Article Text

Statistics from Altmetric.com
Summary box
What are the new findings?
Conventional remote monitoring systems for critically ill patients are expensive.
We propose a conceptual prototype of low-cost wearable remote monitoring for resource-restricted settings capable of real-time signal capture and quality control.
We describe piloting this system for monitoring of patients with COVID-19 in a field hospital in Vietnam.
How might it impact on healthcare in the future?
This prototype could provide a flexible and scalable solution for remote patient monitoring in resource-limited settings, with the potential for improved patient care, staff time and healthcare resource utilisation.
By gathering real-time continuous monitoring data, our system could use advanced analytics and personalised clinical decision support systems.
Introduction
As of 24 February 2021, the Vietnam Ministry of Health has reported 2412 cases of COVID-19.1 The country’s meticulous contact tracing strategy, mass testing and strict quarantine require all confirmed cases and first-degree contacts to be isolated and carefully monitored in dedicated facilities for at least 14 days. Additional monitoring of cases occurs until resolution of symptoms and three consecutive negative reverse transcription PCR tests.2 Even for mild cases (those without oxygen requirement) and first-degree contacts, trained medical staff wearing personal protective equipment (PPE) perform monitoring two times per day.
Many quarantine facilities are rural local hospitals or military camps where there was hitherto only limited medical monitoring capacity. Therefore, even in a country with limited COVID-19 cases, the required control measures continue to place a great burden on the country’s healthcare system.
Throughout the world, there is an unprecedented demand for equipment and staff to monitor patients with COVID-19. To eliminate unnecessary patient contact and reduce the burden on facilities and staff, the Food and Drug Administration in the USA has relaxed regulations concerning remote non-invasive monitoring devices, increasing the potential of technological solutions.3 In the UK, non-invasive pulse photoplethysmography (PPG) has been used for self-monitoring oxygen saturation (SpO2) in cases of mild disease or following hospital discharge.4 In the Netherlands, an automated remote monitoring system with non-invasive multisensor patches was piloted in hospitalised patients.5 Patients were randomised to normal practice or remote monitoring where vital sign data were transmitted every 2 min to a central system. Subsequent patient room visits by nursing staff were monitored, and although specific monitoring visits were reduced, overall visits were not, nor was the amount of PPE used. Reports of remote monitoring applications in low-income and middle-income country (LMIC) settings are very few. One system piloted in Sierra Leone in the 2014 Ebola outbreak showed proof of principle that a multisensor patch could transmit continuous real-time patient data to a central monitoring facility6; however, the cost associated with these units remained significant.
Since 2014, technological advances have meant that sensor systems are cheaper and of better quality. Algorithms from PPG sensors can measure heart rate, SpO2, respiratory rate and cardiovascular indices, reducing the reliance on more expensive and complex monitors and therefore applicable to resource-limited/rural settings.7–9 In this report we describe the initial piloting of a lightweight, non-invasive, conceptual prototype consisting of a medical-grade wearable PPG sensor, mobile device and screen mirror application, used to remotely monitor and access key continuous vital sign data in patients with COVID-19.
Methods
The study was carried out at the Cu Chi Field Hospital in Southern Vietnam, within the context of a larger observational study in which patient vital signs and laboratory data are collected prospectively in symptomatic and asymptomatic cases testing positive for SARS-CoV-2. Figure 1 illustrates the proposed standard operating procedure for remote wearable monitoring this study piloted. The cases described here were without severe symptoms and able to carry out the self-monitoring arm of the standard operating procedure. All participants gave written informed consent prior to enrolment in the study.
