Article Text

Abstract
Objective To describe unmet needs and values in stroke rehabilitation using the Health Value Framework and the associated coassessment tool Health Value Spider, a framework designed to identify and prioritise unmet needs based on health technology assessment (HTA).
Setting The study took place at Oslo University Hospital, Norway, from February to April 2019. Participants in three consecutive workshops were recruited from Sunnaas Rehabilitation Hospital, Oslo Municipality, Hospital Procurement Trust and Oslo University Hospital. Twenty-four hospital workers (medical and allied health staff and administrative staff) participated in workshop 1 and 29 patients, user representatives and hospital workers in workshop 2. Twenty-one patients and hospital workers participated in workshop 3.
Interventions Stakeholder analysis and scenario building was performed in a coassessment setting where unmet needs were identified applying the Health Value Framework. Two of the authors are also the developers of the Health Value Framework (KJK and LNS).
Results In the two first workshops where health workers, patients and next of kin perspectives were elicited, three needs were identified: patient insecurity in patient journey transitions, lack of stroke rehabilitation expertise in primary care and invisible patient problems, such as fatigue and cognitive impairment. In workshop 3, 12 opportunity areas were identified. Four opportunity areas were selected by the stakeholders based on a prioritisation process: early discovery of cognitive impairment, rehabilitation continuity, empowered patients and next of kin and remote monitoring and digital touchpoints.
Conclusion Health Value Spider successfully identified and prioritised unmet needs and described associated values.
- cardiovascular
- economics
- affordable
- accessible
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Summary box
What are the new findings?
The person-centred coassessment framework Health Value Framework was designed to help identify and prioritise unmet needs and is based on health technology assessment (HTA).
This study demonstrated that the Health Value Framework was feasible and can be used to identify stakeholder needs and opportunities corresponding to those needs.
From a health innovation perspective, the Health Value Framework was successfully applied in identifying and prioritising unmet needs.
How might it impact on healthcare in the future?
The Health Value Framework makes it possible to involve and pay attention to what is important to the patient at an early stage in the innovation process.
The Health Value Framework facilitates the early involvement of decision makers, considered important to increase the adoption and diffusion of quality improvements.
Introduction
Chronic illness represents a substantial burden on individuals and society but comes without a self-management recipe. Long-term conditions are estimated to take 70% of healthcare budgets.1 Globally, the top 10% of healthcare consumers account for two-thirds of all healthcare spending, and this top 10% is dominated by patients with complex long-term needs.1 2 Responding to the challenge of improving person-centred care, new, integrated care models need to improve patient experience and health outcomes at lower costs. Such models may require methods less familiar to healthcare like design thinking, including coassessment of person-centred needs and health value in integrated care services that is yet not developed. Integrated, person-centred care can be understood as what WHO defines as people-centred health services; what best serves patient needs, which means putting people and communities, not diseases, at the centre of health systems.3 This empowers people to take charge of their own health rather than being passive recipients of services. Evidence shows that health systems oriented around the needs of people and communities are more effective, cost less, improve health literacy and patient engagement and are better prepared to respond to health crises.3
The design approach has been highlighted as an important framework for innovation and improvement work.4 One reason is to involve and pay attention to what is important to the patient and facilitate self-management, another that it holds the promise of better and more cost-efficient care.3 5 For that purpose, it has been argued that patients and staff as codesigners of healthcare is an important resource improving the quality of care6 and that codesign practices should be embedded in healthcare organisations. Identifying the needs of patients is a prerequisite to provide patient-centred services, and routine collection of patient experience data alone is considered insufficient for this purpose.7
In addition to addressing patient needs when redesigning care, clinical, organisational and economic aspects also have a role. A recent literature review found stakeholder insight to be an important source of data in early assessment of potential health benefits.8 However, while qualitative methods is invaluable in enabling an understanding of unmet needs, economic assessments are needed to ensure that new services are justifiable in terms of the benefit it produce.9 A critical appraisal of the role of innovation in quality improvements emphasised the need to include decision makers in the innovation process to increase the adoption and diffusion rate.10 Decision makers need to understand how unmet needs can be addressed in a low-risk way. As part of a planning process, it is important to recognise risks and costs and assess the potential benefit. This includes the disruptive effects of even beneficial innovations,10 as healthcare improvements may generate additional capacity rather than savings.11 Due to fixed costs of a typical healthcare setting, quality improvements may not be cost saving unless attention is paid to the potential economic benefits.
