Article Text

Abstract
Purpose Hospital-level care provided at home improves patient outcomes, yet nearly all programmes function in urban environments. It remains unknown whether rural home hospital care can be feasibly delivered.
Methods Based on prior stakeholder learning and detailed landscape analyses of various rural areas across the country, we re-engineered the workflows, personnel and technology needed to respond to many of the challenges of delivering acute care in rural homes. We performed a preliminary ‘mock admission’ in a simulation laboratory with actor feedback, followed by mock admissions in rural homes in Utah of chronically ill patients who feigned acute illness. We employed rapid cycle feedback from clinicians, patients and their caregivers and qualitative analysis of participant feedback.
Findings Following rapid cycle feedback in the simulation laboratory and rural homes, mock admission, daily rounds and discharge were successfully conducted. Technology performed to laboratory-determined specifications but presented challenges. Patients noted significant comfort with and preference for rural home hospital care, while clinicians also preferred the model with the caveat that proper patient selection was paramount. Patients and clinicians perceived rural home hospital as safe. Clinicians noted rural home hospital workflows were feasible after streamlining remote and in-home roles.
Conclusions Rural home hospital care is technically feasible, well-received and desired. It requires testing with acutely ill adults in rural settings.
- delivery of health care
- hospital medicine
- health services research
Data availability statement
No data are available.
Statistics from Altmetric.com
Summary box
What are the new findings?
Illness that traditionally requires hospitalisation represents a common critical moment in nearly every person’s life. Rural home hospital is a disruptive care delivery model that adapts the urban home hospital principles by implementing innovative technologies, top-of-license personnel and novel workflows to deliver high-value acute rural care for rural patients, who face geographical, financial and cultural barriers to accessing acute care in traditional hospital settings.
Following rapid cycle feedback in the simulation laboratory and rural homes, mock admission, daily rounds and discharge were successfully conducted. Patient and clinicians perceived rural home hospital as safe, workflows as feasible and patients noted comfort and preference for rural home hospital care.
How might it impact on healthcare in the future?
We have designed appropriate training, scope of practice, and workflows for nurses, physicians, paramedics, and other healthcare professionals in this unique acute care at home setting. If successful, such a model would likely ameliorate issues surrounding access, safety, quality, experience and cost in rural areas and would entirely reimagine a decentralised acute care delivery model.
Learnings from this phase of the work will inform future iterations and testing of the rural home hospital model.
Introduction
For the 1 in 5 Americans living in rural areas, totalling nearly 60 million people, it can be challenging to receive hospital-level care.1 The hospital may be located miles away, emergency services may not be reliably available for transport, or care may not be accessible at all due to hospital closure.2–5 Even when a hospital is available, its use may be associated with significant adverse events, owing to the site of care.6–11
Many urban healthcare systems have chosen to adopt a home hospital model that provides hospital-level care at home as a substitute for the traditional hospital.12 13 Home hospital programmes typically provide a full suite of services that would normally be delivered in a hospital, including nurse and physician visits, intravenous medications, remote monitoring, video communication and point-of-care testing.13 Conditions treated include the most common reasons for internal medicine admission: infection, exacerbation of heart failure, asthma, and chronic obstructive pulmonary disease, and others. Randomised controlled trials14 15 and quasi-experimental evaluations16–18 have shown significant improvements in cost, 30-day readmission, physical activity and experience for patients hospitalised at home compared with a traditional hospital.
Despite the success of urban home hospital programmes, rural areas have rarely trialled this innovation. While some factors may make rural areas an ideal setting for a home hospital, including the provision of lower cost agile capacity, other factors have undoubtedly prevented home hospital, including travel burden and connectivity.
We recently described rural perceptions of home hospital care through a series of qualitative interviews and a focus group with rural clinicians and patients, demonstrating interest and perceived acceptability among clinicians and patients in rural America.19 We took key learnings from these stakeholders to iterate on the design requirements of how home hospital care might function in rural America. To prepare a plausible rural home hospital model, we tested our assumptions of the personnel, workflows and technologies required through simulated ‘mock admissions’ first in a lab setting and then in rural homes of chronically ill patients who feigned acute illness and had been hospitalised previously.
