainable hand hygiene compliance near neonatal incubators.
- neonatal intensive care unit
- hand hygiene compliance
- behaviour change intervention
- feedback system
- participatory design
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- neonatal intensive care unit
- hand hygiene compliance
- behaviour change intervention
- feedback system
- participatory design
Introduction
Worldwide, 10% of infants are prematurely born (<37 weeks of gestational age).1 The most vulnerable of these are admitted to a neonatal intensive care unit (NICU). Infants with a very low birth weight (<1500 g) carry a high risk of bloodstream infection due to the immature host defence; incidences ranging from 11% to 53% have been reported.2 3 These children are placed in an incubator to keep their body temperature stable and to allow for optimal observation.
Bloodstream infections in preterm infants are associated with severe complications, such as severe cerebral haemorrhage, loss of hearing, spasticity, necrotising enterocolitis, chronic lung diseases, retinopathy and poor (neuro)developmental outcomes; they can even lead to lifelong disability and death.2 4–7 Affected infants stay some 12 days longer than the average duration, which incurs additional costs.8 Furthermore, these infections need to be treated with antibiotics, thus raising the risk of antibacterial resistance.9
The WHO and the Centres for Disease Prevention and Control recommend correct hand hygiene as the best method to reduce the horizontal (patient to patient) spread of pathogens by healthcare professionals.10 Hand hygiene is a major element of many bundles of measures to prevent (bloodstream) infections.2 11 12 Correct hand disinfection is achieved by rubbing the hands with a liberal amount of alcohol-based hand rub (ABHR) and let them dry for at least 30 s to kill off micro-organisms.
This procedure is in accordance with the European guideline EN 150013 and the manufacturer user-instructions of the ABHR used at the NICU of this study (Manusept basic, Bode Chemie GmbH, Hamburg, Germany). Besides rubbing time other factors are relevant like the amount of applied ABHR and the rubbing technique (the way the ABHR is distributed over the hands and fingers).
Regrettably, hospital staff compliance with hand hygiene protocols is generally low. Studies found that only 20%–45% of staff disinfected their hands adequately by protocol; others simply forgot or felt work pressure.3 14–16
A variety of non-technical and technical (electronic) systems have been developed to monitor hand hygiene compliance, some of which also aim to improve compliance by behaviour change.17 18 The use of advanced electronic systems that provide real-time individual feedback about hand hygiene compliance resulted in a short-term beneficial effect on compliance.18 None of the existent systems monitors compliance with the required (30 s) drying time and is dedicated to hand hygiene practices near a neonatal incubator.19–21
Long-lasting high compliance with hand hygiene could perhaps be achieved with a closed-loop feedback system20 22 that provides visual feedback prompts when someone uses the ABHR dispenser and opens the incubator doors. We aimed to design an incubator hand hygiene feedback system that reminds users to wet and rub hands with ABHR and apply at least 30 s drying time, and also documents compliance and non-compliance in a web-based database.
Materials and methods
The feedback system was co-designed in an educational setting by researchers and students of the Rotterdam University of Applied Sciences together with nurses, medical doctors, Newborn Individualised Developmental Care and Assessment Programme (NIDCAP)23 certified specialists, housekeeping staff, infection prevention specialists and medical device safety specialists of the NICU of the Erasmus MC-Sophia Children’s Hospital, in incremental design-research projects between 2011 and 2016. A participatory design approach served as co-creation method.24
Around 20 NICU healthcare professionals participated in ‘co-creation sessions’. A co-creation session included two to five NICU healthcare professionals and one to three students, and served to demonstrate and discuss design proposals, mock-ups and prototypes; for example, simulating feedback scenarios (the sensory and cognitive ergonomic aspects of visual feedback that would optimise hand hygiene compliance) with sketches attached to a real incubator and computer visualisations (figure 1). The co-creation sessions lasted 30 min and resembled an informal, unstructured, interactive group interview. Alternative design proposals could be assessed, after which discussions between NICU healthcare professionals, students and teacher-researchers led to design decisions. Mostly, two consecutive co-creation sessions took place for one specific design decision, and in most cases, this led to a congruous opinion. All sessions were documented by taking notes, photos and or videos.

