Article Text

Abstract
‘Design with the user’ is a guiding principle for creating digital solutions to solve systemic developmental challenges. According to this principle, digital solutions are more likely to be effective if the intended users are involved in the design process, thereby rooting design thinking in a human-centric approach that seeks to understand their characteristics, needs and challenges. However, few examples exist for human-centred design (HCD) processes being successfully applied in low-and-middle-income countries to create digital health interventions that achieve both scale and sustainability. This paper describes the application of a five-stage HCD process to develop a suite of mobile solutions to improve reproductive, maternal, neonatal and child health in Bihar, India, and discusses lessons learnt. Two of the solutions were later adopted by the government and scaled to 10 million subscribers and more than 300 000 front-line health workers (FLHWs) in 13 states. The socio-ecological model, which considers the interplay between individual, interpersonal, organisational, community and public policy factors, provides a conceptual framework for understanding key learnings from the HCD process. At the organisational level, we found that demand generation was constrained by deficiencies in the public health system, while at the community level, gender norms were a barrier to changing health practices. At the interpersonal level, mobile health solutions for mothers also had to address fathers, because they controlled women’s access to mobile phones. At the individual level, FLHWs had limited time to build their skills and needed more flexible, home-based learning opportunities; most FLHWs had access to mobile phones, but devices were overwhelmingly basic and digital skills limited; voice technology was required to maximise reach among low literate women and an authoritative yet empathetic narrator was required to humanise the digital experience, lend credibility and create engagement.
- Child Health
- Public Health
- Reproductive Health
- Women's Health
- Primary Healthcare
This is an open access article distributed in accordance with the Creative Commons Attribution 4.0 Unported (CC BY 4.0) license, which permits others to copy, redistribute, remix, transform and build upon this work for any purpose, provided the original work is properly cited, a link to the licence is given, and indication of whether changes were made. See: https://creativecommons.org/licenses/by/4.0/.
Statistics from Altmetric.com
Introduction
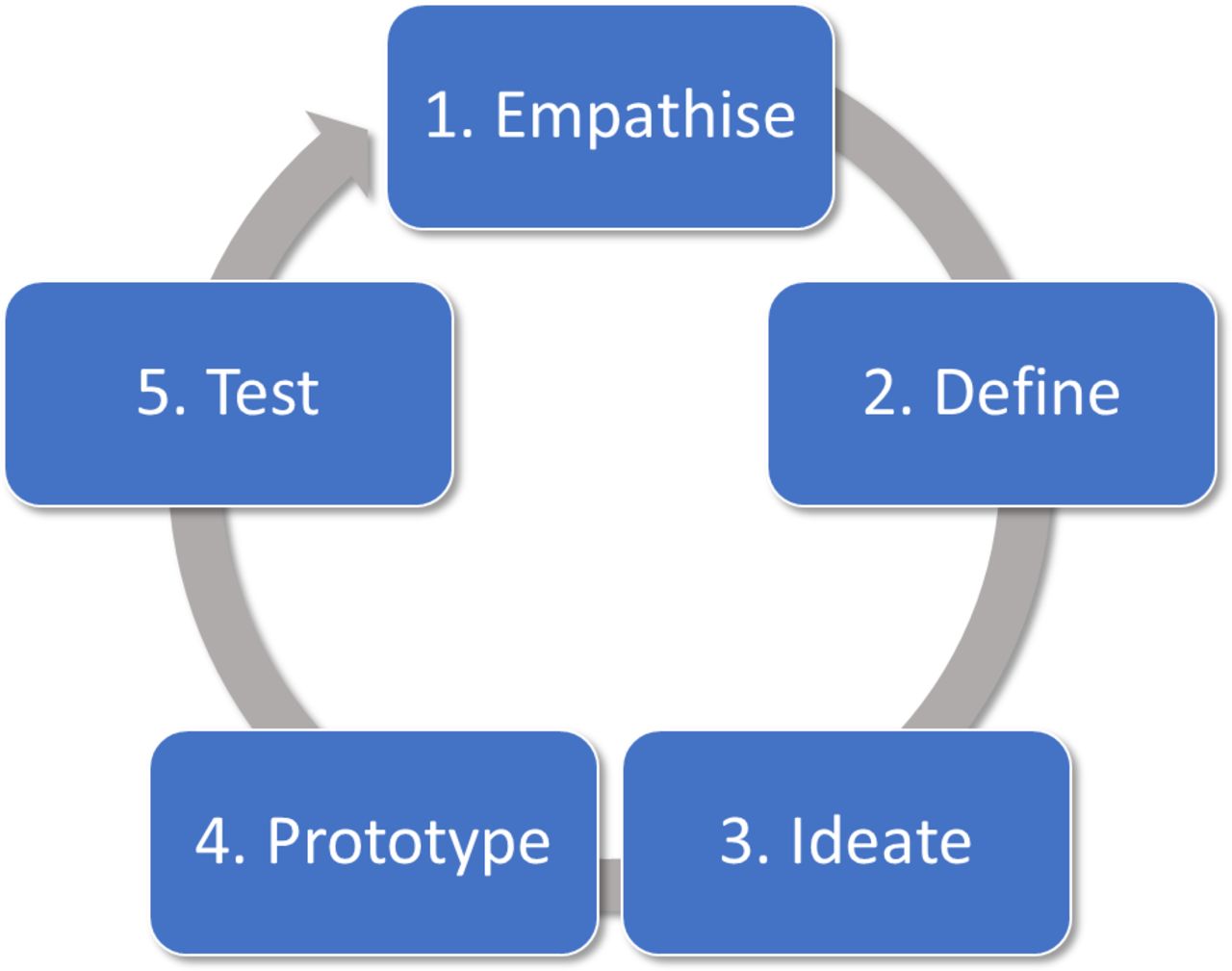
