Article Text

Statistics from Altmetric.com
Summary box
What are the new findings?
We describe the design and evaluation of a touchless peritoneal dialysis connector system showing reduced incidence of bacterial contamination in comparison with the standard of care.
How might it impact on healthcare in the future?
Integrating the touchless connector system into peritoneal dialysis systems may help reduce peritonitis risks in patients.
Background
Introduction
Peritoneal dialysis (PD) is one of the options available for treating end-stage kidney disease, the last stage of chronic kidney disease in which the organs no longer work enough for a patient to survive without dialysis or a transplant. In the option most people know, haemodialysis, patients visit a dialysis centre thrice weekly to use a machine that filters excess fluid and solutes from their bloodstream. In PD, these excess fluids and solutes are filtered via a membrane in the abdomen called the peritoneum. The space of the peritoneum is filled with dialysis fluid through a catheter implanted in the abdomen (the permanent peritoneal catheter); osmotic and concentration gradients between the blood and the fluid lead to the removal of excess body fluids and solutes, respectively. It is the preferred option for dialysis for children with blood volumes too small for circulation in a haemodialysis machine.
There is renewed interest in PD in both high-income and low-income and middle-income countries. In the USA for example, a new payment model introduced by the Centers for Medicare and Medicaid Services is incentivising physicians and providers to increase the proportion of patients on home therapies like PD.1 The COVID-19 pandemic and the desire for social distancing also increased PD demand.2
In low-income and middle-income countries, recent studies have drawn attention to how limited access to kidney replacement therapy may result in up to 7 million deaths yearly, more than the deaths from HIV and tuberculosis combined. Less than a third of patients in Asia and only 16% of patients in Africa are said to receive needed treatment, mostly due to unaffordable costs.3 In the 2019 Global Kidney Health Atlas, the International Society of Nephrology has recommended a PD first treatment approach as a potential solution to this problem.4
Despite the potential benefits, PD uptake continues to be limited and this is due in part to concerns about peritonitis—an infection of the peritoneal membrane through which the therapy occurs. Almost a century since Georg Ganter first described PD in a 1923 paper,5 peritonitis continues to be a common and serious complication globally.6 7 It is the direct or major contributing cause of death in >15% of patients and the most common reason patients stop the therapy. Peritonitis leads to repeat episodes in 3%–20% (14% overall), surgeries for peritoneal catheter removal in 10%–88% (22% overall), permanent transfer to haemodialysis in 9%–74% (18% overall) and death in 0.9%–8.6% (2%–6% overall).8–11 Strategies to prevent peritonitis are urgently needed.
Peritonitis, causes and prevention
There are different causes for peritonitis, including catheter contamination, infection of catheter exit site or tunnel, intestinal bacteria, bacteria in patient blood or even infections ascending from uterine or vaginal sources.12 However, contamination of the peritoneal catheter while patients connect for treatment is the most common cause. More than 50% of peritonitis episodes are caused by bacteria colonising the skin or mucous membranes and touch contamination alone contributes to over 40% of peritonitis episodes.13 14
In a 2018 review, Salzer reported that ‘most cases of PD-related peritonitis are the result of touch contamination’ and this was consistent with findings from the 2016 report of the Standardizing Care to Improve Outcomes in Pediatric ESRD, where touch contamination was associated with a higher risk of peritonitis (RR 2.22; 95% CI 1.44 to 3.34).15 16 Contamination of the catheter by respiratory droplets is also an important source as nasal bacterial carriage can increase risk of peritonitis in patients. When compared with non-carriers, carriers had a twofold to sixfold higher incidence of Staphylococcus aureus peritonitis,17 and studies using phage typing of S. aureus from the patients with peritonitis found that in most cases, the isolates were the same as in the nostrils.18–20
The International Society for Peritoneal Dialysis (ISPD), a global authority on PD, which has published recommendations for treatment and prevention of peritonitis for over 30 years recommends that peritonitis rates for a dialysis centre be below 0.5 episodes per patient-year. This means that for a dialysis provider with 100 patients undergoing PD for a year, the total number of peritonitis episodes recorded in that year should be below 50. Yet, the rate reported from providers in different countries and within the same country continues to vary widely. For example, reported rates range from 0.06 episodes per patient-year in Taiwan to 1.66 episodes per patient-year in Israel and there have been up to 20-fold variation in the reported rates within Australia, Austria, Scotland and the UK. While the sources of these variations are poorly investigated, they may be due to factors like each provider’s patient population or their PD training practices.11
In the most recent guidelines,21 the ISPD recommends rigorous training in aseptic technique to reduce rates from patient-related sources of peritonitis. Providers also train new patients and retrain them after peritonitis episodes. The patients are expected to report any breach in the aseptic technique, so further actions can be taken to prevent peritonitis, for example, changing the catheter extension sets, or administering antibiotics.22
This reliance on patients to control peritonitis is however problematic, as fewer than 50% of patients remain adherent to their training after 6 months of commencing therapy.23 This might also explain why many providers restrict PD to patients whom they feel will comply with training while excluding many otherwise eligible patients.24
Essentially, the wide variation in peritonitis rates and the selective prescription of PD reveal gaps in peritonitis prevention and the need for innovation. The increasing demands for PD across the world, from payment changes in favour of cost-effective home therapies, to the attempts at increasing access and affordability of dialysis in low-income and middle-income countries, make it even more crucial that solutions that better prevent peritonitis be developed.