Visualisation of a feedback-scenario (increment 3, 2014).
Inclusion to the co-creation sessions was limited to NICU nurses and housekeeping staff, all being NICU staff at the Erasmus MC-Sophia Children’s Hospital in Rotterdam. No parents of preterm infants were involved because they do not (need to) disinfect their hands with ABHR. In addition to the co-creation sessions, we conducted semistructured interviews with NIDCAP-certified specialists.
In total, 32 third-year and fourth-year students of different bachelor degree educational programmes (Physician Assistant, Occupational Therapy, Industrial Design Engineering, Healthcare Technology, Electrical Engineering, Technical Software Engineering) did the design research, usually in teamwork, in increments with constant participation of the NICU staff. Table 1 describes the five increments in the development of an incubator hand hygiene feedback system, which we named the Incubator Traffic Light. In the first co-creation sessions (increment 2, 2013), ethical aspects (eg, feelings regarding privacy and integrity) were discussed. It appeared that most NICU healthcare professionals would support a feedback system as long as no data directly related to patients or NICU healthcare professionals would be logged. From the first interviews with professionals, it appeared that they would like to have some form of visual feedback for the prescribed 30 s drying time near the incubator doors. This was provided for by incorporating coloured light-emitting diodes (LEDs). In addition, the hand alcohol dispenser needed to be placed as close as possible to the incubator doors. The manually lever operated ABHR dispenser that was in use at the time could not be placed directly on the incubator, however, as the noise and vibrations could disturb the baby. The later introduced touchless operated dispenser that was noiseless, and healthcare professionals saw no problem in placing this dispenser directly on the incubator.
Increments in the design research process
Results
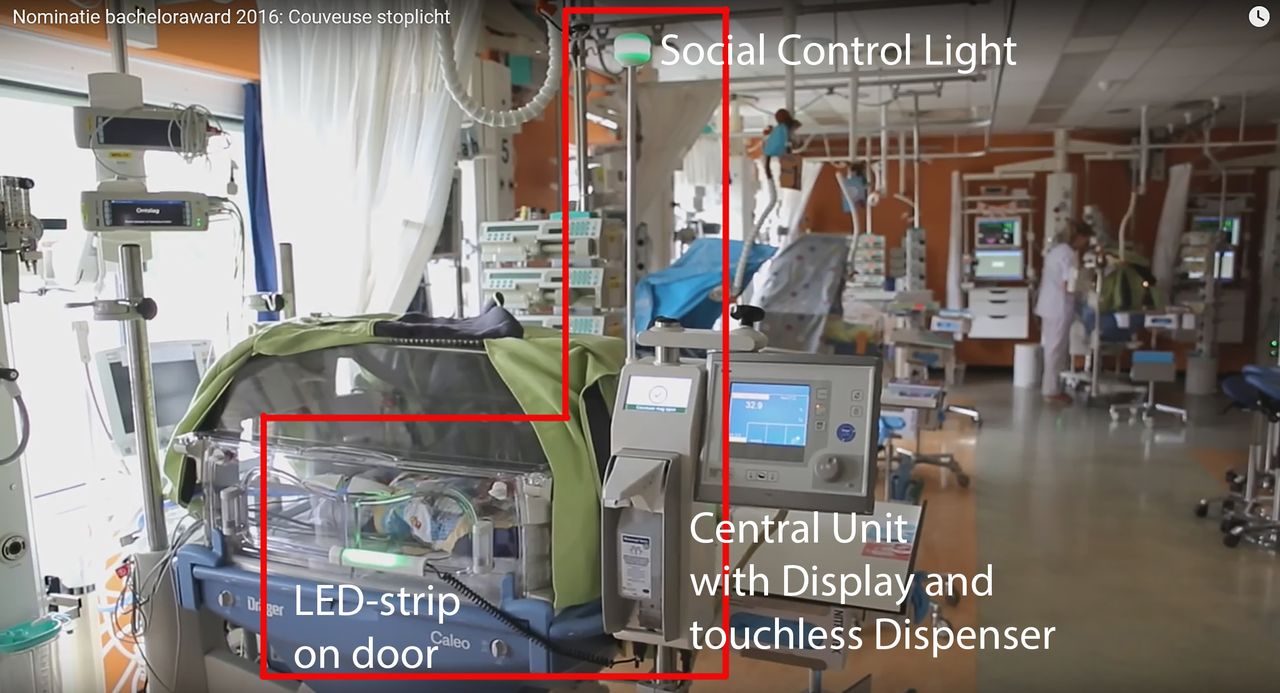
The final prototype of the Incubator Traffic Light provides visual feedback by a display situated above a touchless ABHR dispenser, a LED strip situated on one of the doors and a social control light situated on an aerial above the display (figure 2).

