Article Text

Abstract
Objectives Horizon scanning methodologies are employed in healthcare to identify and prioritise innovations at the early stages of development processes. To date, horizon scanning has been predominantly applied to early awareness systems of health technologies to facilitate healthcare planning. Still, horizon scanning methodologies may also be relevant for identifying novel healthcare delivery models and interventions. This study aimed to examine perceptions of determinants for adopting horizon scanning in the context of the development of integrated care models.
Methods Qualitative semistructured interviews were conducted between March and May 2021. The interviewees (n=10) were participants in innovation projects in the South-Eastern Norway Regional Health Authority. Data were analysed thematically with the aid of a predefined framework adapted from behavioural change theory.
Results Determinants of adopting horizon scanning were reported at the individual, organisational and wider institutional levels. Seven domains were perceived to enable or hinder stakeholders’ potential use of horizon scanning: knowledge of structured reviews, skills to perform horizon scanning, beliefs about consequences (validity and reliability of information, outcomes of filtering and priority setting, stakeholder involvement), beliefs about capabilities (technical skills, knowledge of roles and professional identities, organisational regulations), emotions (positivity, engagement, change fatigue), organisational resources (professional library, time, management support), context (complexity of ‘integrated care’, professional hierarchies, legal and political regulations).
Conclusions This study provides novel insights into potential determinants for adopting horizon scanning to identify, assess and prioritise innovative integrated care models. The findings may assist organisations considering using horizon scanning and inform strategies to mitigate barriers and promote facilitators.
- delivery of health care
- health services research
- behavior and behavior mechanisms
- policy
Data availability statement
Data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Summary box
What are the new findings?
Horizon scanning methodologies can be useful for identifying, assessing and prioritising innovations in healthcare delivery models at an early stage.
We identified determinants to the adoption of horizon scanning in the context of health services delivery innovation as perceived by stakeholders
How might it impact on healthcare in the future?
This study may inform organisations considering using horizon scanning to identify novel health services models and contribute to developing interventions that target potential barriers and promote facilitators.
Introduction
It is widely believed that developing and implementing novel products, services and processes in the healthcare sector has the potential to improve population health and promote a more efficient use of resources. Healthcare organisations worldwide strive to improve their healthcare delivery models.1 To manage the rapid emergence of innovations and to promote promising technological development, horizon scanning methodologies are increasingly employed in the healthcare and biomedical fields and, in particular, in early awareness systems of health technologies such as pharmaceuticals and medical devices.2 3 Horizon scanning follows a standardised stepwise process to yield a systematic detection and assessment of early signs of important developments, assessing their potential impact and, in this way, prioritising resources and investment in innovation. Thus, horizon scanning holds promise for informing and preparing decision-makers for change.
However, less attention has been given to the application of horizon scanning for identifying innovative healthcare delivery models, for example, integrated care models. Alerting policy-makers and other stakeholders to emerging issues and providing options for the development of integrated care may be challenging due to the lack of common definitions and conceptual frameworks of integrated care, the complexity and intersectional nature of integrated care and the variety of perspectives stemming from various stakeholders in the health system. Nonetheless, horizon scanning offers a structured approach to addressing weak signals of future trends and may aid innovation in healthcare delivery. Adopting horizon scanning for the purpose of detecting early signals of innovation in the context of integrated care delivery models may potentially be informative and useful. However, its value depends not only on the efficacy of the methodologies of scanning they provide but also on their acceptance and uptake by stakeholders.
The aim of this study was to explore potential enabling and constraining factors for the use of horizon scanning methodologies in the early phases of identifying innovative integrated care delivery models, as perceived by healthcare personnel with experience in project development. To aid the analysis, we utilised a theory-based behaviour change framework, the Capability, Opportunity and Motivation model of Behaviour (COM-B) and the Theoretical Domains Framework (TDF).
