Article Text

Abstract
Background Healthcare systems revolve around intricate relations between humans and technology. System efficiency depends on information exchange that occur on synchronous and asynchronous platforms. Traditional synchronous methods of communication may pose risks to workflow integrity and contribute to inefficient service delivery and medical care.
Aim To compare synchronous methods of communication to Medic Bleep, an instant messaging asynchronous platform, and observe its impact on clinical workflow, quality of work life and associations with patient safety outcomes and hospital core operations.
Methods Cohorts of healthcare professionals were followed using the Time Motion Study methodology over a 2-week period, using both the asynchronous platform and the synchronous methods like the non-cardiac pager. Questionnaires and interviews were conducted to identify staff attitudes towards both platforms.
Results A statistically significant figure (p<0.01) of 20.1 minutes’ reduction in average task completion was seen with asynchronous communication, saving 58.8% of time when compared with traditional synchronous methods. In subcategory analysis for staff: doctors, nurses and midwifery categories, a p value of <0.0495 and <0.01 were observed; a mean time reduction with statistical significance was also seen in specific task efficiencies of ‘To-Take-Out (TTO), patient review, discharge & patient transfer and escalation of care & procedure’. The platform was favoured with an average Likert value of 8.7; 67% found it easy to implement.
Conclusion The asynchronous platform improved clinical communication compared with synchronous methods, contributing to efficiencies in workflow and may positively affect patient care.
- inventions
- medical apps
- mHealth
- assistive technology
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Healthcare systems revolve around intricate relations between humans and technology, enabling the modern healthcare professional (HCP) to provide efficient services to patients.1 The efficiency stems from the exchange of critical communication using synchronous (face-to-face interactions, phone conversations) and asynchronous (instant messaging (IM), email and electronic/paper-based health records) communication methods.2 3 Currently, healthcare is heavily reliant on synchronous communication despite its association with interruptions to workflow, distractions and unsatisfactory outcomes in the delivery of care.2 3 This subsequently has led to medical errors, increased length of stay (LOS) in hospital, work stress, fatigue and anxiety, which undermines the quality of care and patient safety.4–7 Combining these factors with an already stretched healthcare system, higher costs, staff burnout and low levels of morale are suffered.8 Emergency messaging aside, synchronous methods are also devoid of any temporal or spatial information as well as context, urgency or complexity of the task at hand.9–12
Therefore, the system is ripe for change. Asynchronous methods of communication are already widely used in industry, in fact, the Topol Review hails the adoption of technology to enable enhanced patient–clinical relationships with improvements to patient experience and safety.13 Implementing digital technology also has the aim to fulfil the goals of the 5-Year-Forward-View: higher quality healthcare with greater value for the taxpayer.6 14 The need for an efficient healthcare system is even more paramount in the pandemic of COVID-19, where inextricably high patient case-loads have placed tremendous demand on healthcare and staff resources.15 Healthcare is now dispersed throughout different times, locations and multidisciplinary boundaries. With or without the emergence of a global pandemic, healthcare is yearning for an efficient solution, which asynchronous communication may provide.3 8 9 15 16
The domains in which synchronous and asynchronous communication platforms can be compared are efficiency of resource utilisation, effectiveness of core operations and service quality and quality of work life (QWL).