Final prototype of the incubator traffic light, located on the neonatal intensive care unit, https://youtu.be/NsNfHdSaTLo (increment 5, 2016). LED, light-emitting diode.
Feedback on hand hygiene compliance is provided via four modes: (1) stand-by; (2) hand rubbing; (3) protocol correct and (4) protocol incorrect (figure 3). The stand-by mode serves as the ‘red traffic light’ (although with amber colour, to avoid unnecessary red light). ‘Hand rubbing’ starts by placing a hand under the dispenser’s tap point to activate the touchless dispenser. In the hand rubbing mode, the blue light on the LED strip and the blue social control light indicate that the hand rubbing is going on. In addition, the display shows a video with hand rubbing instructions (showing a good execution of hand rubbing with ABHR) and a graphic 30 s countdown timer. After 30 s, the next mode displayed is either the ‘protocol correct’ (‘green light’) or the ‘protocol incorrect’ (‘orange blinking light’); the latter is the case if the door is opened before 30 s have elapsed, or alcohol has not been dispensed.

Visual feedback per modus and elements of the incubator traffic light. LED, light-emitting diode.
Hardware
The system’s hardware consists of a main unit of two plastic housing parts (3D printed ABS) that contain a touchless hand alcohol dispenser (Ophardt, Issum, Germany, type: Ingo-man plus Touchless), a 4.3-inch colour display (Graphic LCD TFT RGB display 480×272 pixels, 4D systems, Minchinbury, Australia, type: uLCD-43D) and a central processing module (Atmel, San Jose, USA, type: ARM processor 32-bit ATSAM4SD32CA-AU) that runs on custom developed software and is powered by a custom designed power module (figure 4).

Interconnect diagram of the electronics of the incubator traffic light (increment 5, 2016).
The front plastic housing part integrates and connects all modules and can be mounted to the 38 mm steel tube of the incubator (Dräger, Lübeck, Germany, Type: Caleo). The backside housing part is mounted to the front part as a protective and aesthetic cover. Via an Euronorm C13-net connector the system is connected to one of the internal 230V Euronorm C-13 net output of the incubator, and is thereby independent from an external 230V net connection. To comply with the electro-technical requirements for devices used in a clinical setting, the metal housing of the dispenser and the aluminium aerial rod, that holds the social control light, are electrical grounded. The aerial rod that sticks out from the main unit contains the social control light at its end (approximately 1.8 m from the ground). This control light consists of a round array of RGB (red blue green) LEDs in a 3D printed plastic housing. The LED strip that is click-mounted to the ridge of the door contains a printed circuit board with an array of 10 RGB Surface Mounted Device LEDs plus a reed switch (electrical switch operated by a magnetic field) that is activated by a magnet on the opposite door functioning as a door sensor.