Methods
Study design, participants and data sources
Based on key learnings from stakeholders19 and detailed landscape analyses of various rural areas across the country (example in online supplemental), we re-engineered the workflows, personnel and technology needed to respond to many of the challenges of delivering acute care in rural homes. We then performed a preliminary mock admission in a simulation laboratory with actor feedback and study team observation to further iterate the model and test various designs.
Supplemental material
To test the feasibility of rural home hospital care in the intended setting, we subsequently performed mock admissions in regions of rural Utah. We defined rural as an area that falls within the following criteria: rural–urban commuting code (RUCA) 4–10, frontier and remote area code (FAR) less than or equal to 4 and Centers for Medicare & Medicaid Services ambulance fee schedule of ‘super rural’ (emergency medical services (EMS) super rural). We defined super rural as an area that falls within the following criteria: RUCA 10, FAR 4 and EMS super rural.
We recruited two patients from the University of Utah Health who lived in a private residence in rural Utah, had capacity to consent and had a chronic illness that had at least once prior resulted in an acute hospitalisation. We asked participants to feign an acute exacerbation of their chronic illness drawing from their lived experience with details added by the study team (cases in the online supplemental). We then deployed the home hospital model to the patient’s home in a simulated mock admission. The study team was present in the patient’s home to observe all interactions, noting in real-time strengths and areas of improvement with respect to workflow, personnel and technology. Using a rapid cycle feedback approach, the home hospital team ‘admitted’, ‘rounded on’ and ‘discharged’, each patient multiple times to allow for iterative improvement and learning. After each segment (admission, daily rounds and discharge) was completed, we asked all clinicians, the patient and their caregivers for formative feedback through a semistructured qualitative interview, focusing on what went well and what could be improved (interview guide in the online supplemental). If possible, we made recommended changes in the next iteration. We continued to repeat a segment until saturation (ie, repetitions of a segment ended when the study team felt another repetition would not yield further insights). The entire mock admission experience lasted a full day. At the end of the entire mock admission, we asked participants for their summative feedback through a semistructured qualitative interview (interview guide in the online supplemental). Patients did not have a prior relationship with the interviewers and were not told interviewers characteristics. Interviews were conducted in-person by trained qualitative interviewers (DML: MD, MPH, principal investigator, male; MPD: MPH, research assistant, female). Interviews were only conducted in English.
Key baseline features of the rural home hospital model
Prior to learnings described in this study, the rural home hospital model included a remote physician guided by a mobile integrated health paramedic or nurse (heretofore ‘in-home clinician’), advanced point-of-care testing including blood diagnostics and ultrasound and continuous biometric monitoring (figure 1). The model also included a health monitoring device which provided continuous physiological measurements to the clinical team in real time. The model includes dedicated in-home medication storage as well as pharmacy and durable medical equipment home delivery. Care workflows designated patient assessment and remote physician consultation procedures for admission, daily rounding and discharge. Internet connectivity was ensured through a cascading approach that sought to prioritise fast and easily available systems first. We therefore would access, and if necessary deploysystems in the following order: in-home broadband (digital subscriber line, cable or integrated services digital network), smart-device cellular, 4G antennae, and finally portable broadband global area network satellite.

Key features of the rural home hospital model. (A) Physician performs remote facilitated history and physical. (B) Kitchen walk-through to discuss low sodium foods with remote physician. (C) Point of care ultrasound delivered in real-time to physician. (D) Portable satellite communication system set up in front yard. (E) View from patient’s front yard. All persons pictured gave permission for use of images.
Qualitative analysis
All clinician and patient qualitative interviews were audio recorded and then transcribed verbatim. All participants gave written informed consent to participate.
Our analytical approach borrowed from grounded theory, which involves open coding (comparing and conceptualising the data), followed by axial coding (forming groupings based on relationships in the data), and then finally selective coding (describing central themes).20 21 A codebook was developed based on the first three interviews and subsequently refined throughout the coding process to create domains and subdomains.