Scanning the horizon for novel integrated care models
There is no common definition of integrated care.4 ‘Integrated care’ is used to denote both the process by which professionals and organisations become integrated and the outcome experienced by service users, such as patients and carers. The WHO (Europe) has offered a system-based understanding of integrated care:
(Integrated care is) an approach to strengthen people-centred health systems through the promotion of comprehensive delivery of quality services across the life-course, designed according to the multidimensional needs of the population and the individual and delivered by a coordinated multidisciplinary team of providers working across settings and levels of care.4
This understanding encompasses different types of integration (organisational, functional, service, and clinical, table 1), as well as the horizontal and vertical dimension of integration, and the breadth and levels at which integration may be pursued. We follow this multifaceted definition of integrated care in this paper.5–7
Typologies of integration, adapted from Lewis et al 5
Horizon scanning is a systematic approach for detecting early signals of potentially important developments, opportunities and threats that could impact areas of interest.8 Although there is not yet a standardised terminology regarding methodologies, tools, techniques and processes involved in horizon scanning, it generally follows a six-step approach of signal detection, filtration, prioritisation, assessment, dissemination and updating information (figure 1). Horizon scanning often begins with mapping signals of innovation with the use of various sources for information and techniques to search for signals of potential value. Preset filtration and prioritisation criteria are used to discard irrelevant signals. Assessment methods include the participation of experts, users and policy-makers and peer reviews. The results of the horizon scanning are then disseminated and evaluated.2

Common stages of horizon scanning from the Euroscan network (Euroscan). This figure is licensed under the creative commons Attribution-NonCommercial-ShareAlike 4.0 international licence (CC BT-NC-SA 4.0).
Horizon scanning should be differentiated from foresight.9 A foresight process may be understood broadly to address the full cycle of policy on ‘complex futures’, involving a range of stakeholders, long-term considerations and different scenarios. It is a rather comprehensive set of activities which includes a horizon scanning phase at the beginning of the process. Thus, compared with foresight, horizon scanning has a narrower scope, a shorter time horizon and a more specific thematic focus. Moreover, horizon scanning can be a stand-alone approach for identifying ‘things to come’.
Neither should horizon scanning be regarded as a systematic literature review. Signals of ‘things to come’ are detected from manifold information sources in addition to, or even instead of, reviews of scientific literature. These sources include targeted literature searches and input from expert groups, committees, surveys, government bodies, conferences, associations, media and more.2 Thus, horizon scanning can lack a clear weighting of evidence and should not be misinterpreted to give an exhaustive summary of current evidence. The aim of horizon scanning is rather to inform decision-makers about signs of innovation at an early stage, at which point available information is limited.
Furthermore, experts and other stakeholders with diverse views, experiences and roles may be brought together to systematically discuss signals as part of the horizon scanning process. The aim can be to build consensus on emerging issues and to assess signals. Stakeholder participation is often organised as workshops, focus group activities or variations of Delphi studies in which relevant issues are ranked, discussed and reranked. Methods and criteria used for assessment vary. Nonetheless, expert consensus is thought to add weight to horizon scanning conclusions.2
Methods
This study used a prospective theory-driven qualitative design. The study was regarded as health services research. Data management and protection was notified to the Norwegian Centre for Research Data (NSD; project number 967152). It was reported according to the Consolidated Criteria for Reporting Qualitative Research.
Setting
The Norwegian healthcare system is universal, tax-financed and semidecentralised.10 The responsibility for primary care lies with the municipalities. The central state is responsible for secondary and specialist care, which is administrated by four Regional Health Authorities (RHAs). The South-Eastern Norway RHA is the largest RHA and provides care to approximately three million people living in 44 municipalities.
Participants and recruitment
Purposive sampling11 was employed as we wanted participants with knowledge and insights into how to develop integrated care innovation projects. The research team established contact with the project management of two ongoing innovation projects carried out in the South-Eastern Norway RHA. The projects aimed to develop integrated care delivery models to meet the complex needs of (1) children and youth at risk of developing mental health problems and (2) multimorbid and older people with frailty. We asked the project management to inform the staff about our study. The first author (MNW-S) sent a formal invitation by email to all 16 participants in the two innovation projects.