Stroke constitutes one of our major societal challenges. Over 15 million people worldwide experience a stroke annually, with nearly one in four a recurrent stroke.12 It is the fourth leading cause of death and challenges the patient pathway in rehabilitation.13 A major bottleneck is the access to rehabilitation. Commissioning is the process of assessing needs, planning and prioritising, purchasing and monitoring health services to get the best health outcomes. Innovative commissioning is one tool for healthcare to acquire need-based, innovative and effective solutions. The hospital and municipality sector have joined forces, since this problem challenges the integration of care between the sectors. Sunnaas Rehabilitation Hospital and Oslo Municipality has, in collaboration with Oslo University Hospital, initiated an innovative commissioning project, where the aim is to identify and prioritise an unmet need and invite the health industry to supply products for testing.
The commissioning will be based on common rehabilitation needs, as defined and agreed on by patients, healthcare personnel and decision makers in each system. The EU Procurement Directive 2014/24 put into action in 2017 allows suppliers more freedom to suggest alternative solutions. This paper addresses the first part of the need specification process of an ongoing commissioning process for new stroke rehabilitation tool. Accordingly, the healthcare partners are setting out to pay for the development of a ‘technology product’ that is yet to be developed. The person-centred coassessment framework Health Value Framework was designed to help identify and prioritise unmet needs and is based on health technology assessment (HTA). The four domains, patient, clinical, organisational and economy, are key aspects considered by the tool. Our aim is to describe unmet needs and values in stroke rehabilitation using the Health value Framework and the associated coassessment tool Health Value Spider, as a person-centred coassessment framework for unmet needs that potentially may be solved by a new technology or service.
Methods
Framework
For this study, a person-centred coassessment framework was used to help identify and prioritise unmet needs (the Health Value Framework). The framework, developed to help identify and assess unmet needs, is based on HTA. HTA is defined as an interdisciplinary process for synthesising information regarding medical, social, economic and ethical issues related to the introduction of health technology.14 Early HTA evaluates technologies still in development and can be defined as the early examination of the medical, economic, social and ethical implications of a health intervention to determine the potential of its incremental value.15 16 To identify promising technologies early, new methods for early HTA are emerging in the literature.17 Based on a literature review on methods for early assessment18 and a stakeholder analysis of decision makers’ needs in a Nordic testbed project,19 a framework with four recommended evaluation domains was developed. The framework is inspired by HTA, design thinking4 and basic pathway management, and evaluates innovations under development. With person centred, the framework adheres to the definition of WHO people-centric services; what best serves patient needs, which means putting people and communities, not diseases, at the centre of health systems.3
The Health Value Framework has two features: a mapping function to identify unmet needs and areas of opportunity, and a coassessment tool for health value based on four domains designed to prioritise areas of opportunity (figures 1 and 2). The coassessment tool, named the Health Value Spider, was codeveloped in a workshop by service designers, health economists and physicians prior to this study, applying the four domains of the Health Value Framework.19

The four health value domains, description of each domain and its two belonging categories.

The coassessment tool the Health Value Spider.
Participants and setting
Three hospital partners expressed interest in using the Health Value Framework to describe unmet needs and values in stroke rehabilitation. The trial took place at Oslo University Hospital, Oslo, Norway, from February to April 2019, with describing unmet needs and values of stroke rehabilitation prior to a commissioning process as its main purpose. Three workshops were arranged to specify the needs of health partners (Sunnaas Rehabilitation Hospital, Oslo Municipality, Oslo University Hospital and Hospital Procurement Trust), patients and next of kin. In the first workshop, 24 health partner employees, including decision makers, participated. Twenty-nine representatives from health partners, user organisations, patients and next of kin participated in workshop 2. The third workshop was facilitated by innovation advisors from Oslo University Hospital and included 21 multidisciplinary stakeholders.
Participants were recruited from the following institutions: Sunnaas Rehabilitation Hospital, Oslo Municipality, Hospital Procurement Trust and Oslo University Hospital. Each institution included participants based on the eligibility criterion decided in the project. The eligibility criterion was that the participants belonged to one of the stakeholder groups in the field of stroke rehabilitation mentioned previously. There were no minimum numbers of participants from each site and stakeholder group, but a requirement that both medical and health professional, purchasers and decision makers at both primary care and specialist level should be represented in the workshops. Also, it was a prerequisite that patient representatives, next of kin and user groups participated in workshop 2.