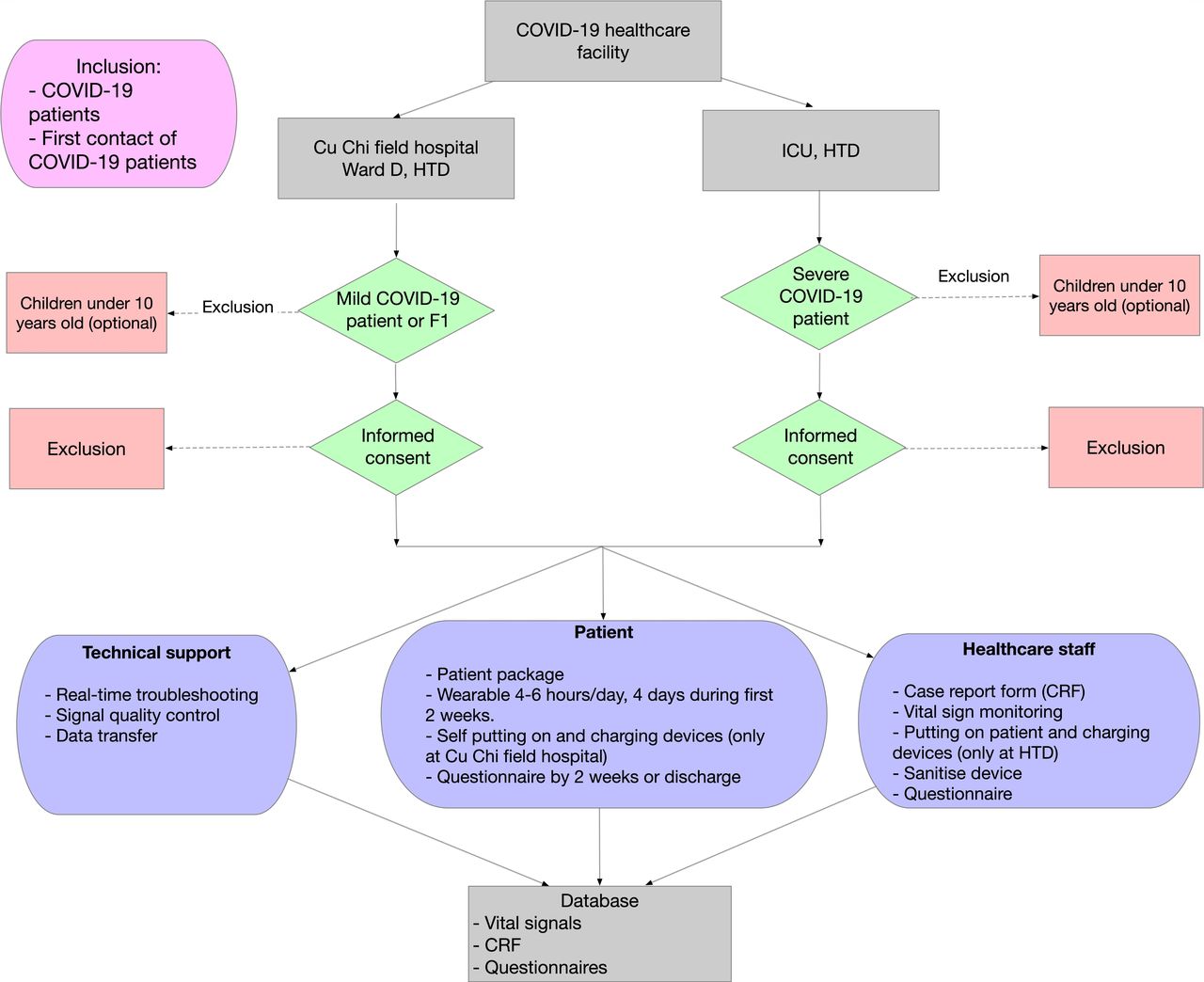
Standard operating procedure for wearable monitoring at the Hospital for Tropical Diseases (HTD) and Cu Chi Field Hospital. ICU, intensive care unit.
The prototype is composed of a low-cost wearable, a Bluetooth-enabled mobile device and a mirror screen application. The wearable is a medical-grade, wrist-worn, fingertip pulse oximeter able to deliver signals to a mobile device in real-time via Bluetooth (figure 2). The mobile device could be either smartphone or tablet, in which discrete applications are installed for signal receipt, analysis and screen mirroring. In this study we used a SmartCare wearable (SmartCare Analytics, London, UK) to transmit anonymised PPG data to a mobile phone (Android V.8.x or V.9.x with 3G/4G connectivity) using AirDroid screen mirror application (https://www.airdroid.com).

{kind=link}
{kind=link}
Wearable pulse oximeter device and smartphone display used for remote monitoring.