Data collection
Individual qualitative interviews were conducted from March to May 2021. Participants received written information about the study and signed a consent form before the interviews were undertaken. Participants were given the opportunity to review the illustrative quotes from their interviews.
A semistructured interview guide was developed covering questions about their experiences with prior innovation projects and beliefs about horizon scanning (see online supplemental file 1) for a description of the guide). Horizon scanning was presented with a flowchart, and the interviewer (MNW-S) presented the different steps (as illustrated in figure 1) in detail. Two pilot interviews were carried out, and the interview guide was slightly amended according to feedback.12
Supplemental material
Interviews were conducted face-to-face and digitally. Interviews lasted from 50 to 60 min. All interviews were conducted by MNW-S in Norwegian and audiorecorded. Field notes were taken during the interviews. The interview transcripts were de-identified. All data were stored on a password-protected computer connected to a university server.
After eight interviews, information began to be repetitive. Two more interviews were carried out and we concluded that there was no need to recruit more participants for the study. We assessed saturation to be achieved after 10 interviews. No additional information was produced by new incoming data.13
Data analysis
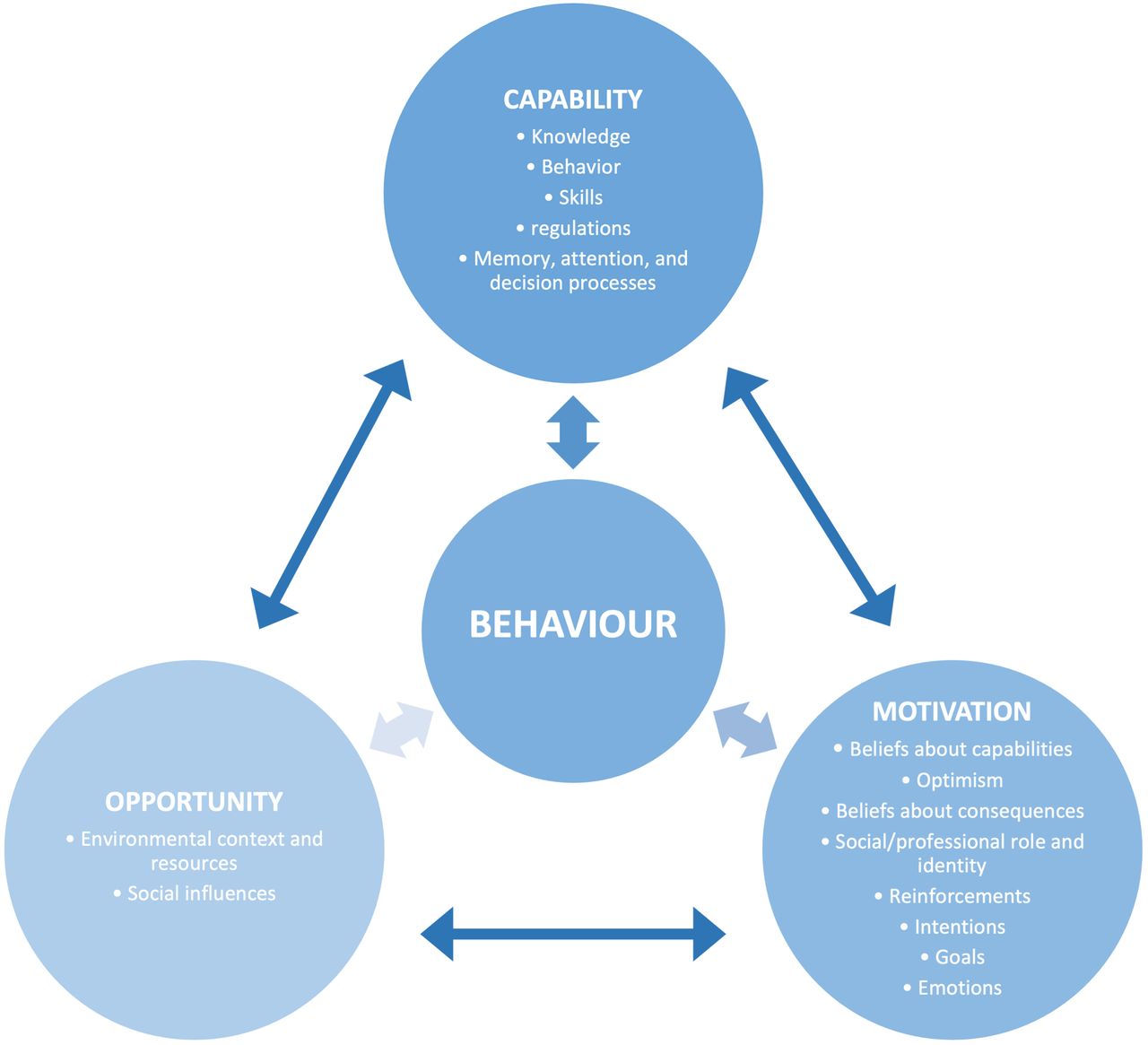
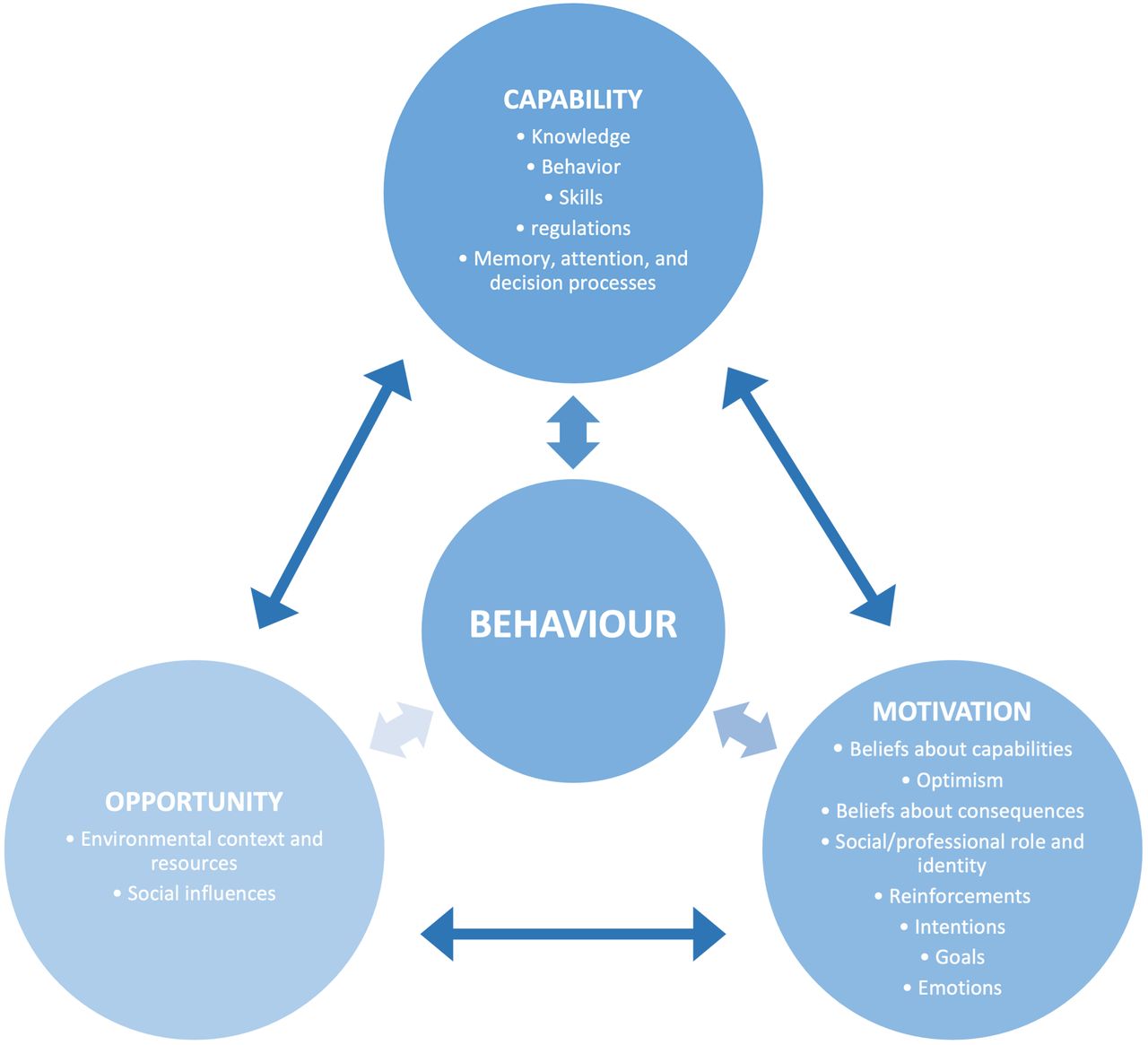