Efficiency of resource utilisation
Efficient communication between all stakeholders throughout the patient journey is integral to safe and effective care delivery.17 18 As disease burdens and complexities increase (as seen with COVID-19), and HCPs work in different times, across larger distances and under different specialties and competencies, it is crucial to ensure that the quality of care is not compromised.19 20 Studies exploring the relationship between communication systems, flow and their effects on hospital processes foreshadow multiple implications for care delivery, such as efficiency in resource utilisation.17 21 Constituents of this domain include healthcare practitioner time in discharge planning, escalation of care and transfers.17 21 Research has shown that digital communication technologies and time saving protocols lead to workflow efficiencies.3 21 More specifically, synchronous communication contributes to inefficiencies in resource allocation and communication.3 Detrimental effects to patients and HCPs may therefore be observed since every point in communication in healthcare is important. In contrast, the adoption of an asynchronous system resulted in 4 hours saved per patient transfer22; changing HCP communication methods can lead to significant time savings.21
Effectiveness of core operations
Disruptive notifications due to pagers have been implicated in several studies as being directly or indirectly associated with medical errors and patient safety outcomes.7 22 Core operations include outpatient consultation, admission, diagnostics, therapeutics, surgeries, transfer of patients within the hospital and discharge. In studies exploring drug dispensing, interruptions conferred to a 12.1% increase in procedural failures and a 12.7% increase in clinical errors.23 It was also found that communication-related endpoints contributed to the majority of clinical errors.24 On the contrary, utilisation of mobile phones by physicians led to a 19% reduction in risk of medical errors alongside efficient escalation of patients’ care.25
Studies exploring healthcare communication practices have exposed that traditional methods contribute towards untimely reviews and communication bottlenecks associated with increased patient risk and LOS.17 These procedures were identified as ‘non-value adding activities’ that were subsequently related to delayed patient care and patient safety implications.19
Service quality and QWL
Synchronous communication practices are associated with increased rates of cognitive workload, burnout and user dissatisfaction.26 This is due to the increased amount of multitasking, disrupted thought processes and additional work stress.26 On the contrary, asynchronous communication methods can reduce the majority of frustrations that HCPs may have, such as the inability to identify other HCP’s work role and absence of responses.27 Addressing these issues can increase the efficiency of staff by improving their cognitive abilities.
Aim
We sought to compare traditional synchronous methods of communication to an IM asynchronous platform, Medic Bleep, and observed its impact on clinical workflow, QWL and hospital core operations at West Suffolk NHS Foundation Trust (WSFT).
Methods
The multimethods prospective study had two separate arms, evaluating both quantitative and qualitative endpoints across three varied clinical sites (surgical, medical and community). The time-motion study (TMS) allowed researchers to observe participants on clinical tasks duration and movements required to accomplish a specific task coupled with an analysis focused on improving efficiency of workflow.
Communication between HCPs was analysed to observe differences in task completion times and its impact on care quality and delivery, efficiency and end-user perception.
Participant selection
Three clinical sites were identified to assess and compare the quantitative effectiveness of the asynchronous IM platform: the trauma and orthopaedics ward (F3—surgical), the maternity ward (F11—medical) and the maternity day assessment unit (community). Selection of these particular clinical environments was due to the distinct medical, surgical and community staff hierarchies they offered, allowing us to observe a microcosm of the communications that exist in a typical hospital. Staff volunteered to be observed during this pilot and were consented. Ethical procedures were followed in line with guidance from WSFT and registered accordingly. Participants were allocated via a random number generator to use the conventional pager or asynchronous IM for communication. Participants specifically included two doctors and two nurses of at least foundation year one and band five grade, respectively. Following this, participants observed in each study site were provided with qualitative questionnaires (see online supplemental appendix).
Supplemental material
Intervention
Prior to the study, both cohorts were given a 2-week acclimatisation period to engage with the asynchronous IM platform. This included verbal and written information on standard operating protocols, staff training (including how to optimally use the application) and staff debrief sessions to ensure end-user buy in and engagement.
Comparator
We used a TMS design to evaluate our primary objective. Continuous time–motion observations were performed with HCPs in all three clinical areas both before and after the asynchronous communication platform implementation. Observers included both independent recruits from West Suffolk Hospital and individuals from the researcher’s team. They followed participants throughout their normal clinical activities and timed activities requiring interpersonal communication.
Outcomes
Following the recording of communication events, data was extracted and stratified into the initiator and receiver of each event, the category of clinical event, response times and the number of messages between primary task initiation and task completion. Measurement of outcomes was initiated when giving a task and ended when the task was completed.
Statistical analysis
All statistical tests were conducted by an independent statistician using GraphPad Prism 6 software. The Shapiro-Wilk test was used to determine whether data sets were normally distributed. All normally distributed data sets were analysed by unpaired t-tests, while non-normally distributed data sets were analysed by Mann-Whitney U tests. Computing and statistical significance was taken at the 95% CI.
Subcategory analysis was also performed separating tasks into specific clinical domains:
To-Take-Out (TTO).
Discharge and patient transfer.
