Article Text

Abstract
Background Mobile health (mHealth) can improve quality of care and empower cardiac patients. However, large-scale adoption is still lacking, as several challenges continue to be encountered in daily practice. We aimed to explore the mHealth experiences and challenges in cardiac patients, healthcare professionals, healthcare managers and information and communications technology (ICT) developers.
Methods A qualitative research was employed where semistructured interviews were conducted in patients, healthcare professionals, managers and ICT developers. We aimed to enrol participants of every stakeholder group, with diversity in sex, age group and occupation. Thematic analysis was used to identify themes reflecting experiences and challenges in mHealth in cardiac patients.
Results In total, 24 interviews were conducted in six patients, eight healthcare professionals, five managers and five ICT developers. Monitoring/care at home was reported as important advantage of mHealth (n=20, 83%). Patients valued increase of self-care (n=6, 100%) and remote reassurance (n=6, 100%), but reported medicalisation as important concern (n=4, 67%). Healthcare professionals warned for increased data burden (n=4, 50%). Managers agreed on the importance of device reliability (n=5, 100%) and ICT developers emphasised that the goal of mHealth is to replace care, rather than being supplementary (n=4, 80%). The majority of all participants (n=22, 92%) considered future use of mHealth as promising.
Conclusions All stakeholders foresee benefit of mHealth in cardiac patients, especially for remote care and reassurance. Frequently mentioned challenges included the need to replace care with mHealth, rather than adding more workload, and employing reliable devices and applications. If collaboration can be improved and group-specific challenges overcome, success of mHealth in cardiac patients can improve significantly.
- remote monitoring
- mHealth
- cardiology
This is an open access article distributed in accordance with the Creative Commons Attribution 4.0 Unported (CC BY 4.0) license, which permits others to copy, redistribute, remix, transform and build upon this work for any purpose, provided the original work is properly cited, a link to the licence is given, and indication of whether changes were made. See: https://creativecommons.org/licenses/by/4.0/.
Statistics from Altmetric.com
Introduction
Healthcare utilisation and costs have substantially increased worldwide in the last decades, due to increasing age of the world’s population with concomitant increasing prevalence of chronic diseases and advances in diagnostic and therapeutic options.1–4 These problems result in a growing need for medical and economical solutions. Mobile health (mHealth), a provision of targeted medical care through mobile technologies, is a recent and rapidly developing form of care, as the number of internet-connected mobile devices is currently over 25 billion.5 6 mHealth might improve care by enabling remote diagnosis and treatment, and reducing healthcare utilisation and costs.7–10 mHealth has been studied in cardiac patients to evaluate potential benefits and has shown promising results in several cardiac patient groups.11–16 Last year, a randomised controlled trial on mHealth in patients with heart failure demonstrated a significant reduction of all-cause mortality in patients assigned to the mHealth arm. This trial demonstrated that mHealth, when used in a selected patient group, can be successful in improving clinical outcomes, including mortality.11 Furthermore, in patients with paroxysmal atrial fibrillation (AF), mHealth provided rapid remote diagnosis of recurrences of AF through a telephone-transmitted EKG recorded at home, enabling rapid management of the episode and even preventing hospital visits.17
Thus, mHealth already demonstrated benefits for several cardiac patient groups. However, healthcare professionals are still hesitant to adopt mHealth in daily practice, which is also shown by the utilisation rate of telemonitoring that has remained unchanged over the past years in the Netherlands.18 19 Reimbursement, costs and resistance to change were identified as barriers for mHealth implementation worldwide, as well as a lack of integration of mHealth applications in the electronic medical record (EMR).20–22 However, with the current COVID-19 outbreak, the adaptation of mHealth seems to accelerate.23
Previous qualitative studies on experiences and challenges in mHealth have predominantly focused on healthcare professionals and patients, as these are the clinical stakeholders of mHealth.24–26 However, when experiences and challenges are not shared between clinical stakeholders and non-clinical stakeholders, this might result in a mismatch between design and use in daily clinical practice.27 To improve the success rates of mHealth, experiences and challenges of non-clinical stakeholders, including managers and information and communications technology (ICT) developers, should be explored.