In this paper, we describe the design and proof-of-concept evaluation of a touchless connector system that has the potential to reduce PD-associated peritonitis.
Methods
Premise and design
The theory behind the design of the touchless connector system is that eliminating inadvertent contamination of the peritoneal catheter will reduce peritonitis episodes by up to 50%, the proportion of peritonitis episodes caused by skin or mucous membrane bacteria.13
Studies investigating how different connection points in a PD system contribute to peritonitis are limited but by interviewing PD nurses, we found the catheter extension set (also called transfer set) to be a vulnerable connection point common to both manual and automated devices. In manual PD, called continuous ambulatory peritoneal dialysis (CAPD), the catheter extension set is the only connection point when a double bag (fluid bag with pre-attached drain bag) is used. The potential for contamination may also be higher since these patients have to connect their catheter extension set for therapy multiple times daily. In automated PD (APD) using a cycler, patients typically connect their catheter extension set for therapy once daily but there are other vulnerable connection points, for example, connection to fluid bags, drainage bags, etc. However, there is evidence suggesting that the automated flush-before-fill mechanisms of the cyclers may reduce contamination,25 leaving the catheter extension set as the remaining vulnerable component in this modality as well.
Based on these findings, the functional need was established as ‘a way to help PD patients connect/disconnect catheter extension sets for therapy without contamination’.
In existing PD systems, the catheter extension set extends from the permanent catheter implanted in the patient’s abdomen (figure 1). It has a disposable disconnect cap, which protects it from contamination when not being used for therapy. Every day, or multiple times daily in CAPD, when patients transfer dialysis fluid into their peritoneum, they first remove and discard this disconnect cap before connecting their catheter extension set to the dialysis fluid source. After completing therapy, they disconnect from the dialysis fluid source and cover the catheter extension set with a new disconnect cap. Depending on patient compliance with training, these moments when the catheter extension set is open could result in contamination of the peritoneal catheter and eventual peritonitis.
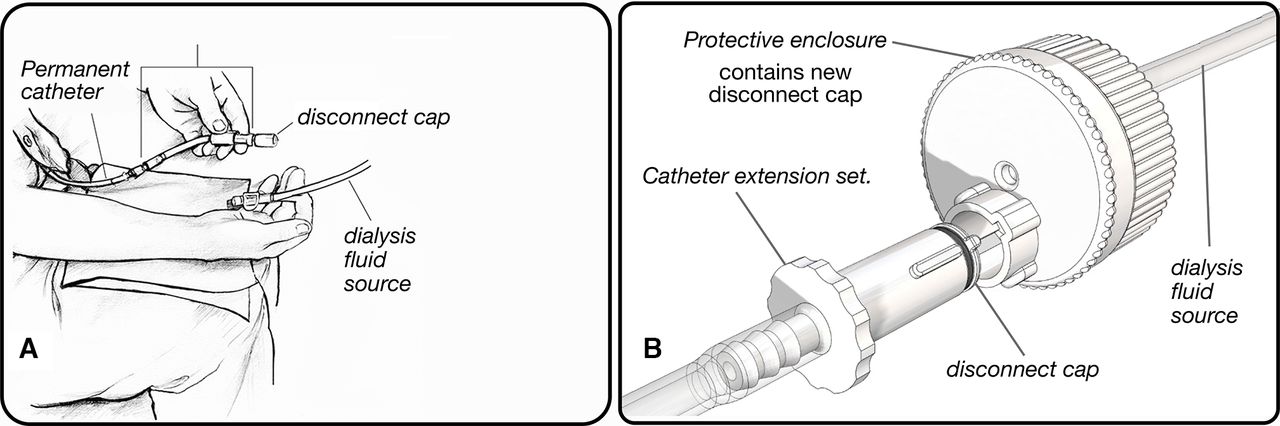
Peritoneal dialysis connector system designs. (A) Standard of care connector system, (B) touchless connector system.