Patient review.
Escalation of care and procedure.
Drug round and observations.
Clinical documentation and meeting.
Qualitative analysis included a questionnaire (see online supplemental appendix) that was created using the authors’ experiences in clinical communication and using current market research based on the extant literature on digital communication and focus groups at WSFT. The post pilot questionnaire administered to all staff in September 2017, allowed the analysis of end-user perception, appetite for pager replacement and whether asynchronous communication would improve the completion of typical clinical tasks.
Results
Quantitative analysis
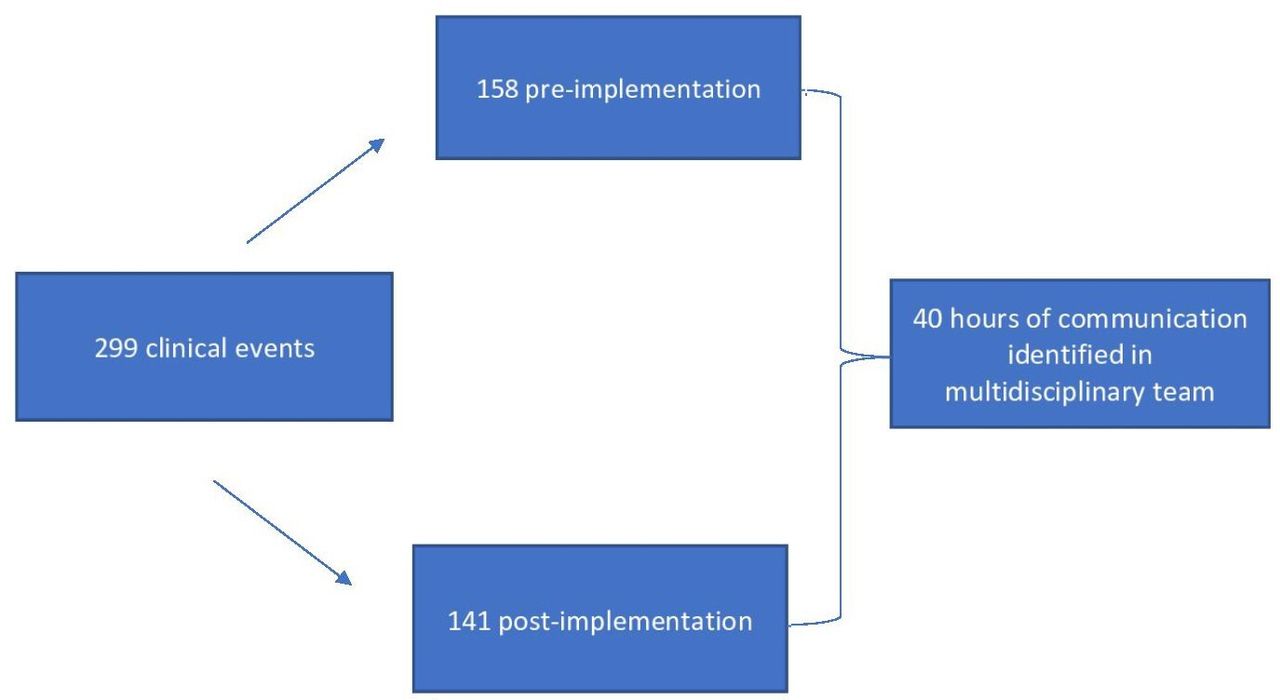
Four doctors (trainees) and four nurses (band 5–6) were observed using the TMS methodology for two days each, prior to and during the observational study; amounting to eight days in total. Figure 1 below shows the hours of communication identified and their divisions according to preimplementation and postimplementation between the multidisciplinary healthcare teams.

Information event flow diagram.
This gave a frequency of an event on average every 21.5 min, with a range among subjects to an event every 3 to 75 min.
