Article Text

Abstract
Background The biodesign process, which originated at Stanford University, has had a significant impact on medical device invention. Design thinking skills are core elements in the biodesign process, but there has been no quantitative evaluation of how design thinking is actually affected by a biodesign course. The purpose of this study was to examine the usefulness of the biodesign process by quantifying design thinking ability.
Methods We recruited 17 participants who had studied a systematic biodesign process in Japan and 20 participants who were unfamiliar with the biodesign process. All participants took the design thinking test and we evaluated their design thinking skills using a combination of the creation score and the evaluation score.
Results The average age of the participants was 34.4 years and 84% were male. Participants who had taken the biodesign program generated more ideas than other participants (5.3±1.9 ideas vs 3.7±2.3 ideas; p=0.01). They also had significantly higher design thinking score, especially creation score, than those who had not taken the program (design thinking score, 220.1±39.7 vs 194.6±32.1; p=0.02; creation score, 91.3±23.0 vs 70.7±20.2; p=0.03).
Conclusion The findings suggest that the biodesign process can cultivate design thinking skills, especially the ability to visualise needs and create solutions. Exposure of more people to the biodesign process may accelerate innovation in the medical technology field.
- biomedical engineering
- delivery of health care
- methods
Data availability statement
Data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Biodesign is recognised as an innovative human resource development program in the area of med-tech.
WHAT THIS STUDY ADDS
People who had taken part in a biodesign program in Japan showed stronger design thinking skills than those had not taken part in the program.
The effect seemed to be particularly strong for participants’ ability to identify needs and generate solutions.
The effect was less strong for participants’ ability to evaluate possible needs and solutions.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Exposing more people to the biodesign process and principles might accelerate innovation in medical technology.
Introduction
Innovation in medical technology (MedTech), which results in radical changes to existing concepts in the healthcare field, requires various elements and there are several barriers to getting innovative products to patients. The biodesign process, which originated at Stanford University, has made a significant impact in medical device invention and has saved many patients.1–4 One distinctive element of the Stanford biodesign process is the application of design thinking to create more sophisticated ideas. It allows innovators to identify core needs through an intensive focus on particular problems of the medical field. They can then create brilliant ideas to address these needs through a brainstorming process within the team. In these phases (called Identify and Invent phase in biodesign process), using this design thinking technique frequently makes the remaining needs and ideas more and more attractive.
The Stanford biodesign process has been established as a new form of medical device development methodology, and has already become popular in several regions, including India, Singapore, Ireland, Australia, Israel, Taiwan and China. The characteristics of this method differ slightly depending on the background and medical system in the region, but the process of innovating is basically the same. Innovative ideas that incorporate design thinking have led to innovative medical devices in all these countries.
In Japan, a biodesign program was launched in 2015 and the process has gradually permeated. Several MedTech start-ups have been created and are achieving results. The record of the biodesign program to date suggests that design thinking is an important factor in medical device development. However, there has been no quantitative evaluation of how the biodesign process affects design thinking. The purpose of this study was to examine the usefulness of the biodesign process by quantifying its effect on design thinking ability in Japan.
What is the biodesign process?
The biodesign process is a comprehensive approach, consisting of discovery of unmet clinical needs, creation of concepts and implementation (called the ‘3Is’, for Identify, Invent and Implement phases).1 2 The most important factor in this process is focusing on unmet needs and providing solutions to those needs. The golden rule of the biodesign process is that innovation should start with the needs of patients, physicians and other important stakeholders—not the technology. Innovation can be more reliably achieved by examining the needs and concepts from a business perspective at an early stage. This approach is called needs-driven and is a different process from technology-push innovation, the more traditional approach in MedTech innovation.