In order to meet the established need, we identified six design criteria which drove the development of the touchless connector system.
Remove the old disconnect cap on the catheter extension set without physical contact.
Eliminate contact between the old, contaminated disconnect cap and the catheter extension set after cap removal.
Connect and disconnect the catheter extension set to the dialysis fluid source without physically contacting either.
Connect a new, sterile disconnect cap to the catheter extension set after therapy without physically contacting either.
Protect the entire process from aerosols via an enclosure.
Provide patients with a step-by-step, error-free process for connecting their catheter extension set to a dialysis fluid source.
Multiple ideas were generated, screened and optimised before arriving at the underlying concept for the touchless connector system. In this concept, the components of interest, that is, catheter extension set, disconnect cap and connector to the dialysis fluid source have been redesigned as shown in figure 1.
The operation of the touchless connector system (table 1) is similar to that described above for existing systems. However, in this design, removal of old disconnect caps from the catheter extension set; connection of the catheter extension set to dialysis fluid source for fluid exchange and recapping of the catheter extension set with a new disconnect cap, all take place within a protective enclosure. This enclosure is unique to the touchless connector system and is a redesign of the connector to ‘dialysis fluid source’ in existing systems (figure 1). It also contains a new, sterile disconnect cap that will cover the catheter extension set after therapy is completed. It is a disposable component discarded with the dialysis fluid source (fluid bag in CAPD or cycler sets in APD) and used disconnect cap after therapy.