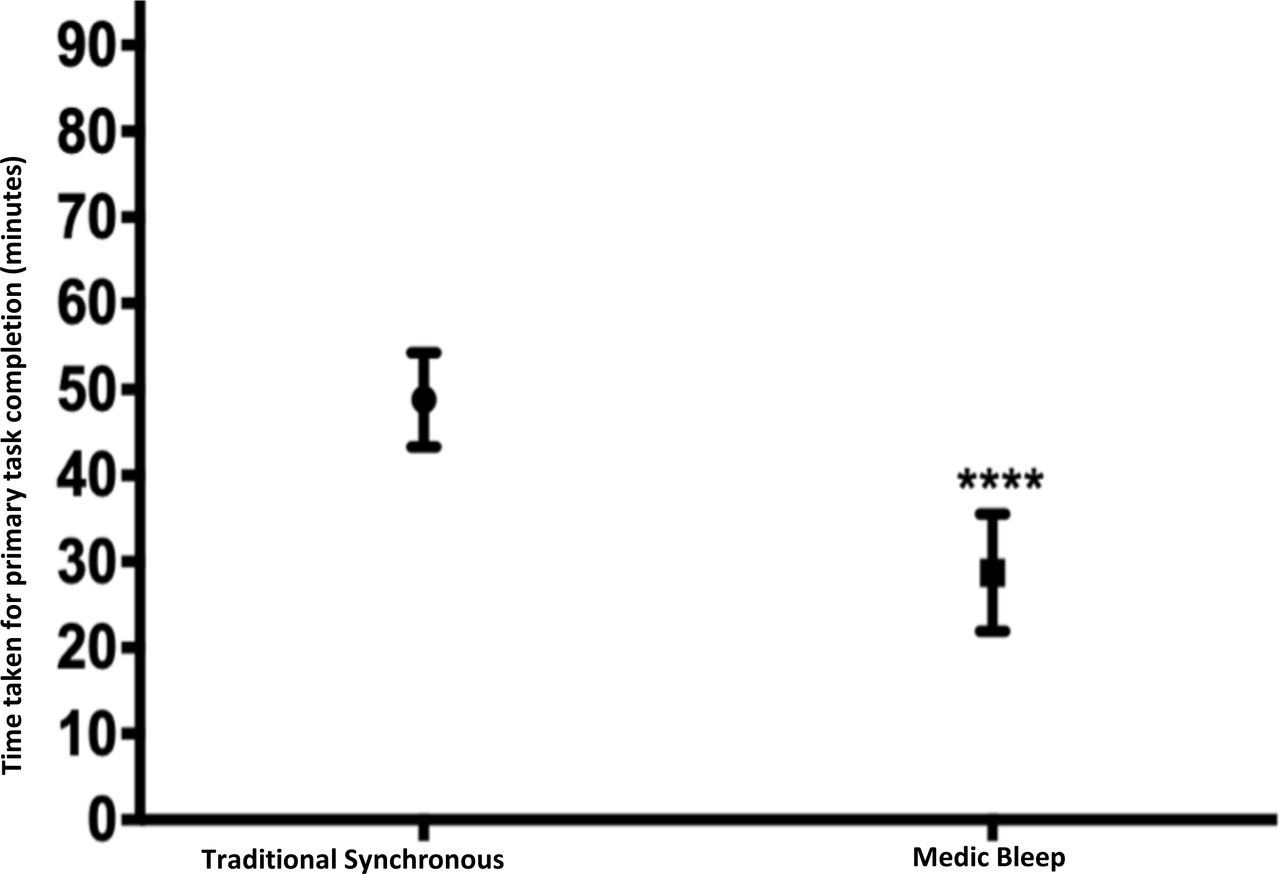
Statistical analysis revealed that asynchronous methods of communication resulted in on average 20.1 min reduction in task completion—amounting to a mean reduction of 58.8% when compared with traditional synchronous methods. These results were statistically significant (p<0.01). Figure 2 below shows the comparison between synchronous and asynchronous methods.
{kind=link}
{kind=link}
Primary task completion: synchronous methods versus asynchronous methods.
Table 1 below illustrates staff roles and its association with statistically significant reductions in time.
Subcategory analysis comparing time reduction by staff role and task
Qualitative analysis
Respondent demographics
A total of 37 HCPs responded to the post-pilot questionnaire from the three ward-based and singular community study site. There were 24 (65%) female respondents and 13 (35%) were male. Role demographics of the respondents were as follows: 15 doctors, 7 nurses and 15 allied health professionals.