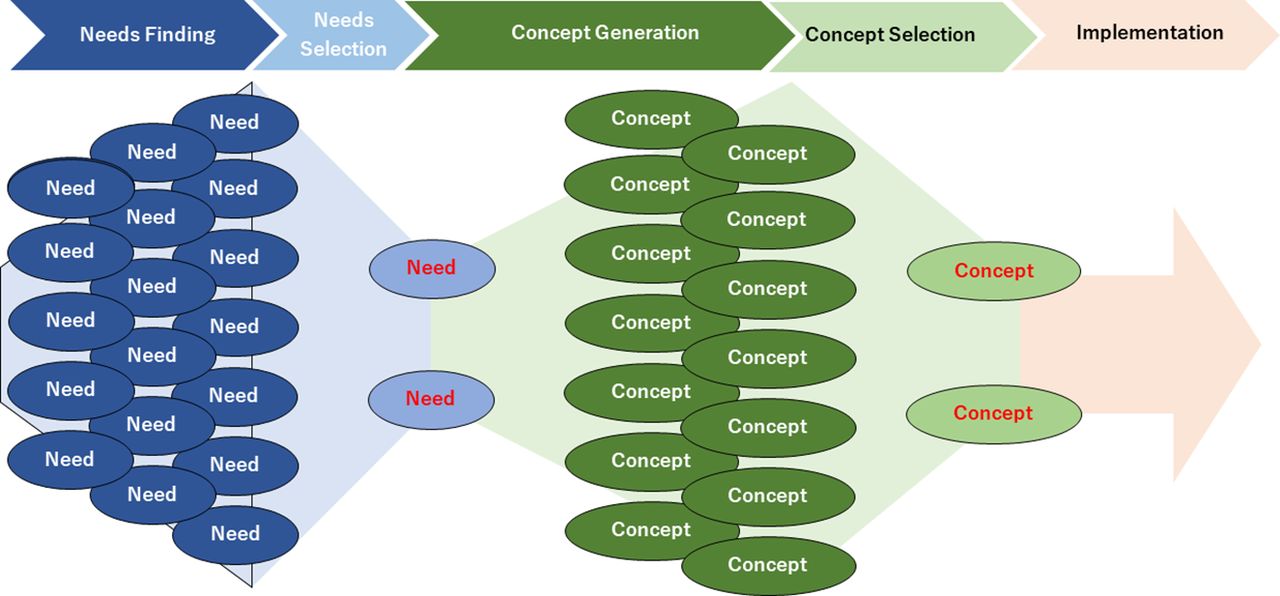
In the Identify phase, innovators search for unsolved problems in healthcare by observing the healthcare field thoroughly. These problems should be stated in a single sentence called the need statement. This is described as ‘a way to address (problem) in (population) in order to (outcome)’. The need statement is the core for future brainstorming and development. It is therefore important to research the disease mechanism, existing solutions, stakeholders and market to create a better need statement. Once a promising clinical need is found, innovators move into the Invent phase. Clinical, engineering and business members of the team engage in creative brainstorming to generate a number of possible concepts. These concepts are then sorted based on technical feasibility, intellectual property, regulatory issues, reimbursement and business models, as well as whether they meet the need criteria in the need statement. In the implementation phase, the team members consider the technical feasibility, the clinical development plan and the viability of the intellectual property, business model and future funding strategies in more detail, to create a strategy to get the innovation to patients. By conducting these three phases in a single process, inventors can move forward with innovative medical devices faster and with less risk (figure 1). Many inventors from the Stanford biodesign fellowship program have generated innovative products.3 4
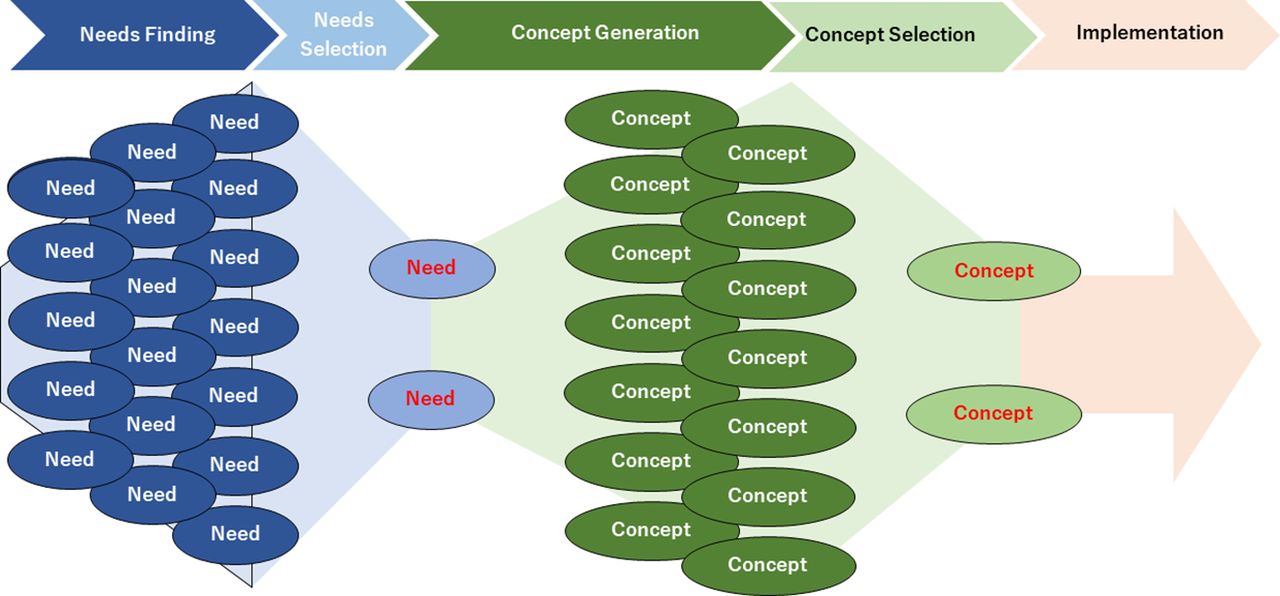
Biodesign process. The biodesign process consists of three phases: Identify (needs finding and needs selection), Invent (concept generation and concept selection) and Implementation.