The transcripts were analysed using two-person consensus (MPD, JBR). One investigator coded each interview (MPD) using qualitative analysis software (NVivo V.12, V.12.2.0) and a second investigator (JBR) reviewed each coded transcript. Throughout the process, the two investigators (MPD, JBR) debriefed with each other to clarify concepts and refine codes, with oversight from DML. Any discrepancies in coding were discussed and finalised by consensus. Following this analytic approach, we finalised central themes and used our learnings to inform the development of the rural home hospital model.
Patient and public involvement
Patients were involved in the testing of this innovation, and their feedback will continue to drive the model.
Results
Preliminary mock admission in a simulation centre
After significant research and field observations, we recognised several key design elements necessary to answer the challenges of deploying rural home hospital care (table 1). We tested Internet connectivity under various bandwidth stressors. We noted that various communication software platforms performed adequately for video at 50 kb/s, audio at 25 kb/s and text message at 2.5 kb/s. We tested various Internet connection options, including cellular 4G, 4G antennae, portable broadband global area network satellite and satellite telephones. 4G options worked optimally, portable satellite produced usable but choppy video, and satellite telephones allowed for clear bidirectional audio.
Challenges and solutions to rural home hospital care delivery
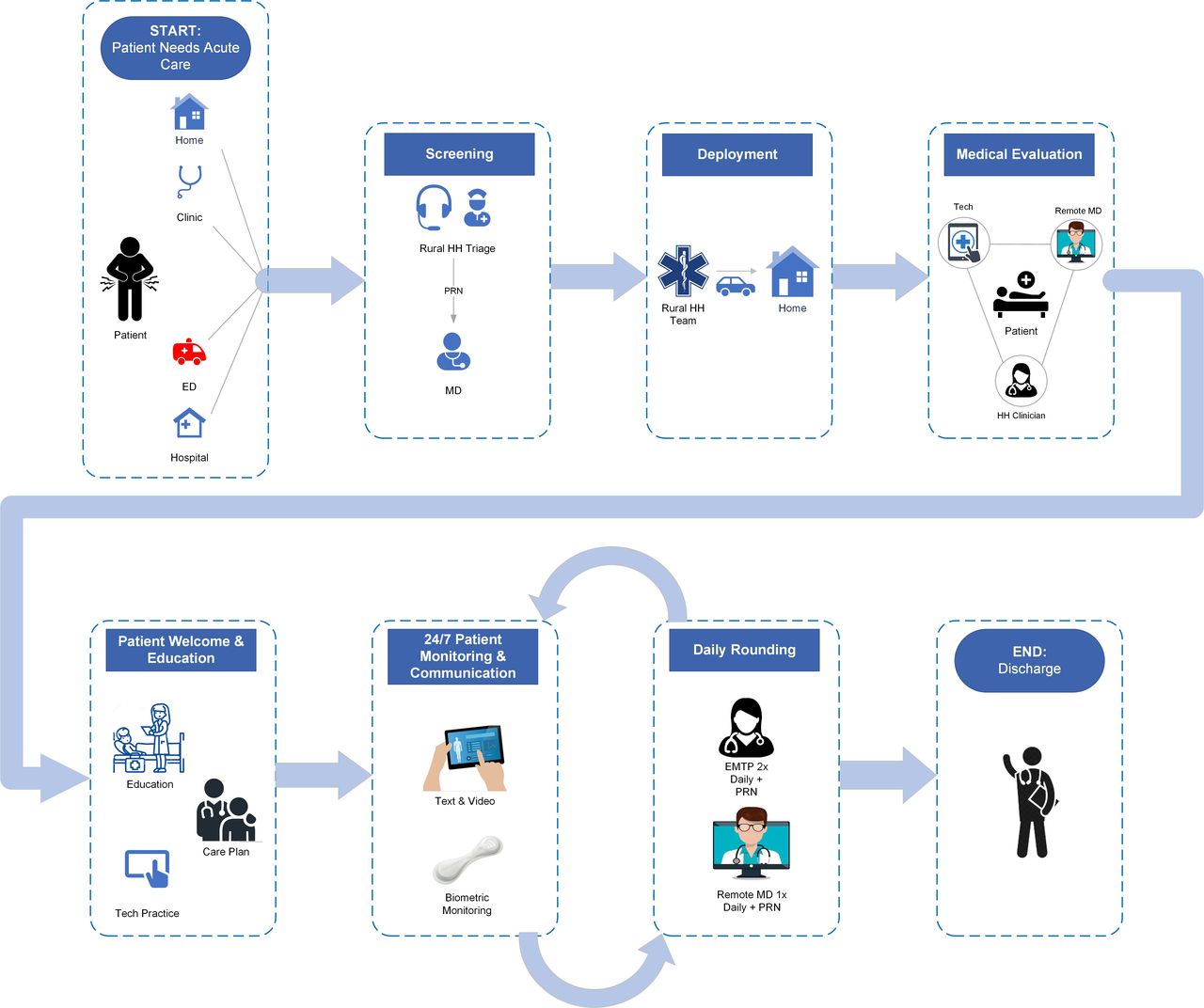
We ran and repeated our workflows for admission (welcome, technology set-up and clinical intake), daily rounds (one morning in-home clinician visit followed by a virtual (if possible) afternoon visit for clinical management), and discharge (coordination) multiple times, enabling us to fine-tune and optimise workflows. Total admission workflow required approximately 45 min. Learnings included the need for a Bluetooth speaker, tablet stand, satellite extension cable and parallel workflow for physician and in-home clinician, with the physician performing a history while the in-home clinician set up systems and collected data. Daily rounding required approximately 25 min after streamlining workflows so that the in-home clinician collected vitals prior to initiating the video call with the physician. Discharge required approximately 25 min, similar to daily rounding. However, this did not account for the time required to disconnect and clean all equipment used for the home hospitalisation and provide patient postdischarge instruction. These exercises facilitated the creation of workflow maps for the rural home hospital care model used to guide the mock admissions in rural Utah (figure 2).

{kind=link}
{kind=link}