Intervention
Figure 3 shows a flow chart of the study progression. Three workshops, with a duration of one workday each, were arranged to specify needs of health partners, patients and next of kind in the stroke commissioning process.
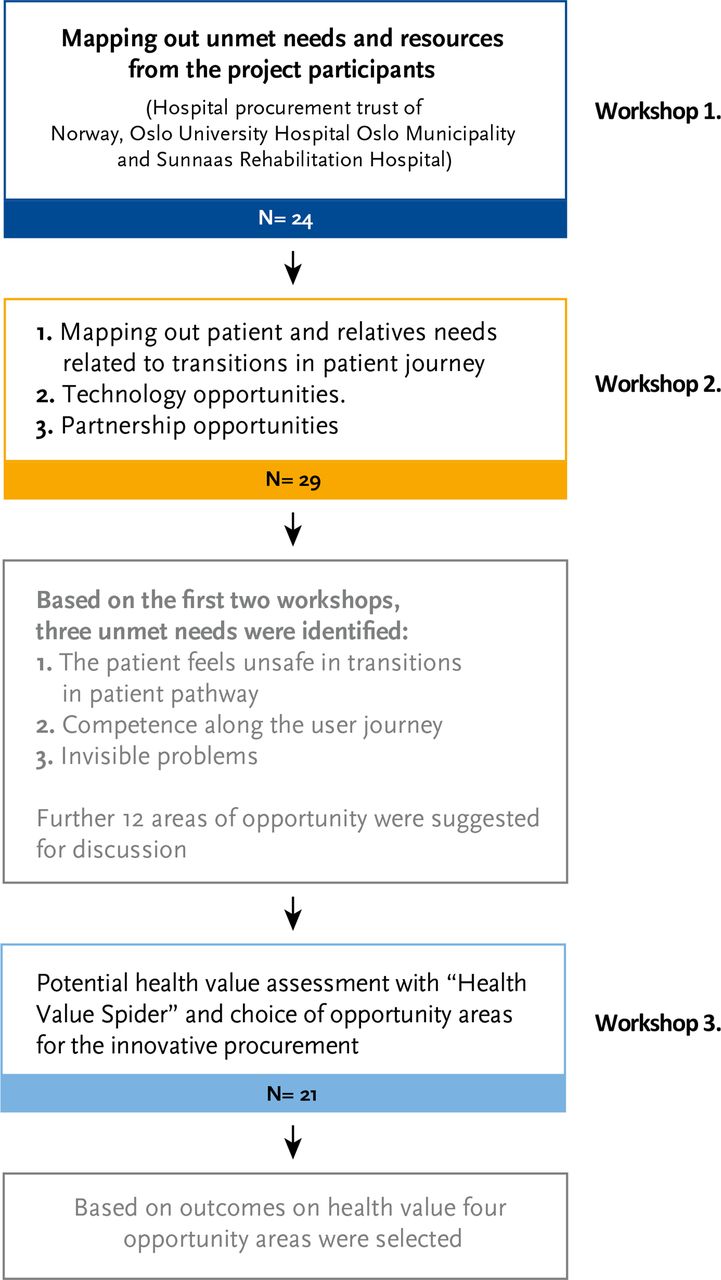
Flow chart of the study.
Workshop 1: mapping needs: the first workshop, conducted in April 2018, employed the mapping function of the Health Value Framework. The purpose of workshop 1 was to map out project partners’ unmet needs and resources. Oslo Municipality, Sunnaas Rehabilitation Hospital, Oslo University Hospital and the Hospital Procurement Trust of Norway, all government funded, participated. The workshop was facilitated by the project’s steering committee and was attended by 24 health partner employees, including multidisciplinary stroke care and rehabilitation teams. Using the mapping function of the Health Value Framework, participants were invited to brainstorm their unmet needs, such as identifying gaps in the patient pathway related to the various rehabilitation journey possibilities.