Connecting and disconnecting for therapy with touchless connector system
To develop the concept, we used an iterative design methodology, advancing through multiple three-dimensional printed prototypes (figure 2) based on feedback from nephrologists, nurses, patients, large dialysis organisations and manufacturers. In total, 118 interviews were conducted across the USA between June and November 2019. The findings from 57 of these interviews with PD providers and an anonymous survey in 6 PD centres helped validate the functional need and value proposition. From all interviews, the team gathered insights on required device characteristics, manufacturing goals and compatibility with existing PD systems.
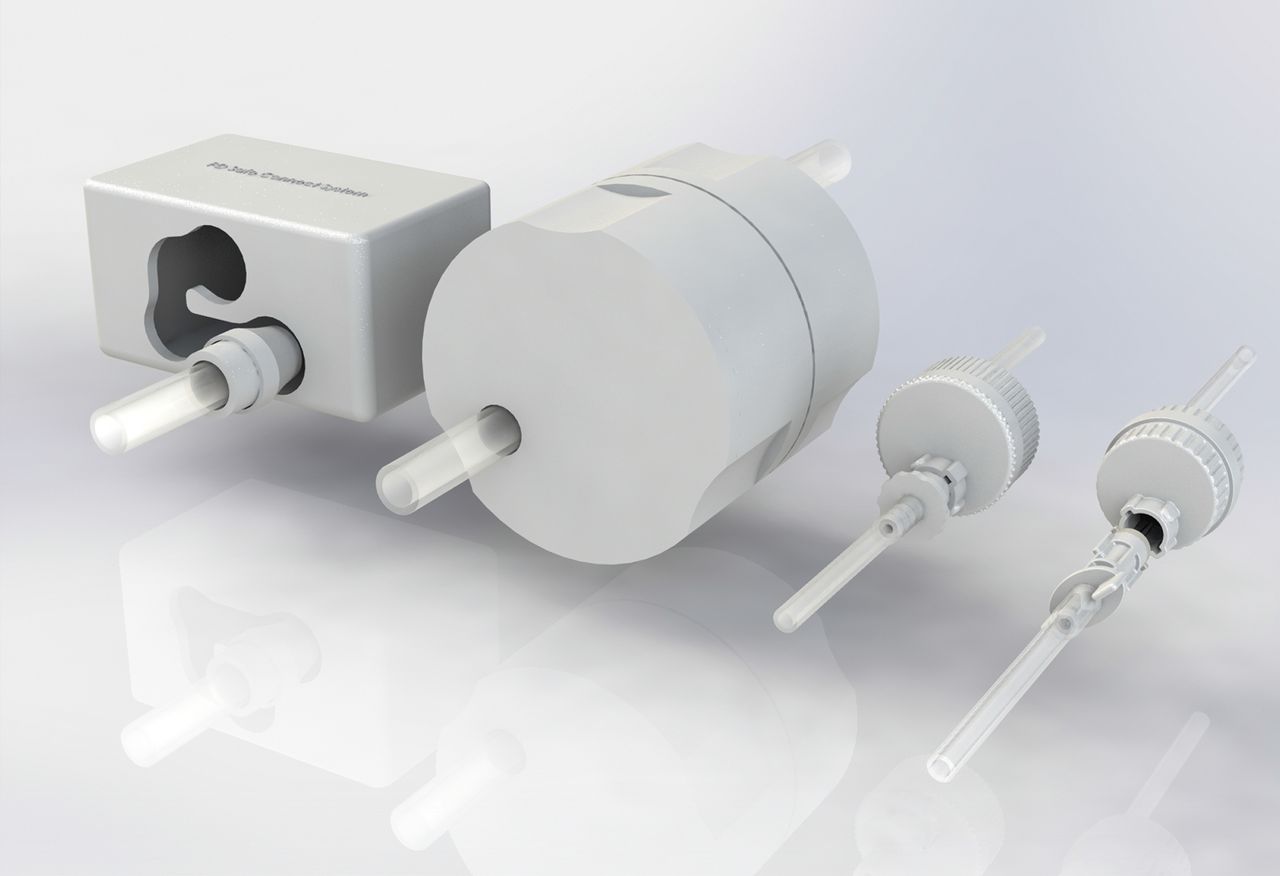
Three-dimensional rendering showing design evolution of the touchless connector system.
In fall 2020, the team conducted a usability study with seven participants to understand and optimise usability of the touchless connector system for patients.
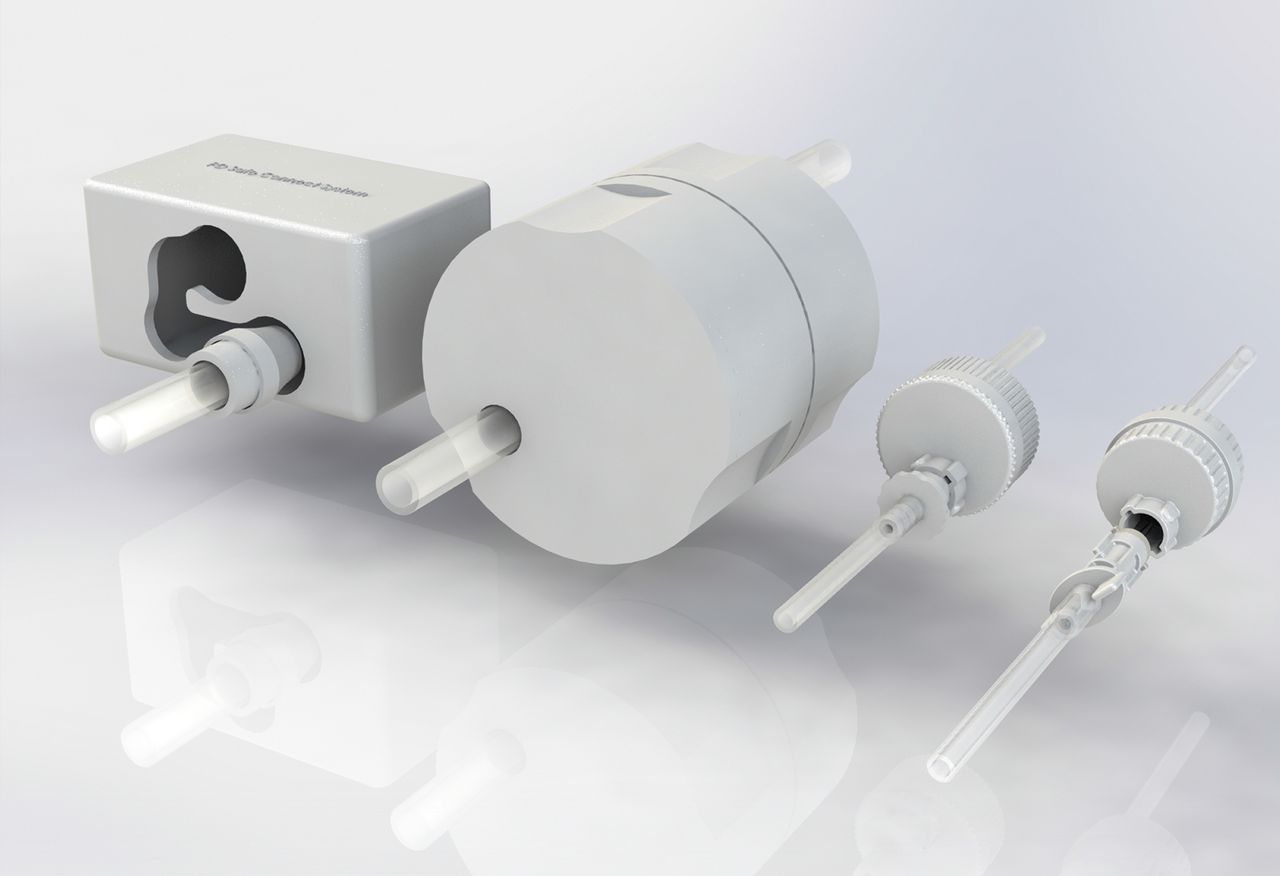
The outcome of this iterative design process is the current injection moulded prototype (figure 3) of the touchless connector system used in the proof-of-concept evaluation.

Current injection moulded prototype of touchless connector system.
Proof-of-concept evaluation
Rationale/Study aims
Since the touchless connector system differs from the standard of care in its ability to prevent touch/aerosol contamination during therapy, we sought to evaluate this experimentally. A reduction of peritonitis episodes will be the most desired validation but this is not practical with current development stage and resources. We have therefore used an approach that simulates a worst-case scenario and assesses the ability of connector systems to prevent contamination.