Workflow map for rural home hospital. ED, emergency department; EMTP, emergency medical technician paramedic; HH, home hospital; MD, medical doctor.
Study team observations during mock admissions in rural Utah
Study team members noted the cascade approach to Internet connectivity demonstrated adaptability and resilience to conditions encountered in the home. Video conference calls between the patient and physician were achieved with high audio–visual quality using in-home broadband, smart devices with native cellular connections, 4G antennae and satellite. Bandwidth limitations arose, including data lag and freezing, when transmitting biometrics, point of care ultrasound and video conferencing simultaneously. The team noted the simplicity, reliability and performance of 4G antennae set-up when other non-satellite options were unavailable. The use of in-home Internet systems, while cost effective and typically reliable but not always present, created a dependency between the in-home clinician and patient and/or their caregiver who may not be able to assist or guide the connection process and were slower to establish. 4G connected devices required the least amount of time and effort to deploy but were heavily impacted by bandwidth fluctuations and showed significant video lag when attempting to connect to multiple devices and/or be used as hotspots. Study team members also noted that in general patients had limited technology literacy, requiring the facilitation of the in-home clinician for nearly all tasks. Larger screens with loud audio and single screen taps and friendly user interfaces would be high yield.
Study team members noted that the physician–patient interaction was inefficient prior to rapid cycle feedback, with repetition between the in-home clinician and the physician. Streamlining roles for each clinician before, during and after the video improved timing and teaming.
While conducting the admission, daily rounds and discharge workflows with mock admissions patients, the study team introduced various stressors to test and improve on the technology approach. Simulations included a sudden failure of the in-home Internet, power outage, low and fluctuating cellular signal and unexpected video failure. By using 4G connected devices and satellite, disruptions to in-home power or Internet services were mitigated. Weak cellular services had the greatest impact. Video failure, due to power outage or weak cellular service, necessitated deployment of satellite. Clinicians responded favourably to the use of satellite to maintain patient monitoring telemetry when coupled with in-home, cellular or satellite phones to provide an audio connection between the patient and the physician. When video was needed after an Internet or cellular failure, satellite provided satisfactory audio–visual video quality to execute all workflows, but all other Internet usage had to be halted during the video call.