‘Design with the user’ is considered a guiding principle for creating digital solutions to solve systemic developmental challenges.1 According to this principle, digital solutions are more likely to be effective if the intended users are involved in the design process, thereby rooting design thinking in a human-centric approach that seeks to understand their characteristics, needs and challenges.1 2 A global conversation has been unfolding for decades about how to effectively approach and structure the human-centred design (HCD) process to solve complex problems.3 Stanford University, one of the leading voices in this conversation, defined a five-stage process as follows: empathise, define, ideate, prototype and test (figure 1).2

Five-stage human-centred design (HCD) process.
Building on its own experience of applying HCD approaches to tackle systemic developmental challenges, BBC Media Action applied Stanford University’s approach to design a digital behavioural change communications programme to strengthen families’ reproductive, maternal, newborn and child health (RMNCH) practices and to generate demand for public health services in the north Indian state of Bihar between 2011 and 2013. The programme aimed to strengthen practices in 11 behavioural areas (see table 1.)
Health practices covered by the programme
This HCD process resulted in a complimentary suite of digital health solutions: Mobile Academy, a training course to refresh front-line health workers’ (FLHWs) knowledge of RMNCH behaviours and improve their interpersonal communication skills; Mobile Kunji (meaning guide or key in Hindi), a job aid to support FLHWs’ interactions with families; and Kilkari (meaning baby’s gurgle in Hindi), a mobile messaging service that delivered weekly, stage-based, time-sensitive audio information directly to the phones of pregnant women, new mothers and their families’ to reinforce FLHWs’ counselling.4 In 2014, two of the services were adopted by the Indian government and collaboratively scaled to 13 states. As of April 2019, when BBC Media Action transitioned Mobile Academy and Kilkari to the Ministry of Health and Family Welfare, they constituted two of the largest mobile health communication programmes in the world.5 Although Mobile Kunji was regularly used by more than 50 000 FLHWs for 7 years in Bihar, scaled to close to 200 000 FLHWs in the states of Odisha and Uttar Pradesh and had a significant impact on a range of health outcomes, it was not adopted at the national level.5 In this practice paper, we reflect on the process undertaken to design these digital solutions, highlighting lessons learnt and considerations that we hope will be useful for practitioners designing digital health solutions in low-and-middle-income countries.