Materials
Touchless connector system prototypes; samples of a commonly used connector system (standard of care); sterile dialysis fluid bags; 100 mL effluent sample bags.
Test devices for both systems were pre-assembled and sterilised with ethylene oxide before being used to form the setup in figure 4.
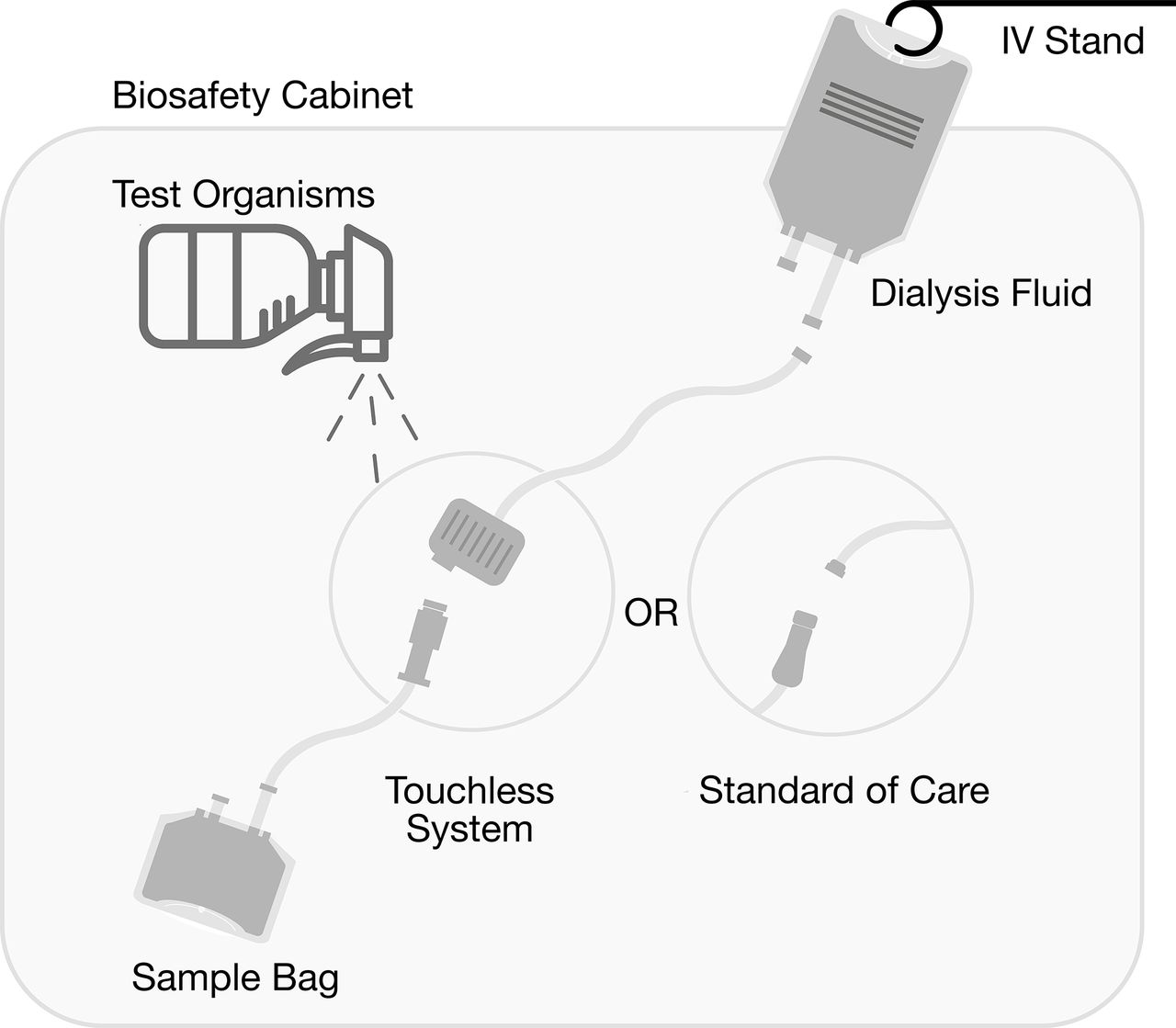
Experimental setup.
Staphylococcus epidermidis (SE) ATCC1228 and Pseudomonas aeruginosa (PA) ATCC39327, representing the most commonly observed Gram-positive and Gram-negative bacteria, respectively in peritonitis,26 were used as the test organisms.
Experimental setup
The experiments were performed within a laminar flow biosafety cabinet in a biosafety level 2 laboratory facility to control the test environment. Experimental setup (figure 4) included a dialysis fluid bag suspended from an intravenous pole, and connected to one end of the test devices, that is, the dialysis fluid source connection, making it available for participants within the biosafety cabinet. The other end of the test devices consisted of the catheter extension set for the touchless connector system or standard of care pre-attached to the effluent sample bags. The effluent sample bags represent the peritoneal space into which dialysis fluid will flow during therapy, and within which contaminating organisms will cause peritonitis.
To simulate contamination, 40 mL of a standardised inoculum (1×107 colony-forming units (CFU) per millilitre) of test organisms was sprayed while test participants made connections.