Methods
Study population
The participants in this study were alumni from the biodesign fellowship program in Japan, which started in 2015, or who joined the global biodesign program at Stanford University. The biodesign fellowship program in Japan is a 10-month program and the context is almost the same as the Stanford fellowship program. This fellowship program was covered in three universities (Osaka, Tohoku and Tokyo), and we enrolled the participants from among the alumni or practitioners from Tokyo Biodesign. We also selected 20 people who were unfamiliar with the biodesign process to provide a comparison. All members took the design thinking test during 2 weeks in May 2021.
Patient and public involvement
There was no involvement of patients or the public in developing or carrying out this study.
Design thinking test
The design thinking test provides a way to score design thinking skills, which have been difficult to quantify until now. This test was composed of two parts: the ability to identify needs and propose solutions which was reflected as ‘the creation score’ and the ability to evaluate the importance of the needs and solutions which was reflected as ‘the evaluation score’. All participants are given a single point in time to identify an unmet need—problem finding—in various situations and to develop possible solutions—solution making—to it. The created solution ideas are peer-reviewed among the participants in blinded condition, and the quality of each person’s ability to find unmet needs and generate ideas for solutions are scored using a patented technology by VISITS Technologies. A needs evaluation score and a solution evaluation score are also calculated in the process. The total of the need finding and solution creation skills is defined as the creation score. The total for the needs evaluation and solution evaluation skills is the evaluation score, and the total of the creation and the evaluation scores is the design thinking score. This test can quantitatively measure the participants’ creativity and is widely used as an index to evaluate the design thinking ability of examinees in various companies and research facilities5 (figure 2).

Outline of design thinking test. The design thinking test consists of the creation score (needs finding and solution creation skills) and the evaluation score (needs evaluation and solution evaluation skills).
Statistical analysis
Categorical variables are shown as numbers and percentages, and continuous variables as mean±SD. Categorical variables were compared using the χ2 test, and continuous variables using Student’s t-test. A p value of <0.05 was considered to indicate a statistically significant difference. All statistical analyses used IBM SPSS Statistics V.28.0.
Results
Baseline characteristics
In total, 37 participants took the design thinking test (17 who had taken the biodesign program and 20 who had not). The baseline characteristics of the study participants are shown in table 1. The average age of the participants was 34.4 years and 84% were male. Age and gender were not significantly different across the two groups. There was no statistical difference in terms of occupation, although the percentage of medical providers was slightly higher in the non-biodesign group.