Patient and clinician formative feedback
The in-home clinician reported that communication and task management with the physician was strengthened through the use of an online task management system which allowed the physician to provide updates to the patient’s care plan in real time. The physician identified the need for a preadmission or deployment protocol when the patient’s electronic health record is reviewed. Such a protocol might also include a brief preassessment check-in between the physician and the in-home clinician to share any concerns and confirm if any changes to the standard admission workflow process would be advisable. The physician emphasised the importance of having high resolution video for conducting the patient assessment.
A patient noted that being in the home allowed for new ways of interacting with the care team, giving the example of a kitchen walkthrough, where the patient learnt about high-sodium foods in the kitchen as the cause of a heart failure exacerbation. Patients felt that continuity of care during their admission would be better in rural home hospital than the hospital. During discharge, patients also expressed a desire for a clear handoff between their rural home hospital team and any subsequent recommendations for follow-up clinical care.
Patient and clinician summative domains
Three domains emerged in which clinicians, patients and caregivers expressed views on their experience with the rural home hospital mock admission: (1) comfort level during rural home hospital, (2) perceived safety during rural home hospital and (3) perceptions of rural home hospital workflow (table 2).
Domains, subdomains and illustrative examples of summative patient and clinician mock admission experience
Comfort level during rural home hospital admission
Patients and caregivers expressed a preference for home versus traditional hospitalisation for acute illness: ‘I really hope that I will be able to stay in my home until I die. I don’t want to be someplace else. And I don’t want my husband to be someplace else either.’ They also noted that rural home hospital meant significantly less time spent waiting in an unfamiliar and uncomfortable hospital waiting room or hospital bed (table 2, 1a). They cited the patient centeredness of the rural home hospital model: ‘[E]verybody’s right here helping and watching and checking.’ This allowed for a comfort and ease they had not experienced previously: ‘[H]aving someone that you could call that could come [would be] a lot easier than…go[ing] up to the hospital. It sometimes gets to be really hard… mostly in the winter, when it’s cold and miserable…I undoubtedly get pneumonia or get sick or something.’
The in-home clinician expressed that the rural home hospital model did not put ‘any undue stress or burden’ on the patient. He noted that his comfort level improved between the first and second mock admission secondary to having more experience and practice with processes and the technology. The physician expressed that she, ‘liked that the patients were really happy staying in their home’. She also explained that a challenge with the admission process could be initial diagnostic uncertainty, given the patient does not receive a complete emergency department workup, and she was not able to be physically present for an exam (table 2, 2a).
Perceived safety during rural home hospital
Both patients and caregivers felt that care was being delivered safely during their rural home hospital mock admission. Patients were comfortable with a remote physician: ‘I feel like she was able to do her job by knowing the facts, …what was wrong, and what could be done for it.’ One patient described that due to the inconvenience, she often delayed seeking hospital care (table 2, 3b). The patient went on to describe that having the option to receive hospital-level care at home would make her more likely to seek timely care.
The in-home clinician felt that care was delivered effectively and safely ‘in every way’ during the mock admissions. One potential safety concern raised by the in-home clinician was inclement weather making driving to patient homes challenging. The physician felt that ‘going into people’s homes is insightful about how they take their medicines’. She noted it allowed her to identify safety issues: [Patient] med[ication] boxes are a mess, and it gives you so much insight into a patient’s life and what’s realistic for them to do and not do when you actually see them in their home environment’. She suggested use of a shared medical record and involvement of a remote pharmacist would serve as important additional safety measures (table 2, 4b). The physician also noted concerns with ‘not being able to physically touch the patient’, resulting in a physical exam that was ‘not good’ due to technology issues (camera aimed in the wrong direction, pixelation of video) and felt she needed to rely on the in-home clinician’s physical exam. She expressed that the physical exam ‘is a really valuable part of delivering safe care’ and it was ‘the main thing that was compromised’.
Perceptions of rural home hospital workflow
Inefficient processes
Patients made no mention of inefficiencies in their care. The physician suggested the need for streamlined workflows between the in-home clinician and physician to alleviate any duplicative history and physical exam activities (table 2, 5c). The physician also noted the tension of being available for the remote clinician while also tending to other patients’ needs: ‘[Y]ou… have to be available at a computer whenever you're needed, so [it is harder to] multitask in between that’. Of note, both these issues improved after several rapid cycle improvements.