To specifically assess resistance to contamination, the inoculum was sprayed when the used disconnect caps in both systems had been removed and the catheter extension sets were open. After test organisms had been sprayed, participants then allowed dialysis fluid to flow from the fluid bag, through the catheter extension sets, into the effluent sample bags. The sample bags were then disconnected from the system for microbiology evaluation and the process repeated for all tests. IOY and TV validated this experimental method with a prior study of 14 tests.
Sample size, test participants and test sequence
According to Virzi, 80% of all usability issues are detected with at least four participants for a minimum sample size of 4.27 Four non-patient adults were recruited with fully informed consents to perform the experiment. Non-patient participants were preferred because of their similarity to new PD patients. The participants received training about PD and the use of both systems. They were allowed to practice till they felt comfortable using both systems as will be necessary for the experiment.
For each participant, test sequence for both touchless connector system and the standard of care included seven samples obtained as follows:
Sample 1: a sterile control before exposure to test organisms.
Samples 2–6: while the 40 mLs of test organisms are sprayed.
Sample 7: a contaminated control in which 100 mL of the standardised inoculum deposited in 2 L of dialysis fluid is allowed to flow through the fluid path of the connection systems.
To minimise bias, tests were alternated between both systems for each participant.
Microbiology
PA ATCC39327 and SE ATCC1228 were purchased from Microbiologix (St. Cloud, Minnesota, USA) and were routinely cultured and maintained on Luria Bertani (LB) agar. Strains were cultured overnight in LB medium (6×5 mL cultures of each bacterium).