Baseline characteristics
Career after biodesign engagement
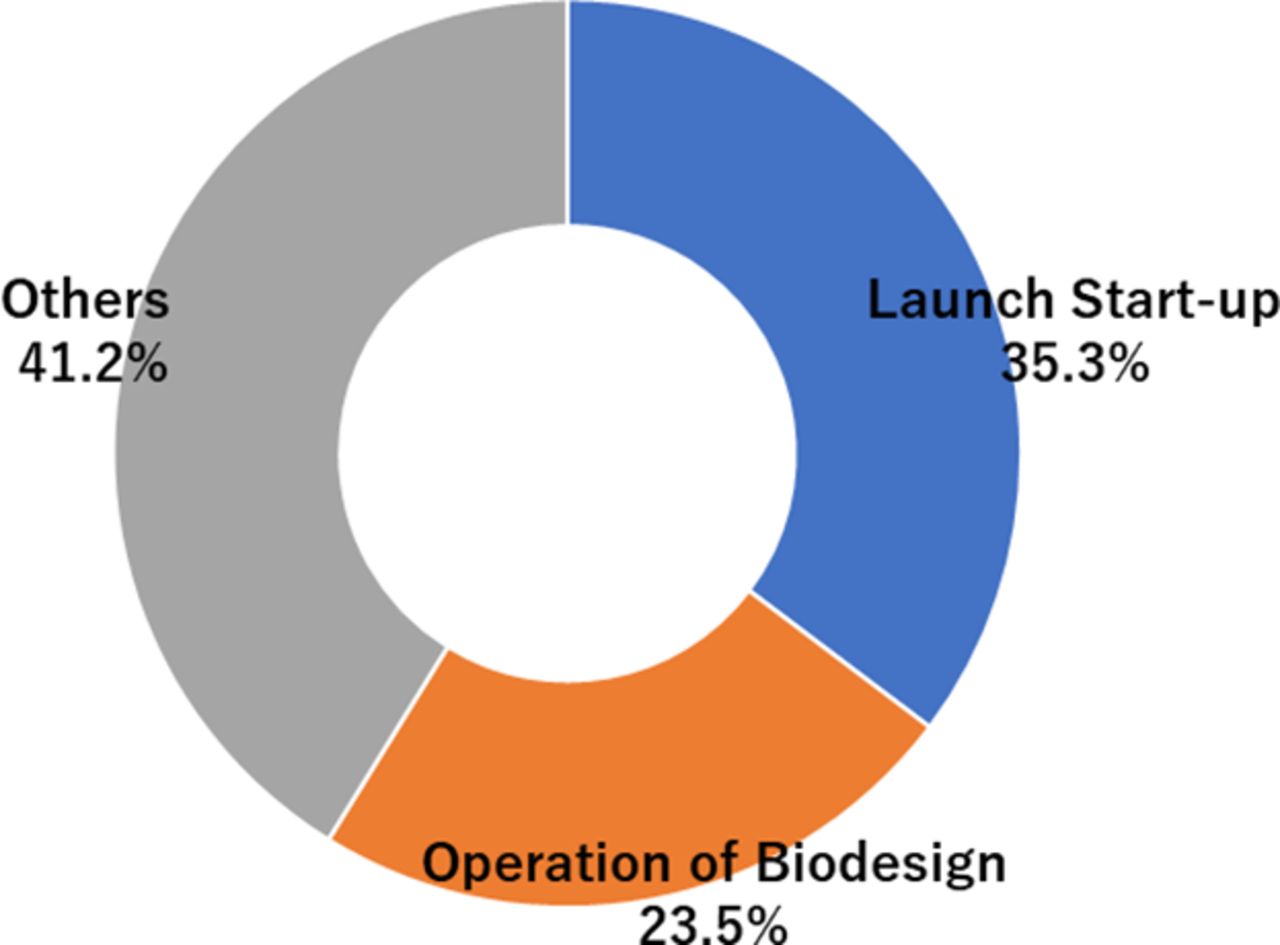
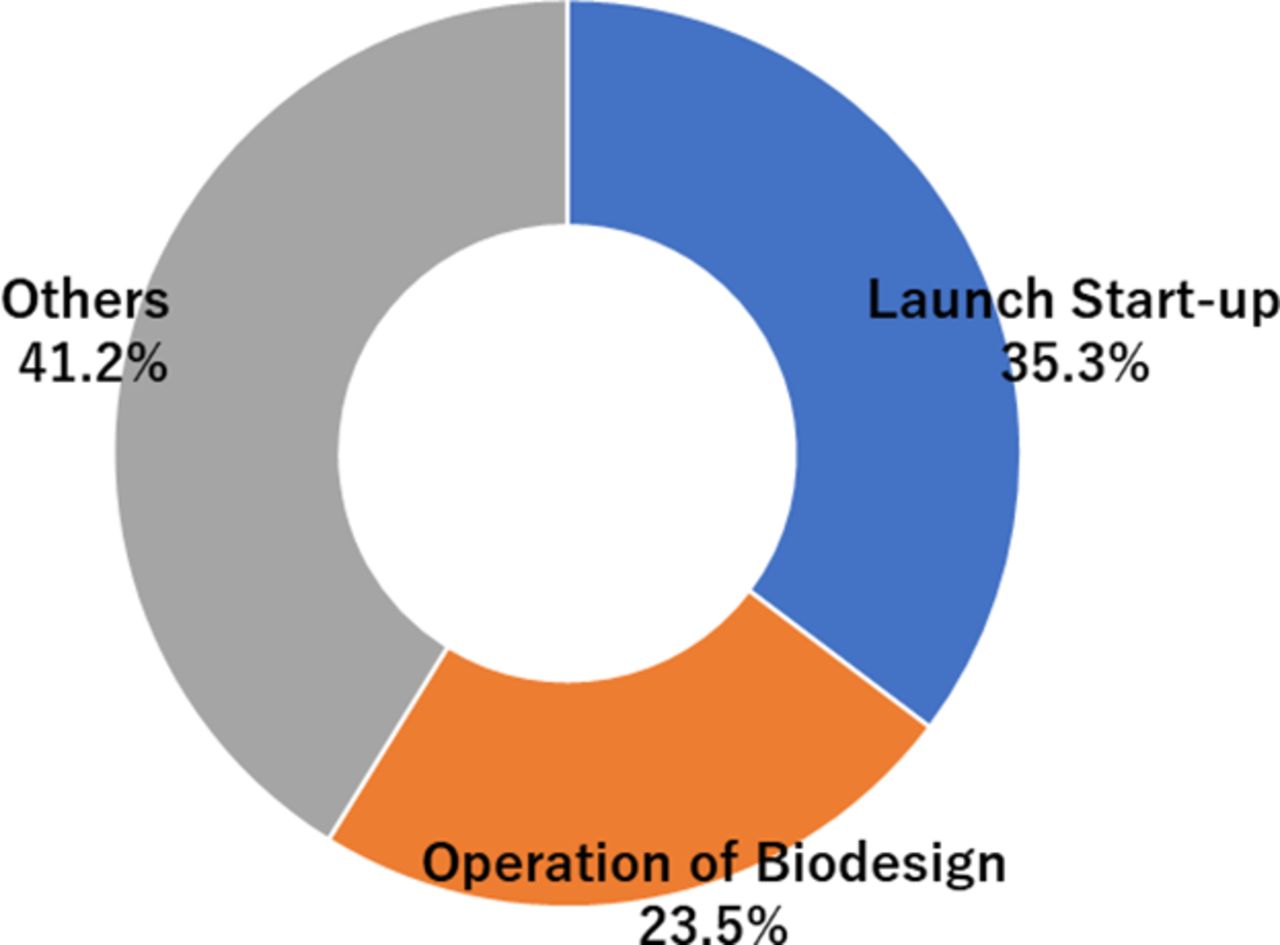
Figure 3 shows the career of each participant involved in Tokyo Biodesign after their engagement in this program. More than half of the participants were associated with start-ups originating from the biodesign program or Tokyo Biodesign more generally.
{kind=link}
{kind=link}
{kind=link}
Career after biodesign engagement. About two-thirds of the participants who took the biodesign program are now working in the MedTech field, including start-ups and operation of biodesign processes.
Design thinking test results
Table 2 shows the summary of the design thinking test. Participants who had taken the biodesign program created more ideas than those who had not taken the program (5.3±1.9 ideas vs 3.7±2.3 ideas; p=0.01). The design thinking score in participants who had taken the biodesign program was also significantly higher (220.1±39.7 vs 194.6±32.1; p=0.02), and particularly the creation score, the sum of needs identification and solution creation skills (91.3±23.0 vs 70.7±20.2; p=0.03).
Summary of design thinking test
Discussion
The purpose of this study was to elucidate the usefulness of the biodesign process by quantitative evaluation using the design thinking test. The results showed that people who were familiar with the biodesign process were 1.5 times more likely to generate ideas and 1.3 times more likely to be creative than those who had not taken a biodesign program. This suggests that the biodesign process can foster creativity and overall design thinking ability.