Devices
More than half (55%) of the staff used their own devices with 45% of staff using either Trust-issued phones, tablets or PCs. An Apple iOS device was the most commonly used device (54%), followed by Android devices (16%), with the remainder (20%) who used a web browser on a desktop PC. The asynchronous platform was the most used and de facto communication method during the pilot followed by in-person communication. WhatsApp and the traditional pager were the least used forms of communication, respectively.
Training and standard operating procedures (SOPs)
Rigorous training provided on-boarding advice and embedding staff into application use and SOPs; staff found that training was sufficient (72.5%), helpful (75%) and quick (70%). Furthermore, staff were asked whether user guidance and frequently asked questions were sufficient. It was observed that 80% of staff considered that it was ‘helpful’ with the remainder finding it ‘unhelpful’.
Benefits of the asynchronous platform
Staff cited that escalation of care, contacting on-call physicians as well as instant collaboration were the dominant factors for the use of the asynchronous platform (see table 2 below). The speed of response time using the asynchronous platform was also questioned about; 30% of staff indicated a response time below 5 min with 40% of staff indicating a response time of up to 15 min. From the respondents, 70% reported that the asynchronous platform improved or greatly improved interprofessional communication with 5% claiming that it had worsened communication. A 24% increase was observed in staff who believed that their discharge management plans were completed quicker with the asynchronous platform compared with synchronous methods. Regarding overall speed, 52.5% of staff felt that this new modality of communication was faster than traditional methods of communication.
Staff reasons for using the asynchronous communication platform
Impact of asynchronous IM
The majority of respondents (62.5%) felt that asynchronous communication had a positive impact on productivity and a further 35% claimed that it did not affect productivity, 5% claimed that it was inferior. Similarly, positive impacts were observed on the patient experience with 45% agreeing that it directly impacted patient care and 55% claimed that it was no different. A further 87.5% claimed that patients and relatives responded positively to its use. Majority of staff (92.5%) confirmed the onboarding process offered easy registration; 75% of staff found it easy to adopt into their working day and 67% found it easy to implement. Respondents felt that sufficient and timely communication increased by 20% after the introduction of the asynchronous platform (72.5% pre-pilot and 92.5% post-pilot). Similarly, 92.5% of respondents felt that adequate support was available throughout the pilot programme. When asked how likely staff would recommend an asynchronous way of working, an average value of 8.7 was observed (with 1 being not likely and 10 being extremely likely).
Challenges with asynchronous IM
Concerns or challenges throughout the pilot programme were also addressed. A large proportion (43%) of respondents cited no concerns or challenges, the remainder of respondents cited the following: the standardisation of a singular form of communication (22%), WiFi and connectivity issues (8%), battery and charging issues (8%) and lastly no response (19%). Most staff (67.5%) were comfortable or indifferent with using their own mobile device; however, the remainder (32.5%) were not comfortable with using their own device and preferred using Trust-issued devices.
Discussion
Using quantitative and qualitative methods, we compared traditional synchronous communication methods with Medic Bleep, an asynchronous IM platform, at three wards in West Suffolk Foundation Trust. Asynchronous communication proved to be effective with respect to workflow, efficiency of resource utilisation, effectiveness of core operations, service quality and QWL.
Efficiency of resource utilisation and effectiveness of core operations
A statistically significant reduction of 20.1 min in task completion was seen when using asynchronous methods of communication, reducing time taken to complete tasks by more than 58.8% compared with synchronous methods. This is supported by the extant literature and reinforces asynchronous communication’s ability to increase the efficiency of services given to patients by saving time.3 21 22 28 Subcategory analysis of how time was saved with respect to type of task shows that core hospital operations such as TTO, patient review, discharge and patient transfer and escalation of care and procedure, all had statistically significant reductions in time taken. This may be due to the asynchronous communication platform’s ability to convey ‘instant messages’ and notify respondents with equal speed—a feature synchronous methods lack.17 28 Our qualitative results support this, as participants stated that timely collaboration with other teams and prompt escalation to seniors were principal proponents for using the asynchronous method.