Overnight cultures were combined and centrifuged at 7000× g for 10 min at 4°C. Cell pellets were washed once in 30 mL of sterile phosphate-buffered saline (PBS) followed by another centrifugation at 7000× g for 10 min. Samples were then combined (PA+SE) and resuspended in 600 mL of sterile PBS to a final OD600 of 0.1, corresponding to ~1× 107 to 1×108 cells of each organism. Final bacterial suspensions were prepared <30 min prior to transfer to the University of Minnesota Bio-Nano Lab for the experiments.
On delivery of sample bags after the experiments, they were immediately placed in a 37°C incubator to mimic human body temperature. The sample bags were stored in the incubator for 16 hours prior to analysis.
For the analysis, 200 μL of dialysis fluid was removed from each sample and placed in a 96-well microtitre plate. Serial dilutions of each sample were performed (10−1 to 10−8) by adding 20 μL of the sample into 180 μL of sterile PBS; 10 μL of each serial dilution were plated on LB agar (for total bacterial enumeration), Mannitol Salts Agar (for Staphylococcus enumeration) and Pseudomonas isolation agar (for Pseudomonas enumeration). Plates were incubated at 37°C overnight, and colonies were counted the next day.
Patient and public involvement
Patients and other stakeholders were involved in the iterative design of the touchless connector system but were not involved in the design of the proof-of-concept evaluation.
Results
Participants were between ages 31 and 56 years, with training time ranging from 5 to 13 min (table 2). None had previous PD experience and they all completed required tests for both systems.
For the microbiology test results, sterile and contaminated controls (samples 1 and 7) for both systems returned expected results, that is, observed bacterial growths on plates cultured from contaminated controls (sample 7) and no observable growths on plates from sterile controls (sample 1). Enumeration for remaining tests is shown in table 3.
Results of microbiology enumeration for test samples
Discussion
Cultures of samples from the touchless connector system showed no bacterial growth in the relevant connection attempts (ie, samples 2–6 for all 4 participants).
In comparison, cultures of samples derived from the standard of care showed bacterial growth. LB agar for total organisms showed bacterial growth in 13 of 20 (65%) relevant samples (figure 5). Mannitol Salts Agar, for SE showed bacterial growth in 15 of 20 (75%) relevant samples and Pseudomonas isolation agar for PA showed bacterial growth in 14 of 20 (70%) relevant samples.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Contamination on Luria Bertani Agar. CFU, colony-forming units.
Conclusion
Results show that the touchless connector system prevents fluid path contamination even with heavy bacterial exposures and may help reduce PD-associated peritonitis risks from inadvertent contamination with further development.
Ethics statements
Patient consent for publication
Ethics approval
Appropriate ethical and biosafety clearance was obtained from the University of Minnesota Institutional Review Board and Biosafety Committee, respectively (IRB ID: STUDY00010459). Participants gave informed consent to participate in the study before taking part.
Acknowledgments
The authors would like to recognise the contributions of Amy Hoelscher, Kieran Leong and Yasheen Brijlal to the early concept prototypes. The authors would also like to thank Heather Collier and the Fairview Kidney Center for providing essential feedback and assistance.
References
Footnotes
Twitter @ioyekinni
Contributors IOY drafted the work and this was then revised critically by all authors. The experiments were conducted by IOY and TV with the microbiology cultures developed by RH. All authors contributed to the conception and design of the work. All authors had final approval of the version to be published and are jointly accountable for all aspects of the work.
Funding Research reported in this publication was supported by the National Institute of Diabetes and Digestive and Kidney Diseases of the National Institutes of Health (Award Number: DK126586); National Science Foundation Division of Industrial Innovation and Partnership (Award Number: 1935233); National Institutes of Health’s National Center for Advancing Translational Sciences (Grant UL1TR002494). Additional support was provided by The Pediatric Device Innovation Consortium at the University of Minnesota. IOY was funded through the Bakken Medical Devices Center Innovation Fellowship Program.
Disclaimer The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health or the National Science Foundation.
Competing interests IOY, AT and TV invented the touchless connector. TV is an employee of Cerovations, a company that has licensed the connector from the University of Minnesota for commercialisation.
Provenance and peer review Not commissioned; externally peer reviewed.