To aid analysis, the COM-B was used. The model hypothesises that three key components interact to shape behaviour, including individual capability and motivation and the social and contextual opportunities that prompt behaviour.14 The three components may be further specified with the aid of the TDF, which is a simplification of a range of theories into 14 domains underpinned by psychological theory.14 15 These domains include individual-level factors, such as knowledge and skills, beliefs about consequences and capabilities, intentions and emotions, and contextual and resource factors, such as time constraints and organisational and legal regulations. We used this combined COM-B/TDF approach to map responses onto the categories of the predefined framework (figure 2).
{kind=link}
{kind=link}
COM-B/TDF. Determinants through COM-B elements and TDF domains (adapted from Michie et al and Atkins et al).14 15 The arrows illustrate the potential impacts of the components on each other. COM-B, Capability, Opportunity and Motivation model of Behaviour; TDF, Theoretical Domains Framework.
Data were analysed thematically, following a stepwise approach described by Braun and Clarke16 (reading, coding, collecting codes, reviewing and refining analysis, reporting). Data were transcribed and coded with the aid of NVivo V.12.
First, we coded and organised data according to the COM-B model. Then, fragments of the text were categorised and then recategorised into subthemes that were deemed relevant to the study according to the TDF. MNW-S did the first round of coding; all the authors were involved in subsequent refinement of coding and organising of data. In cases of discrepancies in interpretation, these were discussed among the authors until agreement was reached. Quotes used for illustration were translated from Norwegian to English by the authors.
Results