Software
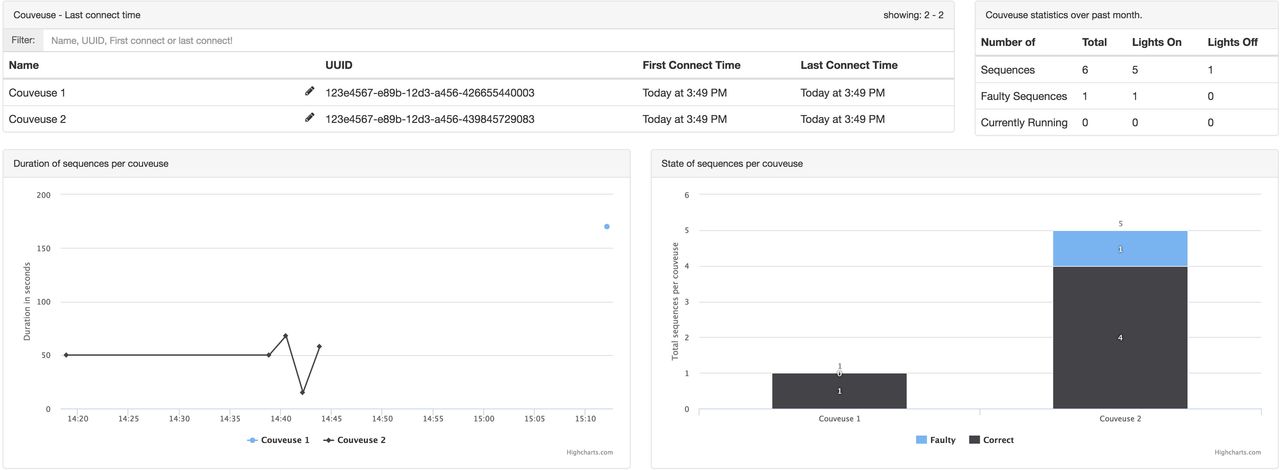
The database server software is installed on a cloud server and collects the compliance and non-compliance data per incubator via Wi-Fi. The data are visually represented on a computer dashboard (figure 5). The current design of the dashboard displays (a) the ‘last connect time’; (b) the incubator ‘statistics over last month’: the total number of sequences (A sequence is understood to be an logged data record: the time between dispensing alcohol and opening the doors); (c) the ‘duration of sequences’ in a time graph and (d) the ‘state of sequences’ in a block diagram, representing the correct and faulty sequences.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Dashboard visualising the data of compliance or non-compliance per incubator (increment 5, 2016).
The data records consist only of time statistics and no patient or clinicians details.
The hardware and software can be configured in two configurations with the use of a jumper switch on the central processing module: ‘lights on’ or ‘lights off’. These two configurations are necessary for our future effect study in which we will compare hand hygiene compliance in one NICU room with 10 fully functional Incubator Traffic Light systems (‘lights on’) with that in another room with 10 systems without visual feedback (‘lights off’).
Discussion
The aim of this project was to design a hand hygiene feedback system for neonatal incubators that provide visual feedback in line with the hand hygiene protocol: 30 s hand rubbing with ABHR before touching the baby in the incubator. The system also had to collect compliance data. The result is a fully functional prototype, the Incubator Traffic Light system, which fits on the Dräger Caleo incubator.
As mentioned in the Introduction section, we applied the European EN 1500 guideline as well as the ABHR manufacturer’s guideline that prescribes 30 s rubbing and dry time. Other guidelines such as the WHO guideline for hand hygiene in healthcare25 do not recommend a specific rubbing time (‘rub until hands are dry’). A study comparing the effectiveness of ABHR for different rubbing times concluded that the effectiveness with a 30 s rubbing time is not significantly better that that with a 15 s rubbing time.26 In case future studies prove that ABHR time could be reduced, the Incubator Traffic Light system can be easily adapted.