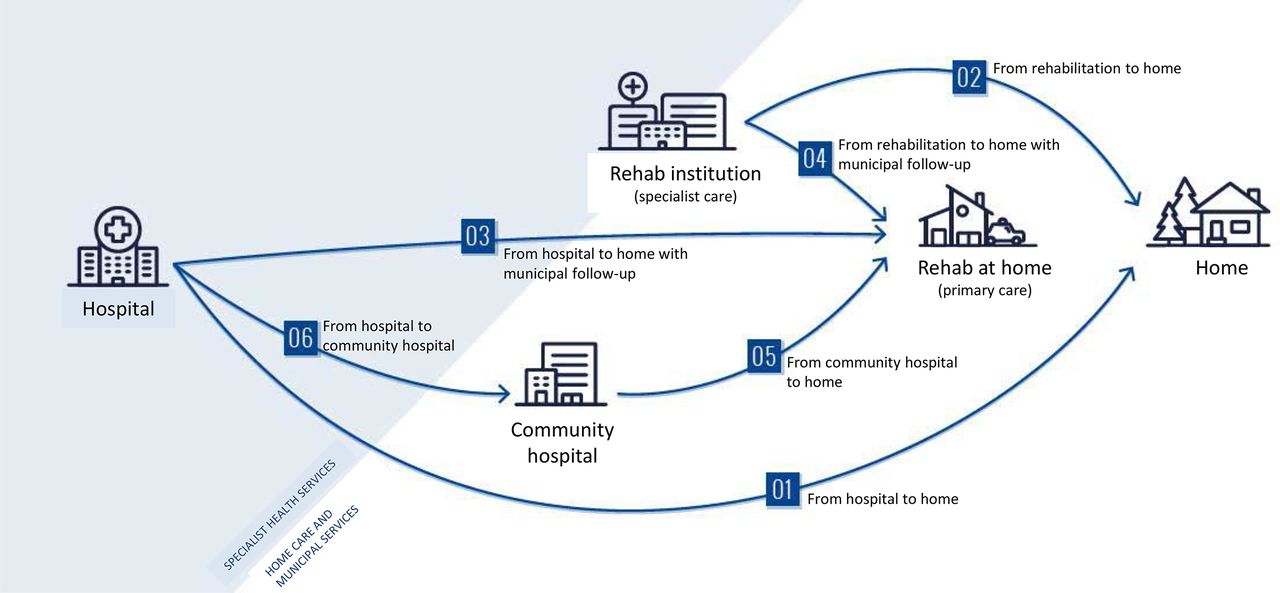
Workshop 2: mapping needs against patient journeys and identifying opportunities: the second workshop in April 2018 had three mapping purposes: the needs of patients and their relatives related to patient journey transitions, technology opportunities and partnership opportunities. This workshop was facilitated by the project steering committee. Twenty-nine representatives from health partners, user organisations, patients and next of kin participated in workshop 2. Healthcare personnel presented the summarised results from workshop 1. Scenario drafting was used to anticipate future developments in the field of stroke rehabilitation to identify opportunity areas of current practice. This process included ‘what if‘ scenarios with expert opinion feedback from users and healthcare personnel. Participants were then invited to nominate technology opportunities that matched unmet needs. For example, would increased digitalisation of health records resolve the need for rehabilitation in the patient pathway? Figure 4 shows the distribution of the three patient discharge opportunities following emergency treatment and the six transitions in the stroke patients’ journey where needs were identified in workshop 2.

Distribution of the three patient discharge opportunities following emergency treatment and the six transitions in the stroke patients’ journey where needs were identified in workshop 2.
Prioritisation: based on the first two workshops, the steering committee of the project, consisting of representatives from the two commissioning partners, Oslo Municipality and Sunnaas Rehabilitation Hospital, prioritised four opportunity areas in the final workshop. The Health Value Framework was used to prioritise the opportunity areas based on potential effects for users, economic and clinical aspects and the organisation.
Workshop 3: refining opportunities and assigning values: the third workshop used the coassessment tool, the Health Value Spider. The purpose of this final workshop was to provide detailed need specifications for the four priority areas and nominate values for each opportunity on the Health Value Spider. This workshop was facilitated by innovation advisors from Oslo University Hospital and included 21 multidisciplinary stakeholders, including decision makers, clinicians and the healthcare industry participated. In this workshop, the participants were allocated, depending on their professional expertise, to address either patient, organisational, economic or clinical opportunity areas (figure 1). The ‘Health Value Spider’ was displayed and value points were discussed until the group reached a consensus about where the value should be placed on each subscale.