Both the physician and in-home clinician found switching between different technology platforms was inefficient: ‘[I]t was… annoying switching screens, and I felt like I ignored some of the screens because they weren't just all in front of me at once’. There were challenges with the digital stethoscope such that the physician felt it would be difficult to hear a heart murmur due to the poor quality of the patient’s heart sounds.
Efficient processes
Patients and caregivers appreciated the efficiency of the rural home hospital model. As previously noted, every aspect of wait time was minimised including admission, daily rounds and discharge, and patients did not mind waiting in their own home with their loved ones (table 2, 6d). One patient cited an experience of inpatient diuresis and the struggle of having to wait to be disconnected from his IV: ‘[W]hen you're doing Lasix and when it says time to go to the bathroom, you ain't got no time to spare. And then you have to buzz them, takes them 10 minutes to come in and unhook you, …and then 10, 15 minutes to hook you back up’.
The in-home clinician enjoyed the ‘unhurried feeling’ of providing care and felt that being in the patient’s home helped facilitate quality care: ‘When you can get the patient in their environment and can see how they live…, I just think this is better. The environment tells me a lot about the patient…’ He also noted the quality time that the remote physician was able to spend with each patient (table 2, 7d). During daily rounds, the physician liked that the in-home clinician could just contact her when he was ready with the information she wanted. Both noted the collaboration platform used in the mock admission helped make rounding efficient: ‘I could just give a brief checklist of what data I wanted…, so then [the in-home clinician] can have that stuff ready ahead of time and make it efficient from my end…’
Team collaboration
The in-home clinician ‘felt further removed’ from the remote physician and said that ‘this is not the same as face-to-face’ where you can develop a relationship working physically side-by-side, although he also acknowledged that their remote interactions were extensive. He expressed that having met the physician in-person helped their working relationship when compared with only meeting over videoconference. Both noted trust among treating clinicians was paramount. The physician also noted the power of collaborating effectively, such that the in-home clinician could be the remote hand of the physician, performing detailed medication reconciliation and education (table 2, 8e).
Both noted rural home hospital needed to adapt to training differences among all clinicians. The physician expressed that paramedics may not have the in-hospital experiences that help them understand the data a physician is interested in, although she noted, ‘I think that this would get better the more you work with somebody, and this was our first time doing it’.
Technology
Patients and their caregivers had no concerns with any of the technology, including the use of continuous patient monitoring. One patient preferred the rural home hospital monitoring compared with the traditional hospital because the monitoring was wireless.
The in-home clinician expressed that the wireless continuous patient monitoring technology was powerful and a ‘very high-yield tool’. He felt that the ‘learning curve was short’ with some of the technology. He did express the need for more training and practice to become familiar with some of the technology and felt that by the second mock admission he had become better acquainted. The physician noted that better positioning of the camera in a patient’s home so that she could see the patient’s face, ability to control the camera’s positioning, and improved resolution were all areas for enhancement (table 2, 9f). The physician noted she could see ‘[some] physicians struggling a little bit with the technology since there were so many different platforms that we were using’.
Discussion
In this simulation analysis of rural home hospital, we demonstrate that acute care delivered in a rural home is technically feasible, acceptable to clinicians and delivers a positive patient experience. Given the dearth of evidence in rural home settings, we purposefully began with scoping exercises using a simulation laboratory and then moved to rural homes. Through a rapid cycle feedback approach, we fine-tuned workflows, personnel and technology deployments to enable acute care delivery in the rural setting.