Background
In collaboration with the state government and with support from the Bill & Melinda Gates Foundation, BBC Media Action first began work on Mobile Academy, Mobile Kunji and Kilkari in the Indian state of Bihar in 2011. At the time, data indicated that Bihar had some of the worst maternal, neonatal and infant mortality rates in both India and the world.6 The maternal mortality ratio was 305 per 100 000 births and the infant mortality rate stood at 55 per 1000 live births.6 The percentage of babies dying on the day of their birth was 16%, and as many as 42% of Bihar’s 15 million children under the age of 5 were underweight.7 Bihar’s mothers were also bearing more children than women in any other part of the country.8
Bihar’s health sector was characterised by significant infrastructure and human resource deficiencies, but by 2011 this was changing. In addition to stimulating economic growth, investing in education for girls and improving law and order, the state government was focusing on improving health outcomes. State health expenditure was growing by 15%–20% annually, and increasing numbers of health workers, including doctors and front-line workers, were being recruited.
To help accelerate progress towards the state of Bihar’s goal of reducing maternal and infant mortality, the government entered into a 5-year partnership with the Gates Foundation. Through this partnership—which was called Ananya (Hindi for ‘unique’)—the Gates Foundation and its partners focused on the critical 1000 days between the start of a pregnancy and a child’s second birthday, which is when most preventable deaths occur.
BBC Media Action was one of the partners in the Ananya programme. Its mandate was to stimulate demand for public health services and strengthen the practice of 11 priority health behaviours that are proven to save lives (table 1). It set about designing communication solutions, using a HCD approach.
Stage 1: Empathise
Empathy has been described as ‘the foundation of a HCD process’—a process involving: (1) observation—‘view users and their behaviour in the context of their lives’; (2) engagement—‘interact with and interview users through both scheduled and short “intercept” encounters’ and (3) immersion—‘experience what your user experiences’.3
To design Mobile Academy, Mobile Kunji (key in Hindi) and Kilkari (baby’s gurgle in Hindi), a multidisciplinary project team (social and behavioural change communication specialists, health experts, researchers and creative and digital strategists and designers) used a range of techniques to observe, engage and immerse themselves in the lives of FLHWs, rural women and their families in Bihar. These techniques included: (1) immersion trips, where two teams of six-to-eight people—working in pairs—each conducted two-to-three in-depth interviews and one focus on group discussion per day in different districts of Bihar over the course of a week to understand the lives of rural families and FLHWs. The teams also observed their daily routines and informally engaged with rural communities throughout the week; (2) extensive desk research to review existing literature on the political economy, the strengths and weaknesses of the FLHW programme in India, the efficacy of digital interventions for social impact in India and other countries, and social and behavioural change communication theories of change for improving health outcomes; (3) a baseline survey of RMNCH knowledge, attitudes and practices among a sample of 1137 husbands, 1085 mothers-in-law and 3893 women with children under 2 years of age and 453 pregnant women representative of the population in eight districts in Bihar; (4) a survey of the mobile access, usage and expenditure habits of a sample of 550 FLHWs and 1500 women and men representative of the population in eight districts in Bihar and (5) engagement with key stakeholders such as other Ananya partners, public health experts and government officials.
A key objective of this stage in the process was to identify barriers to changing RMNCH practices (such as social norms, religious traditions, economic priorities, class, caste, religion and levels of media exposure and digital access and use), as well as insights into catalysts for change. It helped the team gain an understanding of the ‘lived experiences’ of poor, rural women—from girlhood through to motherhood—and their access to services, levels of mobility and agency in making decisions about their pregnancies and the birth of their children and how they cared for their babies.
Stage 2: Define
In stage 2 of the HCD process, qualitative and quantitative data from the formative research described in stage 1 were analysed by BBC Media Action’s research team to ‘define the problem’—that is, to identify barriers to change. As part of this process, the team identified the following barriers to changes in health practices at scale.
Inequalities in health access
The formative research identified inequalities in access to healthcare in Bihar, where health workers from one religious tradition might not visit new and expectant mothers from another in their catchment areas, and lower-caste communities were often excluded from public health services.