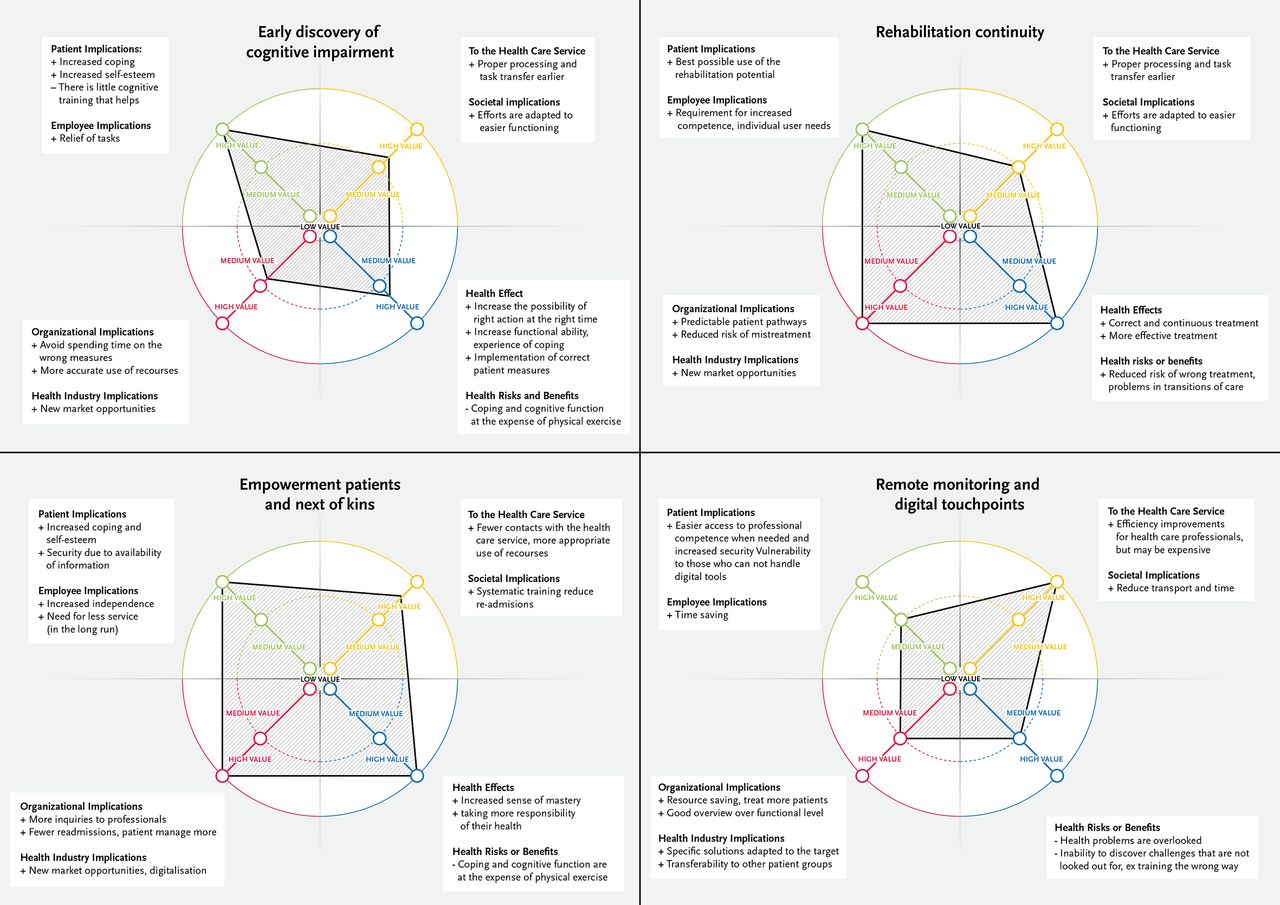
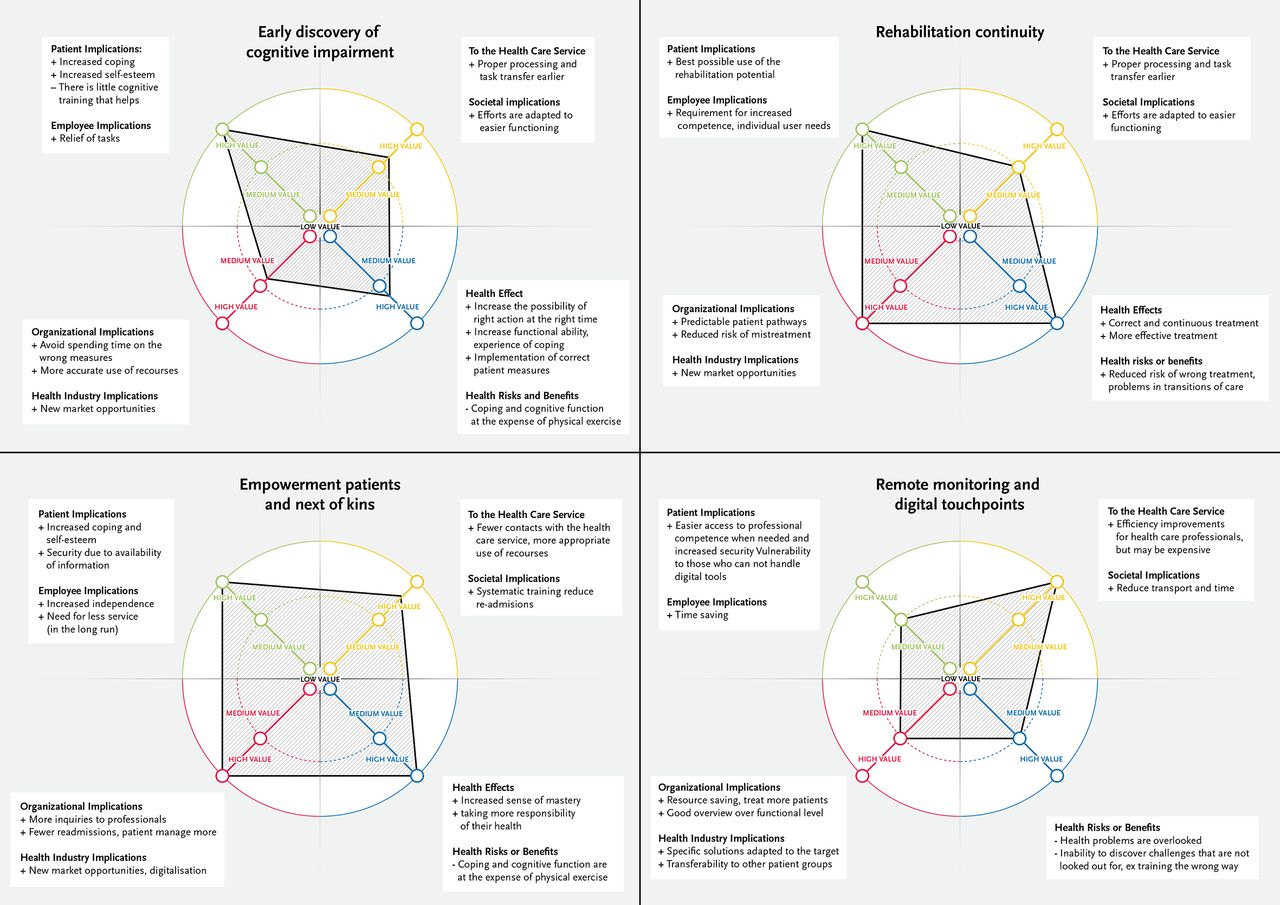
The Health Value Spider was applied to align stakeholders around quality improvements. Each stakeholder assessed the potential health value of each opportunity area identified in the first two workshops, applying the Health Value Spider. The opportunity areas were explored based on the four health value aspects in figure 1: patient (patient and employee implications), economic (to the healthcare service and to society), organisational (implications for the organisation and the health industry) and clinical (health effects and risks). Each domain was scored on a continuous scale marked from low to high value. The opportunity areas were prioritised based on the size of the Health Value Spider imprint (figure 5).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Distribution of the perceived value for each area of opportunity among the participants in the third workshop (n=21). In the figure, the four opportunity areas with the highest score are visualised.
Objectives and outcomes
The primary objective was to describe unmet needs and values in stroke rehabilitation using the coassessment framework for unmet needs in a commissioning process. Because the purpose of the Health Value Framework is person centred when coassessing unmet needs and opportunity areas, the tool’s ability to help describe needs and prioritise opportunity areas were selected as surrogate endpoints. Accordingly, agreement in the prioritised quality improvement areas was considered the most important success criterion.
Data analysis and ethical considerations
Excel 2010 was used for analyses. Stakeholder analysis and scenario drafting were used to identify the unmet needs. The Health Value Spider imprint was used to describe the potential health value of each opportunity area and provided input to the final tender specification.
Participants were informed that anonymised and aggregated data from the workshops would be used for research purposes. As such, no ethical considerations are necessary for this study as data sources are based on published articles, national statistics, expert opinion and aggregated qualitative data.