Our work builds on the home hospital literature that suggests high-value care can be delivered to patients in mostly urban environments.16 22 To our knowledge, few home hospital programmes operate in rural areas due to the challenges of geography and connectivity. With the use of the right technology and workflows, this scoping exercise demonstrates the possibility of rural home hospital care for a carefully selected patient population. It further builds on our recent work detailing rural patient and clinician interest in the care model.19
We identified the need for remote care physician training. Significant aspects of the physical exam can be performed by video, especially with a facilitator such as an in-home clinician, yet few physicians receive training in this method of patient assessment.23 24 Multiple randomised controlled trials have found remote care non-inferior to in-person care.25 Facilitated video interaction, coupled with point of care imaging and laboratory analysis, reduces physician uncertainty. When considering the workforce needs of the in-home clinician, it is likely that various clinical roles practising at the top of their license may fit the role well: mobile integrated health paramedics,26 27 nurses, and highly trained community health workers.28 Customising a programme to a local area’s offering will be important.
Participant insights helped us to identify additional areas for improvement. Clinicians mentioned the challenge of using so many apps and systems, suggesting the need for a home hospital technology platform that unifies the various technologies under one ecosystem. We made great improvements in parallel workflows as we deployed rapid cycle feedback, further structure (perhaps in the form of checklists) can be helpful in optimising remote physician and in-home clinician workflow.
Finally, given the physician and in-home clinician may not always have synchronised schedules, care may be facilitated if the physician creates rule-based plans for the in-home clinician to follow. For example, diuretic dosing based on specific weights would obviate the need for the in-home clinician to contact the physician during a second visit. It may be that rural home hospital requires additional communication norms than are typical of hospital-based care.
While potentially highly disruptive in how we deliver acute care in rural settings, the rural home hospital model, as all care models, is not a panacea. Just as in urban home hospital programmes, clinicians must be careful to select appropriate patients such that the programme’s capabilities match the patient’s needs. Not all acutely ill patients will be eligible for rural home hospital. Prior to admission, clinicians and patients should have a clear view of the risks and benefits of rural home hospital. A discussion should be had with the patient about the limitations of home hospital and how the model compares to traditional hospitalisation. For example, for a carefully selected patient, an emergency event has a very low likelihood, yet an adverse event in a hospital affects about one in ten.29 Receiving care in a rural home may therefore carry fewer risks. The present model discussed in this simulation analysis begins in the home; however, several other admission pathways exist including the patient presenting acutely ill to a clinic or emergency department, or if a patient is admitted to the hospital and requires additional days of acute care and the patient is appropriate for home hospitalisation (‘early transfer’). Finally, although cost in urban settings is demonstrably lower in multiple studies, teams need to consider the added cost in rural areas of travel and specialised communication technology compared with the cost of traditional hospitalisation. This requires further research.
Our study has limitations. First, we performed only two simulations in two rural regions of Utah involving two clinicians, limiting generalisability. Although rural areas share many themes, they each have unique pressures and variables. It may be that in some areas our designs will work better and in others worse. We did purposefully choose two highly rural areas in an attempt to stress the system as much as possible. In addition, other clinicians and patients may have different perspectives. Second, the clinicians participating in the simulation were accustomed to practicing in rural environments. It is possible that other clinicians may require additional training to perform well in this care model. Training should include using simulations with different scenarios including urgent and emergent situations. Third, given the simulated nature of this study, it is possible new improvements will be required to be made to the rural home hospital model. We anticipate future research will address this.
Our simulation analysis demonstrates the feasibility of delivering acute care in a rural home setting. We anticipate these findings represent the first step in driving a paradigm shift in the delivery of hospital-level acute care in rural America.
Data availability statement
No data are available.
Ethics statements
Ethics approval
This study was approved by the Partners HealthCare and University of Utah Health institutional review board.
Acknowledgments
The authors would like to acknowledge Kevin Carr for his assistance with workflow mapping.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @davidlevinemd
Contributors DML, JBR, MPD: substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; and drafting the work or revising it critically for important intellectual content; and final approval of the version to be published; and agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. NC: the acquisition, analysis, or interpretation of data for the work; and drafting the work or revising it critically for important intellectual content; and final approval of the version to be published; and agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. SH: the acquisition, analysis or interpretation of data for the work; and drafting the work or revising it critically for important intellectual content; and final approval of the version to be published; and agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding This work was supported by an Ariadne Labs Spark Grant, Boston, MA.
Competing interests DML receives funding from Biofourmis for an investigator-initiated artificial intelligence study on deterioration of home hospital patients.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.