The biodesign process is a MedTech innovation method that started in 2001 at Stanford University. Previously, it was thought that being discovery-driven was important for innovation in healthcare field, which is still the case in the pharmaceutical industry. However, more recently, a needs-driven approach has come to be considered important especially for medical devices and diagnostic equipment. The needs-based approach in medicine is inspired by the concept of so-called design thinking, which is a process of emphasising, defining, ideating, prototyping and testing to find essential needs that are unknown to users. It is already being used in various non-medical fields. Consumers in medical care are quite complex, and it is difficult to understand their essential needs. Most inventors and innovators are not medical consumers and there are various stakeholders involved, including medical providers, patients and family. It is therefore essential to have a deeper and more focused empathy to understand real needs. The biodesign program at Stanford University emphasises the importance of having a cross-disciplinary team (medical providers, engineers and business experts) diving deeply into the field and understanding needs regardless of their own backgrounds. This needs-driven approach has led to innovations in several medical fields.6–10
In this study, we conducted the first quantitative evaluation of design thinking skills using a design thinking test. The test used in this study was divided into two main parts: (ⅰ) the ability to identify needs and propose solutions and (ⅱ) the ability to evaluate the importance of the needs and solutions. We found that the overall scores of the participants who had taken the biodesign program were higher than those who had not taken the program, especially the ability to propose needs and solutions. The biodesign fellowship program in Japan is a 10-month program. Approximately half of the period is spent focusing on identifying needs and the other half on creating solutions. It is therefore understandable that the participants from the biodesign program had a high ability to identify needs and solutions. The biodesign participants were also slightly better able to evaluate the needs and solutions, but this difference was not statistically significant. This evaluation ability can be thought of as discernment about promising needs and solutions. This ability can be nurtured by personal project success and gaining experience through exposure to various medical devices in the market. This result may suggest that continuing to be involved in medical device development using the biodesign process, and gaining experience after taking a biodesign program, will lead to better development of evaluation skills.
This study had several limitations. First, it had a fairly small sample size and the participants who took the biodesign program might have already had more creativity than others. The results need to be validated with a larger sample in the future. Moreover, the participants are from the Tokyo Biodesign program only and not from other facilities of biodesign in Japan. However, the fellows from each university received the same program and their quality is assured by Japan and Stanford University, which should generalise the result of this study to the whole of Japan. Second, the biodesign group in this study included fresh fellows who have just completed the biodesign training, as well as those who have worked in other areas for a while since completing the biodesign training. Therefore, there may be differences in proficiency in biodesign thinking. However, all of the participants apply the biodesign-based design thinking skills at their next positions and their design thinking skills should be maintained. Third, the design thinking test we used has not yet been validated academically. However, it is already being used in major companies in Japan, and >120 000 people have taken the test, so we can have some confidence in its validity.11 Fourth, this test does not fully cover the whole process of design thinking. Particularly prototyping and testing are not carried out, although the test simulates finding needs with empathy, redefining problems and discovering potential needs. Fifth, the biodesign process has been demonstrated in many countries, and there are some differences between the programs in each country. An international validation is therefore necessary to assess the development of design thinking skills from the biodesign program.
Conclusion
The biodesign process makes extensive use of design thinking skills and has been used within medical device start-ups in many countries. This is the first study to quantitatively evaluate whether the biodesign program fosters design thinking skills. This study suggests that the biodesign program is particularly effective in improving the ability to identify needs and generate solutions. Exposure of more people to the biodesign process may accelerate innovation in the MedTech field.
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
Acknowledgments
Many thanks to Tomoyuki Tajima, Mariko Koike, Mari Kobayahshi, Ryusuke Kameya, Nobuyuki Tanigaki, Masamitsu Nakayama, Atsushi Inaba, Jin Hayakawa, Hirotaka Ieki, Itsuki Osawa, Atsushi Tsujimoto, Jun Yokota, Emiko Ooba, Atsushi Yamada, Daisuke Inagaki, Susumu Miyazaki, Takayuki Uchida, Nanako Atsumi, Tokio Matsuzaki, Kentaro Hayashi, Takahide Murasawa, Tatsuya Kamon, Miho Hoshina, Yuki Hori, Koji Sato, Kensuke Niimura, Ken Matsuda, Taishi Nagata, Hironori Sunagawa, Takashi Sekiya, Yusaku Tagawa, Kenta Kitamura and Shu Sho.
Footnotes
HK and TK contributed equally.
Contributors HK, TK, YM and MS conceived of the presented idea. MM and TI performed the computations and verified the analytical methods. FI, IK and MO supervised the findings of this work. YM is the guarantor who accepts full responsibility for this article. All authors discussed the results and contributed to the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; internally peer reviewed.