One of the stakeholders included in the study was also author of the study (KJK). The author was asked to contribute with her clinical expertise as a hospital physician in workshop 3, allocated to respond to clinical opportunity areas. She had no role in the prioritising or decision making of unmet needs that were solely made by the two commissioning institutional partners. Two of the authors of this article are also the developers of the Health Value Framework (KJK and LNS), with the associated Health Value Spider.
Results
Workshops 1 and 2: mapping needs and identifying opportunities to meet needs
Based on the first two workshops, three categories of unmet needs were identified: (1) the feeling of patient insecurity in patient journey transitions, (2) lack of stroke rehabilitation expertise throughout the user journey and (3) the stroke patients’ invisible problems. Examples of invisible problems were fatigue and cognitive impairment—problems that take a long time to uncover and that are especially challenging because it may be difficult to accept and to know how to relate to it. Currently, there is a lack of expertise and rehabilitation services to deal with these challenges when the patient has returned home and embarks on everyday life. Associated with the three defined needs, the following 12 areas of opportunity were proposed and discussed in the workshop by the participants: (1) early discovery of cognitive impairment, (2) rehabilitation continuity, (3) empowerment of patients and next of kins, (4) remote monitoring and digital touchpoints, (5) better coordinated rehabilitation transitions, (6) expertise along the user journey, (7) research expertise in all stages of the rehabilitation chain, (8) competence and support for relatives and the network around the patient, (9) available, adapted and updated information to patients and relatives, (10) cognitive training and support for patients, (11) identification of the patient’s invisible problems and (12) systematic patient and relative training and cochoice in rehabilitation.
Workshop 3: refining opportunities and assigning values
In the third workshop, these findings were further explored, refined and evaluated applying the Health Value Framework with the associated Health Value Spider. As step 1, 12 opportunity areas were assessed using the coassessment framework based on the following effect categories: patient and employee implications, healthcare service effects, social implications and organisational implications. Furthermore, the potential effect of each area of opportunity was assessed on a scale ranging from low, medium to high value. After each category received, a score of either low, medium or high based on significance of the written input of benefits and implications, an imprint was drawn. The size of the health value imprint gives a visual impression of its value. Figure 5 shows the detailing of potential evaluation outcomes of the four highest ranked opportunity areas in this study.
In step 2, the participants were asked to contribute to the prioritisation of opportunity areas based on their suitability for a tender process and the following commissioning process. An opt-out took place, where areas of opportunity not considered less suited or unsuitable for the tender process were marked with ‘red’ and ‘yellow’ Post-it notes. In a plenary session, the opportunity areas were visualised and discussed separately, while Post-it notes were added if new information was considered significant by the group.
Based on information from steps 1 and 2, the final choice of four opportunity areas to be refined for the upcoming tender was made by a decision-making group consisting of members from the three healthcare institutions: Oslo Municipality, Sunnaas Rehabilitation Hospital and Oslo University Hospital. Following the decision, a more detailed information was summed up based on information written directly on the value spider and the Post-it notes that were added during the plenary session. 'The annotations on figure 5 details the potential benefits identified. These figures can now be used to operationalise the tender specification.
Outcomes
Based on the Health Value Framework, four opportunity areas were recommended for further exploration prior to the upcoming tender process. The highest value opportunity area was found to be empowerment of patients and next of kins, followed by rehabilitation continuity, remote monitoring and digital touchpoints and early discovery of cognitive impairment.
Discussion
This study demonstrated that the Health Value Framework was feasible and can be used to identify stakeholder needs and opportunities corresponding to those needs. There was agreement among stakeholders that the four tender opportunity areas were satisfactorily identified. From a health innovation perspective, the Health Value Framework was successfully applied in identifying and prioritising unmet needs.
Patient-centred services may be easier to provide if patients are invited to a more direct and ongoing role in identifying, implementing and evaluating improvements.1 The approach to quality improvement and health innovations is traditionally based on unmet clinical needs and insufficient health supply. We believe the Health Value Framework is particularly helpful because the method seeks stakeholder consensus and addresses both patient and societal values at the same time. Traditional decision making rarely includes numerous stakeholders in a simultaneous decision-making process. The Health Value Framework directs both clinicians and healthcare decision makers’ initial attention to unmet patient needs and organisational aspects in addition to health outcomes and cost aspects.