A hand hygiene education programme and sequential promotion initiatives have served as behaviour change interventions to improve hand hygiene compliance in a NICU setting.3 27–29 The education programme was associated with positive effects on hand hygiene compliance, although a ‘wash out’ effect was observed during 6-month follow-up.3 An intervention in which screensavers were displayed with visual reminders had a positive effect on hand hygiene compliance; it is unknown, however, whether the effect is sustained on the long term.28 An interrupted time study over 10 years concluded that the positive effect of sequential hand hygiene promotion interventions (education programme, gain-framed screen saver messages and an infection prevention week with an introduction on consistent glove use) on the infection incidence at a NICU ‘might be sustainable’.30
We could not find information on technical interventions like ours aimed at behaviour change regarding hand hygiene compliance in the NICU setting in the literature, patent databases or non-scientific databases. In previous hand hygiene compliance studies that used closed-loop visual feedback,20–22 the feedback loop also starts at the moment the ABHR is dispensed from a alcohol dispenser, gives feedback before patient contact and sends compliance data to a centralised database. Our system, however, was designed in the context of contact with a baby in an incubator, with the feedback focused on compliance with the required (30 s) rubbing time. Other systems only give feedback about whether or not ABHR is dispensed (dispenser activation) and or skin contact with alcohol is achieved (alcohol sensor) before a patient is approached. Furthermore, other systems require some form of (personal) identification to start the feedback loop (eg, a badge or sensor carried on the person) and feedback is directly linked to or visual on that person.22 31 Our system is anonymous and starts when the dispenser is activated. Personal data are not recorded; anonymity was a strict requirement that emerged during the participatory design sessions.
Strengths
Letting the end-users serve as co-designers helps accelerate the design process because early design mistakes are avoided and acceptance of a new intervention can grow. In this way, we could develop a prototype that was approved by all stakeholders and is ready for clinical safety testing.
Our Incubator Traffic Light not only serves as a hand hygiene reminder, but also stimulates compliance to the recommended rubbing and dry time and, by showing video instructions, good rubbing execution.
The system was developed to be used with a neonatal incubator, but it can also function as a stand-alone hand hygiene feedback unit (without the door sensor and slightly altered feedback settings) everywhere in a hospital.
Limitations
Achieving sustainable change in behaviour and acceptance of such a system is a delicate matter. In the co-creation sessions, opinions differed about the ‘usefulness’ of such intervention. It appeared necessary to constantly re-evaluate design decisions. Not all design decisions can be backed with logged evidence because not all discussions with NICU healthcare professionals were recorded in writing. For example, faulty conclusions were drawn with regard to the ergonomic placement of the main unit and display on the incubator because the sessions had not been conducted in the actual NICU setting. In a co-creation session in the incubator storage room, it became evident that the main unit and display needed to be placed on the left side of the incubator (seen from the ‘working side’ of the incubator, with the head of the baby to the left). After re-evaluation with prototypes in the real NICU situation, however, it became clear that the right side was far more logical from a usability point of view considering space and workflow.
Future studies
The data server software, specifically the design of the dashboard’s graphic user interface (figure 5), is not yet optimally user-friendly and has to be re-designed in co-design with direct end-users.
An observational study with a control group is planned to validate the effect of our system on compliance with hand hygiene as primary outcome and the incidence of infants’ bloodstream infections as a secondary outcome. To this aim, three identical NICU units with each 10 incubator-bed places will be randomly divided into a unit with 10 active Incubator Traffic Light systems (intervention unit, ‘lights on’), a unit with 10 non-active systems (non-intervention unit, ‘lights off’, but with compliance registration) and a unit with no systems (control-unit, compliance registration by visual observation). The study consists of three phases: pre-assessment, intervention and follow-up.
Conclusion
We developed a sophisticated technical intervention to support appropriate hand hygiene at NICUs. The planned observational study should prove that the ‘Incubator Traffic Light’ system contributes to sustainable improvement of hand hygiene compliance near neonatal incubators.
Acknowledgments
We thank all NICU healthcare professionals of Erasmus University Medical Center-Sophia Children’s Hospital and all the students and their guiding teachers of the Rotterdam University of Applied Sciences who contributed to the development of the Incubator Traffic Light. We also thank Ko Hagoort for text editing.
References
Footnotes
Contributors RHJvG and OKH were involved in the planning and execution of the study and writing the associated manuscript, including revision. LSGLW was involved in writing and revising the manuscript. All authors read and approved the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request.