Existing social norms around key target behaviours
The formative research identified a powerful web of social norms and traditions that regarded women’s bodies as impure. These cultural beliefs and norms led to behaviours such as discarding the ‘impure’ first breast milk (the highly nutritious colostrum), washing a baby to remove its ‘polluted’ coating from the womb (which in fact protects the baby from infection) and putting ‘medicine’ on the umbilical cord to heal it (which can lead to infection).9 To compound the problem, husbands in Bihar considered pregnancy and childbirth to be women’s issues, which their mothers and wives should handle. Men did not involve themselves in discussions about maternal and child health. Family planning was a taboo subject for all, hidden by a culture of silence and concealment.
Limited agency among new and expecting mothers
The formative research identified family power dynamics that excluded young wives from decision-making about their own health and the health of their children. Daughters-in-law had few opportunities to leave the home and had little access to external sources of information. They also had little interaction with their husbands and had a limited role in family planning decisions. Instead, mothers-in-law typically controlled most health-related decisions. A socially pervasive preference for sons meant that many families put pressure on their daughters-in-law to continue having children until they had a son.
Decision-making and access to phones controlled by gatekeepers in the family
The formative research identified that husbands supported a decision-making hierarchy that privileged their mothers over their wives. Research also found that husbands usually had primary control over household finances and, along with their own parents, took most of the household decisions. Although mobile phones were identified as a channel with high household penetration, husbands controlled access. Therefore, any mobile-based health communication intervention designed to reach pregnant women and new mothers would need to be mediated by these gatekeepers. FLHWs were identified as key potential change agents with socially sanctioned access to new and expectant mothers.
Most women, including FLHWs, had access to a mobile phone—but these phones were basic, and their digital skills were limited
Research identified that in 2011, 51% of the female population in Bihar was illiterate.10 Only 18% of women of reproductive age watched television and only 12% listened to the radio.11 In contrast to low levels of mass media penetration, BBC Media Action’s mobile access and use survey found that 80% of households and 90% of FLHWs in Bihar had access to a mobile phone.12 However, more than 98% of these devices were basic phones without internet access. Moreover, digital literacy levels were incredibly low—with only 9% of FLHWs ever having sent a text message. Women also struggled to navigate the complex interactive voice response (IVR) menus that most mobile network operators used for call centre support.
FLHWs had little time to build their skills and few job aids
Because FLHWs visited poor, rural women directly in their homes, FLHWs were thought to be one of the most effective channels for strengthening families’ health practices. Formative research revealed that they themselves faced constraints in providing support to families. They were from the same villages and socioeconomic backgrounds as the families they aimed to serve and often had comparable levels of education. Although the Indian government required FLHWs to have completed the 10th grade, more than 30% had low literacy skills or were even illiterate in Bihar in 2011. As such, their clients often did not take them seriously. FLHWs also had limited time to build their skills on an ongoing basis. Some lived far from centres of learning and lacked the financial means to travel, while others had family obligations that prevented them from accessing formal training programmes. Most FLHWs also had few job aids, and the flip charts that they were supposed to use during their interactions with families were so cumbersome that few FLHWs carried them during their household visits.
Deficiencies in the public health system posed a challenge to shaping demand and practice
The formative research identified deficiencies in the public health system, including in human resources, supply chains and infrastructure, which posed a challenge to interventions designed to generate demand for public health services. For example, in Bihar in 2011, an irregular supply of iron and folic acid (IFA) tablets to primary health centres made it challenging to ensure women’s timely and continuous consumption of IFA tablets during pregnancy. Despite these constraints, a decision was made, in close collaboration with the Bihar state government and donors, to proceed with the design process. The conclusion was that a public with a greater level of health knowledge would be better able to place constructive demands on the public health system and hold it to account for the quality of its services than families with no information about their rights and entitlements.
Stage 3: Ideate
Based on learning from stages 1 and 2 of the HCD process, an overarching theory of change for a suite of mHealth services to improve RMNCH outcomes among families in Bihar was developed.13 It was based on the hypotheses that: (1) providing timely, accessible, accurate and relevant information improves knowledge; (2) however, while knowledge is necessary, it is insufficient to change behaviour; (3) negotiations between FLHWs and families are critical to improving the self-efficacy of families; (4) discussion is often a gateway to change and (5) increased knowledge and better interpersonal communication skills will make FLHWs more confident and motivated.