Out of the 16 persons invited to participate in the study, 10 were included in the study (1 declined the invitation and 5 did not reply). Eight of the participants were females, and two were males. The participants had different educational backgrounds (including medicine, physiotherapy and psychology) and various roles in the health and social care sector at both specialist and primary care levels (including managers, advisors, coordinators, hospital doctors, GPs, psychologists and physiotherapists).
Barriers and facilitators
Determinants to adopting horizon scanning methodologies in the early phases of detecting novel integrated care models were identified at the individual, organisational and wider contextual levels (ie, factors embedded in the broader healthcare system). Following the combined COM-B and TDF framework, the determinants are reported under the headings Individual capabilities, Organisational and contextual opportunities and Individual motivation and further categorised under relevant TDF domains. Table 2 provides an overview of the results, with illustrative quotes for each domain.
Factors perceived to determine adoption of horizon scanning methodologies
Individual capabilities
Knowledge of literature reviews and structured frameworks
The participants reported knowledge of literature reviews and structured frameworks as a determinant for perceived acceptance among project participants and organisation management, of endorsing the use of horizon scanning. Participants with prior experience in research could draw parallels between horizon scanning and literature review methodologies and comment on similarities and differences. Knowledge of scientific methods was seen as a facilitator to the potential use of horizon scanning.