Qualitative studies exploring healthcare communication practices have exposed that traditional communication methods have contributed to untimely patient reviews and bottlenecks associated with increased patient risk and LOS.17 On the contrary, process mapping revealed a reduced number of steps and wait periods when using the asynchronous platform, thereby potentially reducing LOS and improving the patient journey. Indeed, delayed patient care including increased LOS, delayed discharge and transfer are shown to have dire patient safety implications.19
Rivera-Rodriguez and Karsh7 acknowledge the necessity of interruption in healthcare and conclude that it is only detrimental if interruptions are prolonged. This may be due to divided attention and deterioration of information held prior to the interruption, causing HCPs to take longer to get back to their initial task. Since a quick glance at the IM application addresses the interruption concern, it would explain why interruptions with the asynchronous platform were met with reduced time to complete tasks. Although, previous literature shows decreased patient satisfaction with greater interruptions, the survey showed that 87.5% of patients and relatives were optimistic towards the asynchronous communication platform.7 23
Service quality and QWL
Following the pilot questionnaires, results indicated a 24% increase in staff who believed that their discharge management plans were completed quicker with asynchronous methods. Discharge management plans are often cited as a major bottleneck in the patient journey and a rate-limiting step of discharge.29 Creating an efficient discharge process is key to reducing lengthy hospital stays and a major determinant to patient satisfaction.29 30
Moreover, staff indicated a high appetite to replace the non-cardiac pager with an average Likert scale value of 8.7, implying that asynchronous channels would be highly recommended to friends and colleagues. With a number of digital systems being implemented, it is difficult for organisations to understand which interventions will provide a return on investment. The technology acceptance model focuses on the likelihood of users to accept technology by examining ‘ease of use’ and ‘usefulness’ to be positive correlators to the actual use of a system. With high user acceptance, ease of implementation and a high appetite to displace synchronous systems, the asynchronous platform has been evidenced to improve QWL, acceptance and actual use of the system.31
Strengths and limitations
Strengths of this study included a wide range of clinical personnel, staff roles and wards highlighting the scope and scale of how an application-based IM device could result in task and role-based efficiencies in a large NHS hospital. Accurate time stamping of clinical communication removed potential interpretation error. However, the study sample was small in number and a limited number of total staff members were followed using the TMS methodology. Furthermore, although training was conducted to ensure that appropriate messaging protocols were followed, the effect of positive engagement and the influence of the platform onsite could result in higher levels of active users.
Future implications
Considering the COVID-19 pandemic, asynchronous communication could serve multiple purposes, including communicating emergency department and critical care bed load, practicing effective leadership via text or voice, allowing for trusted communication between HCPs and giving instant updates about guidelines and dissemination of critical information. The implementation of this asynchronous communication platform has proved fruitful at West Suffolk Foundation Trust; however, more research needs to be conducted looking at the direct association of patient safety outcomes and its ability to assist in the COVID-19 crisis.
Conclusion
Current synchronous methods of communication can disrupt interprofessional communication in healthcare organisations and affect the patient journey. This study shows that asynchronous communication modalities reduce the time taken to complete tasks by 58.8%, saving 20.1 min of time. These workflow efficiencies are associated with reduced patient LOS, increased patient safety outcome and QWL, alongside producing a collaborative work environment. Users experience high levels of satisfaction, including perceived improvements in communication and delivery of patient care. Further research exploring clinical communication in a larger study sample will expand the knowledge base on the causal aspects affecting clinical communication and also evaluate the benefits of asynchronous communication platforms on patients, staff and organisations.
Acknowledgments
This research would not be possible without the hard work and diligence of West Suffolk Hospital NHS Foundation Trust. In particular, we would like to thank Dr Nick Jenkins, Mr Dermot O'Riordan and Rowan Procter whose insight and expertise were integral to the success of this study. Guidance from our contributory authors Yat Wah Li, Adam Devany, Harpreet Sood and Vishnou Mourougavelou were also integral in the success of this study and manuscript.
References
Footnotes
Contributors Both authors fulfil the authorship criteria as per BMJ policy and contributed equally in terms of research, writing and editing.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests MJ is an intern at Medic Creations and RM works for Medic Creations. Medic Creations is the company that created Medic Bleep.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request.