A communications framework and technical briefs were then created by the multidisciplinary project team to detail the communication strategy and content required to deliver on the theory of change. Ideas were then generated through a series of brainstorming sessions for a complementary suite of digital solutions for FLHWs and families to support these pathways to change. The first set of ideas focused on how to improve FLHWs’ knowledge of RMNCH practices and their interpersonal communication skills. The starting point was how existing digital health solutions with promising evidence from other geographies could be reused and improved in the Indian context. This approach (reuse and improve rather than starting from scratch) has subsequently been identified as one of the key principles of effective digital development.14 Stage 1 of the HCD process had identified BBC Janala, a multiaward winning IVR-based training course designed to teach English for livelihoods in Bangladesh, as a digital solution with potential for replication in Bihar.15 IVR was identified as an appropriate technology because it overcame the challenges of low literacy and negligible smartphone ownership in the state. The programme then considered how the BBC Janala IVR application could be adapted to provide FLHWs with high quality, standardised learning, which that they could pursue at their own convenience. This design thinking resulted in Mobile Academy, an interactive IVR-based training course for FLHWs, which aimed to refresh their RMNCH knowledge and improve their interpersonal communication skills and uses an intuitive, linear to navigation.
Recognising that change would be slow unless FLHWs were also equipped with tools to improve the quality of their engagement with families, the team generated ideas for job aids. The challenge was how to cover 11 health behaviours and more than 100 simple, doable actions in one lightweight, low-cost, scalable audiovisual job aid. This was no easy task, given that a negligible number of FLHWs owned smartphones. Microexperiments, consisting of in-depth interviews with FLHWs in Bihar, were conducted to gather feedback on a range of innovations on the traditional flip chart. The research identified that the flip chart had to be lightweight, because FLHWs often walked long distances to visit their clients. It also had to fit into FLHWs’ purses, because FLHWs were reluctant to carry anything else. The team experimented with equipping FLHWs with small, lightweight ‘Pico Projectors’ to play audiovisual content to families, but procurement and maintenance of the projectors were identified as roadblocks to government adoption and sustainability at scale. Finally, the team conceived the idea for Mobile Kunji: a job aid consisting of a lightweight deck of 41 illustrated cards made of durable credit card material, each with talking points on the back, and an illustration and a unique mobile short code (five-digit mobile number) on the front.16 FLHWs would use the deck like a flip chart in their counselling sessions with families, but could also dial the short codes to play audio content related to each card via the speakers on their basic mobile phones. This approach to unpacking the IVR navigation overcame the challenges that FLHWs had with navigating complex IVR menus and created a low-tech audiovisual job aid that FLHWs could use with their existing mobile phone.
In addition to digital solutions for FLHWs, ideas were generated for digital ‘direct to beneficiary’ communication solutions to reinforce the information shared by FLHWs with families, and to send timely reminders about critical health practices. Stage 1 of the HCD process had identified an IVR messaging pilot programme for pregnant women in Ghana called Mobile Midwife, which was showing promising results, and had potential for replication in India. Ideas were generated for how to adapt Mobile Midwife to meet the needs of families in Bihar, based on the learning from stages 1 and 2 of the process.
Stage 4: Prototype
The ideation phase of the HCD process resulted in prototypes for a suite of three mHealth services (Mobile Academy, Mobile Kunji and Kilkari). Paper-based prototypes and then fully functional IVR prototypes were developed by BBC Media Action’s multidisciplinary team, working with its technical partners, OnMobile and the Grameen Foundation, for user testing in Bihar. Prototypes for Mobile Academy and Mobile Kunji were iteratively developed and tested over the course of 6 months, while Kilkari prototypes were iteratively developed and tested (see stage 5) over 9 months. After the user testing was completed, final versions of all three mHealth solutions were developed, which covered the 11 behavioural areas listed in table 1.
The content of the mHealth services was narrated by one voice—Dr Anita, who was designed to act as a friend, philosopher and guide for FLHWs and families. This fictional doctor character was created to humanise users’ experiences of automated mobile-based communication, which many had never experienced before. Dr Anita was born from step 1 of the HCD process, which identified that in Bihar in 2011, some families might go through their entire lives without seeing a doctor and would welcome ‘a doctor in their pocket’. Formative research had also identified that men—who owned most phones in rural Bihar and controlled women’s access—would need to hear from an authority figure that they considered credible. Women also wanted advice from a trustworthy source, but empathy too. The tonality of Dr Anita, who addresses FLHWs or fathers and mothers at the beginning of every call, was crafted to try to achieve a delicate balance of empathy and authority.