Skills to perform horizon scanning
None of the participants was familiar with horizon scanning. Participants with knowledge of different approaches to literature reviews reported lack of skills for successfully carrying out necessary searches to identify and filtrate relevant literature. This was perceived to be a barrier to the adoption of horizon scanning.
Organisational and contextual opportunities
Organisational resources
A major theme, and the most frequent factor mentioned by the participants, was time constraints. Participants described the daily work as hectic and demanding, and there were concerns about spending too much time on planning and conducting horizon scanning. Participants believed that lack of management support for spending time on project participation was a potential barrier.
Skills-based education and training in horizon scanning methodologies was perceived as an organisational responsibility. The participants reported that management support in increasing knowledge, awareness and engagement was necessary to enable the use of horizon scanning. Moreover, the involvement of professional librarians was seen as a facilitating factor.
Complexity of ‘integrated care’
Some of the participants identified the lack of a common definition of integrated care as a barrier. They mentioned how different stakeholders, such as healthcare professionals, service users, managers, health authorities and policy-makers, had different expectations and views of the definition of integrative care models, which potentially may hinder the horizon scanning process.
Professional hierarchies
Some participants further discussed how organisational culture and professional hierarchies would influence discussions at various steps in the horizon scanning process. They worried that specialist healthcare would dominate discussions and perceived this as a barrier.
Organisational and regulative context
The participants worried that the different organisational, legal and political regulations regarding primary and specialist care were a potential barrier. Horizon scanning, aiming at identifying promising models from different countries, with different healthcare systems, may yield results that are not easily translatable to the present context. Furthermore, the different regulatory contexts of primary and specialist care in the Norwegian healthcare system were perceived to be a potential barrier.
Individual motivation
Beliefs about consequences of using a horizon scanning framework
The participants identified various consequences as determinants. The systematic and structured approach characterising horizon scanning was perceived to be both a facilitator and a barrier to its use. On the one hand, the stepwise process of horizon scanning was reported to potentially enable better information, more targeted discussions about goals, priorities, limitations and opportunities, and inclusion of relevant stakeholders at different stages of the process. On the other hand, questions were raised about employing predetermined criteria such as the potential cost–utility ratio at the filtration stage, and further, using too strict criteria to prioritise and assess novel care models. Furthermore, concerns about disagreement on criteria and methods within horizon scanning were expressed, as different stakeholders’ preferences could lead to spending too much time agreeing on and planning the stages of horizon scanning.
Beliefs about capabilities to undertake horizon scanning
Several participants perceived the lack of skills among healthcare professionals in employing horizon scanning to be a potential barrier. This included lack of technical skills, such as familiarity with systematic literature search. Furthermore, the lack of knowledge about the different organisational structures at the primary and specialist healthcare levels and the lack of understanding of the different professional roles, knowledge bases, and professional terminology of stakeholders, were seen as barriers to use. Knowledgeable and committed professionals could act as facilitators.
Emotions
Participants believed that a positive culture of engagement among stakeholders would facilitate the use of horizon scanning. However, several participants reported that there was a kind of ‘change fatigue’ in the organisation and that people were tired of participating in new projects. There was some hesitation about using new methods due to previous experience in other projects. Questions were raised as to whether horizon scanning would lead to improved results, and whether putting in the effort to use horizon scanning made any difference compared with the current processes.
Discussion
To the best of our knowledge, this is the first study of how stakeholders with experience in healthcare innovation projects perceive barriers to and facilitators of using horizon scanning methodologies to identify, prioritise and assess novel integrated care delivery models.