In innovative commissioning, the translation of needs into functional specifications is crucial for the attractiveness to the dialogue with industry. This case study has addressed the first part of the need specification process of this ongoing commissioning process. In addition to identifying and prioritising unmet needs, the process revealed areas that will be expanded further in the next phase of refining the need specification in the final tender documents. The overall goal of the upcoming innovative commissioning process is to allow participating municipalities and hospitals to purchase solutions that help patients who had a stroke that are discharged from hospital or treatment institutions to continue to have a positive development in their rehabilitation even after returning home. The project group proposed a number of tasks to further explore the identified areas of opportunity: a systematic review of the research literature on stroke rehabilitation and a horizon scanning to identify technologies available in the market within the selected areas of opportunity. Furthermore, as the patient perspective may have been skewed because severely affected patients who had a stroke were unable to attend and therefore not invited, additional patient and next of kin interviews was suggested.
Codesign practices embedded in healthcare organisations provides an opportunity for patients, staff and decision makers to align on and prioritise user need and need specifications prior to tender processes. The Health Value Framework was successful aligning stakeholders around unmet stroke rehabilitation needs. Furthermore, the Health Value Spider identified unmet needs that were successfully prioritised among the stakeholders. Unfortunately, standardised inclusion criteria for which stakeholders should be included in such processes have yet to be reported in the literature. As such, generalisation of the identified stroke rehabilitation needs cannot be made. A strength of the Health Value Framework is, however, that it is based on HTA methodology designed to promote a multidisciplinary approach to evaluation and prioritising. Accordingly, the stakeholders included in the Health Value Framework represent a holistic perspective on healthcare needs in stroke rehabilitation.
Limitations and generalisability
Our study had several limitations. The participants may have been more motivated to enact behavioural change. The aim of the Health Value Framework was to initiate the specification and prioritising of unmet needs for the upcoming innovative commissioning, not for a comprehensive mapping of needs in patients who had a stroke. A number of areas will be further elaborated later in the commissioning process. Identification of unmet needs of patients and relatives is limited to user groups and user organisations able to attend the workshop. Patients admitted to health institutions were unable to attend the workshops. Mapping of unmet needs in patients admitted to the home without rehabilitation was not included, although this group represents one-third of the user group. The Health Value Framework mapping was limited to the unmet needs of users (patients and health professionals) familiar with and able to articulate challenges in a workshop. Also, since healthcare workers, patients, next of kin, user organisations and decision makers were part of the same workshop groups, this study does not provide participant group priorities, just consensus-based recommendations.
In view of the small sample, we are unable to comment on the generalisability of our findings in this case report. However, some interesting points emerged. In terms of user friendliness and evaluation of outcomes, the agreement that was reached in workshop 3 regarding the selection of opportunity areas suggests that the Health Value Framework was effective and efficient identifying and evaluating unmet needs. Furthermore, the hospital innovation advisors at Oslo University Hospital now have adopted the framework as an innovation support tool at Oslo University Hospital. Formal measures of satisfaction and perception data relating to the Health Value Framework/Spider were not collected, and this is an area for future potential research. It would be interesting to compare and contrast these data among key groups of stakeholders.
Future developments
Observation, interviews and other methods for mapping of needs may identify additional needs and provide a more thorough basis for the design and development process in collaboration with the project partners. A systematic review of the research literature on the impact of stroke and a technology study to identify what exists within the identified areas of opportunity should be provided in the next phase of the commissioning process. Furthermore, the continuous scale used to score the domains in the Health Value Spider, today ranked on three levels (low, medium and high), may benefit from being extended to more levels to ensure more precise evaluations. Finally, the Health Value Framework needs to be further validated through feasibility testing in various clinical settings and tender processes.
Acknowledgments
The author would like to thank all the participants in the workshops that made all the information on user needs and health values in stroke rehabilitation; participating patients and next of kin, patient organisations, representatives from the MedTech industry and healthcare workers representing Sunnas Rehabilitation Hospital, Oslo Municipality, Hospital Community Trust and Oslo University Hospital.
References
Footnotes
Contributors KJK, JR, MSB, FA, KR and ST have substantially contributed to the conception or design of the work or the acquisition of data. KJK and LNS have substantially contributed to the analysis and interpretation of data and to the draft of the work. All authors have been contributing to the critical revision for important intellectual content and final approval of the submitted version. All authors agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding This study was supported by the Norwegian research Council (grant number: 237766/030). This funding has enabled design of the study and collection, analysis and interpretation of data and in writing the manuscript.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The Regional Committee for Medical Research Ethics, Region Eastern Norway provided information that consent was not needed.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement No data are available. This is not a clinical trial, and there are no clinical data.