Enrolled patients were supplied with a patient package containing the pulse oximeter smartphone, charging cables and a user guide. These packages remained with the participant for the duration of their hospitalisation. Following brief training, patients were able to attach the pulse oximeter to perform continuous PPG measurement for 2–3 hours, up to four times during their first 2 weeks of hospitalisation. Support was provided through mobile phone communication. For infection control, we use a single-use wristband and kept the mobile device in a sealed bag. Sanitation of chargers and wearables followed standard medical device decontamination procedures advised by the Vietnamese Ministry of Health.2
PPG signals were visualised on a daily basis to confirm satisfactory waveform morphology and allow timely feedback to healthcare staff. Recorded PPG signals were then evaluated for signal loss and signal quality indices. Signal loss was defined as the percentage of signal recording with value of either 0 or with value unchanged for more than 300 ms. Frequency trimming based on Welch’s method was applied to remove sections with abnormal frequencies. The remaining data were then split into 5 min segments. Four standard signal quality indexes were calculated for each 5 min segment, using Python scipy and statsmodels libraries.10 Selected indices were kurtosis (an indication of ‘tailness’ of distribution), skewness (a measure of symmetry), entropy (a measure of uncertainty/randomness of the signal) and signal to noise ratio (SD of filtered to unfiltered signal). Segments where more than two of these indices fell into the 0.1 or 0.9 quantiles of the whole recording distribution were classified as ‘non-acceptable’.
Results
We successfully implemented the new monitoring procedure at Cu Chi Field Hospital, necessitating only minimal staff training and short time for the application installation. The monitoring system was piloted in two patients recruited between 2 and 5 February 2021. In total, 8.63 hours of PPG were obtained, of which there was approximately 33% signal loss. Signal quality indices calculated from the remaining segments are shown in table 1, where 94% of segments were classified as acceptable.
Signal quality indices of two patients’ recordings
Nursing and medical staff feedback was positive, with very few reporting difficulties in carrying out the monitoring scheduled. Preliminary patient feedback was also encouraging, in terms of comfort, perceived benefits and engagement in self-monitoring. Importantly, patients reported feeling less isolated and less anxious.
Discussion
We present preliminary data showing the feasibility of a remote monitoring prototype tailored for low-resource settings, piloted in a Vietnamese COVID-19 healthcare facility. Commercial centralised patient remote monitoring systems, such as those used in intensive care units, are costly in terms of both initial installation and ongoing maintenance and few incorporate wearable sensors. Those allowing real-time access to raw data are scarce and prohibitively expensive for large-scale use in resource-limited settings. By separating wearables from the central monitoring platform, the system we propose offers increased flexibility at lower cost. Different wearables can be used and ‘smart’ features such as signal dashboards and early identification of signal change can be computed in situ by another mobile application. As a result, development of the different components can be independent and exploit open-source solutions.
Similar to previous studies using wearable devices for clinical monitoring, we found appreciable amounts of data were lost.11 12 While we did not aim to establish reasons for this, they may include movement artefact, sensor quality and other factors related to real-life operating conditions in LMIC hospitals. Nevertheless, evaluation of the remaining data showed almost all segments were classified as having acceptable signal quality.
Although our pilot was performed in a field hospital setting, we experienced little difficulty in implementation. In the absence of reliable WiFi, a standard mobile internet plan of 100 Mb/day was sufficient to transfer 4–6 hours of 100 Hz PPG recordings. While we transferred only anonymised PPG waveform, it would be possible to encrypt and compress data prior to transferring. To manage a number of mobile devices simultaneously, multidevice screen mirroring subscription packages are available at US$100 per 10 devices per year. Ultimately, the technical support we provided in this study could be easily performed by non-medical staff, further increasing flexibility.
We have herein presented initial feasibility data of our prototype system. Our ongoing and future work will continue to evaluate our system in a larger sample of patients with COVID-19 with differing severities across other hospital sites in Vietnam and Indonesia, where we will further evaluate signal quality analytics and user acceptability. Ultimately we aim to assess other vital sign metrics, using data to develop artificial intelligence (AI)-assisted analytic and diagnostic tools for COVID-19 infection.