We used the COM-B model, which hypothesises an interactive relationship between three components; individual capability and organisational and contextual opportunity can influence individual motivation, while behaviour can alter capability, motivation and opportunity. For example, participants who had prior knowledge of research methods (capability (knowledge)), and had experience with literature reviews were more assertive of the perception that horizon scanning would yield favourable outcomes to innovation projects (motivation (beliefs about consequences)). Furthermore, these participants were less confident in their capabilities to perform horizon scanning themselves (motivation (beliefs about capabilities)). Participants who discussed professional hierarchies (opportunity (environmental context)) as a contextual barrier to using horizon scanning were more prone to the view that knowledge of different stakeholders’ roles, knowledge bases and professional terminology (capability (knowledge)) would enable horizon scanning. Complexity of integrated care (opportunity (environmental context)) related to discussions of ‘change fatigue’ (motivation (emotions)), while time constraints (opportunity (organisational resources)) were mediated by motivation through optimism and engagement (motivation (emotions)).
Identification of new healthcare delivery models in the context of integrated care is particularly challenging due to the lack of common definitions and conceptual frameworks. Furthermore, multiple stakeholders including health and social care professionals with different roles and professional identities, researchers, managers, health and social care authorities, patients and service users, may have different views about local needs and about which dimensions of integrated care are most important, which processes should be prioritised and which care models should be developed.
Stakeholder inputs are critical to the success of the horizon scanning process.17 Moreover, by including different perspectives as a part of the horizon scanning framework, one can potentially detect trends and connect real needs to the development of new service models.
In previous horizon scans, workshops have proven important for finding core issues, initiating the process of refining questions, sharing perspectives, and building trust and understanding.18 They can also provide a sense of ownership in the questions discussed.18 This study identified how participants were apprehensive about the experience they had had with other projects, including that different stakeholders had had different preferences regarding choices of service delivery models. Furthermore, professional hierarchies were seen as a potential barrier to horizon scanning, as influential and dominating stakeholders may use their authority to make decisions about criteria for identification, filtration, prioritisation and assessment. How to avoid such unintended consequences should be studied in future research.
Limitations
This study was small, and the findings may not be easily transferable to other settings. However, replication may be facilitated by this study’s use of the systematic and theoretical basis for identifying potential determinants for acceptance and uptake among stakeholders. The use of a predetermined framework is at the same time a possible limitation, as we may have overlooked data that did not fit the pre-defined framework. This is a limitation inherent to deductive (concept-driven) thematic coding.
In horizon scanning of novel integrated care models, one major task is the definition of keywords and terminology to use for signal detection. We realise that ‘integrated care’ may take many forms and that the term may be understood to involve different types of integration. For example, the concepts of service integration and clinical integration should be carefully defined to avoid a potential overlap. We cannot disregard the fact that the participants in this study may have understood the term ‘integrated care’ in different ways, which may have affected their views.
Conclusion
We investigated stakeholders’ perceptions of the potential use of horizon scanning methodologies to detect innovative integrated care models by using a theoretically informed behavioural approach, combining the COM-B and the TDF. The findings of this study might aid the development of interventions targeting barriers and promote enablers to adopt horizon scanning for identifying and assessing novel healthcare delivery models. Further studies should explore behaviour change techniques that would be suitable for addressing the determinants identified for the introduction of horizon scanning as a tool in complex processes and the piloting of horizon scanning for emerging integrated care models.
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study was approved by in accordance with Norwegian regulations, this study was regarded as health services research. It is therefore assessed and approved by Norwegian Centre for Research Data (NSD). Project ID number 967152.
Acknowledgments
We would like to thank the participants. We would also like to thank the Norwegian Centre for Health Services Research (NORCHER) for contributing to this research.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors All authors contributed to the conception and design of this work. MNW-S was responsible for the acquisition of data under the supervision of GT. MNW-S, GT and EF contributed to the analysis and interpretation of the data, the drafting and revising of the paper for intellectual content, and final approval of the version to be published. MNW-S, GT and EF have all agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding Financial contribution from the Research Council of Norway through the Norwegian Centre for Health Services Research (NORCHER project number 296114) is acknowledged.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.