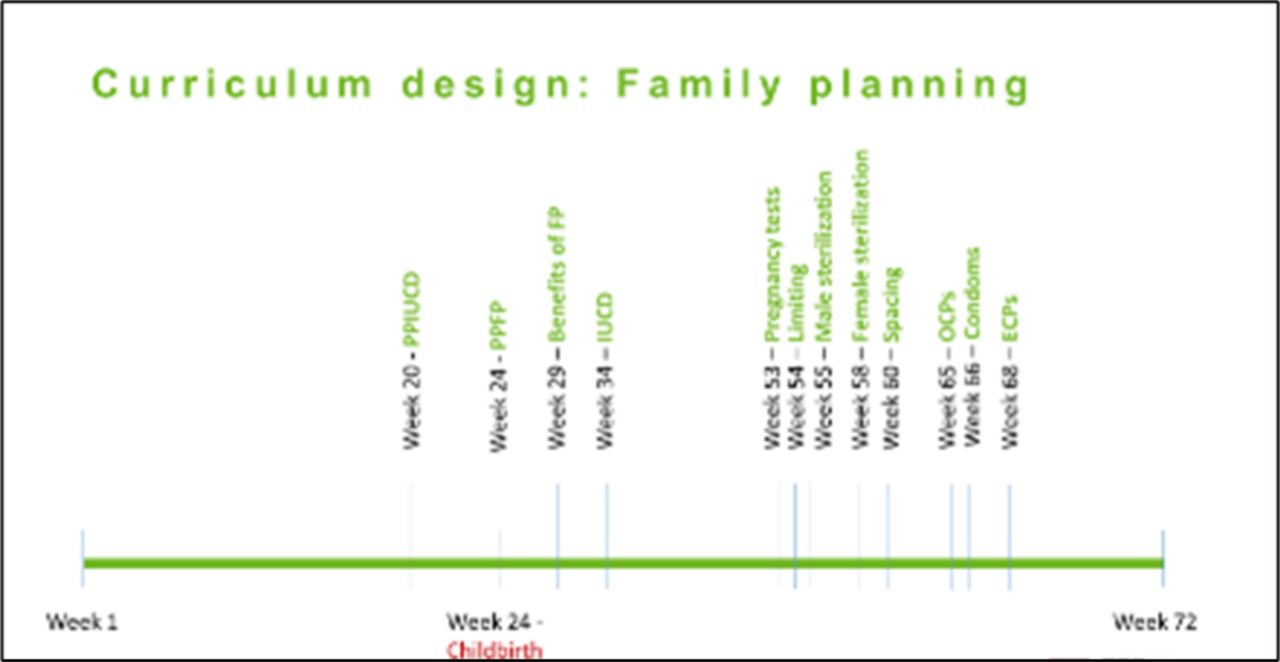
The content strategy for the mHealth services also ensured a balance of content across all 11 behavioural areas, and adequate repetition of information across calls to enhance recall, without boring users. The scope of the content evolved after two of the mHealth services was adopted by the Ministry of Health and Family Welfare in 2014. For example, the family planning content in Kilkari was expanded to make 12 family planning calls, distributed across 72 weeks, to subscriber at the most appropriate times (see figure 2).
{kind=link}
{kind=link}
Schedule of family planning content in Kilkari.
Stage 5: Testing
The paper-based prototypes, consisting of accessible summaries of the concepts for each service and sample audio content, were qualitatively tested with FLHWs and families via in-depth interviews to explore and assess user demand and willingness to pay for each of the mHealth services. Responses to all three concepts were positive. However, although FLHWs were willing to pay for Mobile Academy, which they considered valuable career development, they were not willing to pay to use Mobile Kunji. Understandably, they thought the government should pay for job aids for health workers. Fathers were willing to pay for Kilkari—but only a nominal fee. These learnings were used to design the ingoing business model for the services.2 Based on these test results, fully functional IVR prototypes were then developed.