In conclusion, we have demonstrated that low-cost wearable systems and remote monitoring can be successfully implemented in an outbreak setting in a COVID-19 Vietnamese field hospital, with the over-riding aim of improving patient management and facilitating more efficient use of overburdened staff and healthcare resources.
Ethics statements
Ethics approval
The study was approved by the Scientific and Ethical Committee of the Hospital for Tropical Diseases and the Oxford Tropical Ethics Committee.
Acknowledgments
We thank the staff and patients at Cu Chi Field Hospital.
Footnotes
NVVC and HBH are joint first authors.
DC, SY and CLT are joint senior authors.
Twitter @phan189, @Le_Van_Tan
Collaborators OUCRU COVID-19 Research Group: Hospital for Tropical Diseases, Ho Chi Minh City, Vietnam (in alphabetical order): Nguyen Van Vinh Chau, Nguyen Thanh Dung, Le Thi Dung, Nguyen Van Hao, Le Manh Hung, Nguyen Phu Huong Lan, Huynh Thi Loan, Dinh Nguyen Huy Man, Nghiem My Ngoc, Huynh Kim Nhung, Phan Minh Phuong, Nguyen Thanh Phong, Tran Thi Lan Phuong, Ngo Tan Tai, Tran Thi Thanh Tam, Pham Ngoc Phuong Thao, Tran Nguyen Phuong Thao, Nguyen Ngoc Thao, Ho Thi Thu Thao, Bui Thi Ton That, Pham Thi Ngoc Thoa, Nguyen Thi My Tien, Tran Nguyen Hoang Tu, Duong Bich Thuy, Huynh Trung Trieu, Nguyen Thanh Truong, Dinh Thi Bich Ty, Thai Lam Uyen, Le Thi Tam Uyen, Huynh Ngoc Thien Vuong, Vo Trong Vuong. Oxford University Clinical Research Unit, Ho Chi Minh City, Vietnam (in alphabetical order): Hai Ho Bich, Mary Chambers, Ho Quang Chanh, Marc Choisy, Jeremy Day, Joseph Donovan, H. Rogier van Doorn, Nguyen Thi Phuong Dung, Ronald Geskus, Huynh Ngan Ha, Vu Thi Ty Hang, Tran Tinh Hien, Ngo Thi Hoa, Nguyen Thi Thu Hong, Evelyne Kestelyn, Huynh Le Anh Huy, Phan Nguyen Quoc Khanh, Thomas Kesteman, Le Dinh Van Khoa, Katrina Lawson, Lam Anh Nguyet, Le Thanh Hoang Nhat, Phung Tran Huy Nhat, Nguyen Thanh Thuy Nhien, Le Nguyen Truc Nhu, Nguyen Thi Han Ny, Sonia Lewycka Odette, Maia Rabaa, Motiur Rahman, Jennifer Van Nuil, Hoang Minh Tu Van, Dong Thi Hoai Tam, Le Van Tan, Tran Tan Thanh, Nguyen Thuy Thuong Thuong, Guy Thwaites, C Louise Thwaites, Nguyen Xuan Truong, Nguyen Thi Kim Tuyen, Sophie Yacoub, Phung Le Kim Yen, Lam Minh Yen, Huynh Xuan Yen.
Contributors HBH, KPNQ, HG, SY, DC and CLT conceived the study. NVVC, HBH and KPNQ designed the study. NVVC, HBH, KPNQ, HTT, CNN, HMTV, LVT, LMY and NTD implemented the study. NVVC, CNN, LVT, NTD, DC, SY and CLT provided resources for the study. LDVK, HBH, CLT and HMTV analysed the data. HBH, HG, HMTV and CLT drafted the manuscript. All authors reviewed the manuscript.
Funding The study was funded by the University of Oxford COVID-19 Research Rapid Response Fund (ref 0009126). DC was supported by the National Institute for Health Research (NIHR) and the Oxford Biomedical Research Centre (BRC). LVT, CLT, HBH, HG, KPNQ, LDVK, HMTV, LMY and SY are supported by the Wellcome Trust (204904/Z/16/Z, 107367/Z/15/Z, 217650/Z/19/Z, 089276/B/09/7).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.