A portable, low-tech laboratory was used to iteratively engage with FLHWs and low literate pregnant women and mothers in eight districts in Bihar to test the IVR prototypes. This task-based user testing had two key objectives: (1) to identify whether respondents could comprehend and recall content, and whether they thought it was relevant and engaging and (2) to identify whether respondents could understand and respond to IVR navigational prompts. Sixty-four user tests were conducted in eight districts of Bihar for Mobile Academy, and another 64 for Mobile Kunji. More than 100 user tests were iteratively conducted in eight districts of Bihar over the course of 6 months to design Kilkari. Each user test was typically one and half hours long. These user tests were filmed with respondents’ consent, so that the multidisciplinary project team could observe and learn from their facial expressions and body language as they accessed the IVR prototypes from their own phones and performed navigational tasks. The team also used a more ethnographic, observational approach to assess user engagement with the Kilkari prototypes. Thirty-six pregnant women and mothers of babies in three locations were subscribed to Kilkari with their consent (12 per location). Researchers then observed what happened when Kilkari calls reached their families’ phones for 2 weeks. The learnings from this stage in the HCD process are summarised below (table 2).
Ten learnings from the prototype testing
Conclusion
After the services were piloted with 50 000 FLHWs in Bihar and research studies revealed a positive impact on multiple health outcomes, Mobile Academy and Mobile Kunji were scaled to Odisha and Uttar Pradesh in collaboration with state governments. After the national government decided to adopt the services in late 2014, the national scale up of Mobile Academy and Kilkari began in January 2016. Over the next 3 years, the government scaled the services to 13 states with BBC Media Action’s support. By 2019, when BBC Media Action made its planned exit from the programme, 206 000 FLHWs had graduated from Mobile Academy, and Kilkari had reached 10 million subscribers, who had listened to more than 200 million minutes of content.
Research studies indicate that Kilkari has had a significant impact on some health outcomes, including the adoption of modern contraceptive methods and has been identified as a ‘highly cost-effective’ approach to saving lives at scale.17 18 Mobile Academy has been identified as an effective tool for refreshing FHLWs’ knowledge, as well as a mechanism for modelling a more effective style of interpersonal communications.19 Although Mobile Kunji was not scaled by the national government because it was thought that FLHWs would soon have personal smartphones, research indicated that it was associated with improvements in a range of health outcomes.20 These results suggest that HCD processes, when effectively applied, can be invaluable in creating impactful digital solutions that resonate with communities and have a strong potential for scale, sustainability and health system integration.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
Footnotes
Twitter @child health
Contributors This practice paper describes the application of a five-step user-centered design (UCD) process to create one of the largest mobile health communication programmes in the world. SaC, PD and RM co-led the adaptation and implementation of the UCD process in India to design the suite of mobile health solutions discussed in this article. AG contributed to the design of research studies to monitor the progress of the two mobile health interventions. AEL was the principal investigator (PI) for the programme of research to evaluate the impact of Kilkari. KS was the PI for the qualitative research to explore the impact of Kilkari and user responses to Mobile Academy. SK played a key role in implementing the UCD process and contributed significantly to the learning articulated in this article. JM helped develop and test prototypes for the suite of mobile health solutions as part of the UCD process and contributed significantly to the learning articulated in this article. ShC was the Producer at BBC Media Action in India responsible for creating much of the content for the suite of mobile health solutions as part of the UCD process and contributed significantly to the learning articulated in this article.
Funding This study was funded by Bill & Melinda Gates Foundation (OPP1179252).
Disclaimer The authors alone are responsible for the views expressed in this article, and they do not necessarily represent the decisions or policies of PAHO or TDR. In any reproduction of this article there should not be any suggestion that PAHO or TDR endorse any specific organisation services or products.
Competing interests SaC, PD, RM, SK, JM and ShC report grants from the Bill & Melinda Gates Foundation, grants from US Agency for International Development, grants from the Barr Foundation, during the lifetime of the project.
Patient and public involvement statement Not applicable- article content draws from the experiences of study authors designing, implementing, and evaluating digital solutions in India and elsewhere globally.
Provenance and peer review Not commissioned; externally peer reviewed.