Aim
We aimed to explore the experiences and challenges of all stakeholders using mHealth in cardiac patients: patients, healthcare professionals, managers and ICT developers, in order to provide key points of improvement for future mHealth programmes.
Materials and methods
Study design
A qualitative design was adopted and semistructured interviews were performed to explore the experiences and challenges of stakeholders most involved in using and adopting mHealth in daily practice: patients, healthcare professionals, managers and ICT developers in mHealth in cardiac patients.28 Semistructured interviews enabled the researchers to emphasise areas of interest while allowing participants to elaborate, providing richness of data. The local ethical committee issued a waiver that committee approval was not required for this study.
Participants
Participants were only eligible if they had been end users or developers of any mHealth application for cardiac patients. Participants could be both end user and developer. All patients who participated were enrolled in a Dutch telemonitoring programme, which monitored weight, blood pressure and heart rhythm.29 Cardiac patients who were currently or previously enrolled in the telemonitoring programme were identified through the outpatient clinic. We aimed to enrol equal numbers of cardiac patients, healthcare professionals, managers and ICT developers to provide an overarching view on experiences and challenges of all stakeholders involved in mHealth. Furthermore, through purposive sampling we aimed to get a broad perspective on the views of our stakeholder group by including participants of different sex, age groups and occupation. All participants were approached by means of email or telephone.
Interview guides
Before the interviews, a list of topics of interest, identified in the current literature, was assembled. The interview guide was pilot tested, reviewed, adapted iteratively during analysis and adjusted per group (online supplementary appendix 1). We aimed to prevent the interviewer from having a biased view on mHealth, as the interviewer was informed about the subject of mHealth, but had no previous experience using or developing mHealth. All participants were asked to elaborate on their personal experiences with mHealth: benefits, drawbacks and challenges. If they also had experience with the above-mentioned telemonitoring programme, they were then asked about their experiences with that programme. Finally, the participants were asked about their perspectives on the future use of mHealth.
Supplemental material
Data collection
Interviews were conducted in person or by telephone by a single researcher, a Masters student in medicine (PRH). The interviewer was not known to the participants. Prior to each interview, it was explained that the interviews were conducted in the context of a research project. At the start of each interview informed consent and approval to record the interview was obtained. All interviews were conducted in Dutch, and were audio recorded and transcribed verbatim. Transcribing was done using Amberscript software (Amberscript, Amsterdam, the Netherlands).
Data analysis
In this study, we used inductive coding for the analysis of the interviews, developing codes from the raw data.30 31 The analysis was done in multiple steps. First, the transcripts were analysed using open coding and a list of codes was compiled. During the study, these codes were evaluated through a process of ‘axial coding’ (identifying central themes and grouping codes in hierarchy). Finally, the transcripts were recoded using agreed-upon codes. Transcript coding was done using QDA Miner Lite V.2.0.5 (Provalis Research, Montreal, Canada).
Results
Participants
A total of 24 interviews were performed in six patients, eight healthcare professionals, five managers and five ICT developers. See table 1 for the characteristics of the participants. All invited participants for this study granted informed consent. The average duration per interview was 30 min.
Characteristics of participants
Through thematic analysis of the transcripts four main themes emerged, related to experiences and challenges in mHealth. A summary of these themes is displayed in box 1. In figure 1, the frequency of the four themes per subgroup is displayed to indicate the main interests per subgroup. In online supplementary figure 1, the frequency of each subtheme is displayed to illustrate what topics were discussed most frequently by all participants per theme from figure 1. Each theme is presented with supporting quotes, shown in online supplementary table 1. The most frequently mentioned benefits and drawbacks per subgroup are summarised in table 2.
Supplemental material
Summary of main themes with subthemes
Benefits of mobile health (mHealth) in cardiac patients:
Remote care.
Increases self-management.
Patient gains health insight.
Drawbacks of mHealth in cardiac patients:
Medicalisation.
Extensive communication required.
Keeping patients motivated.
Technical challenges:
Reliable devices.
Privacy and security of data.
User-friendliness.
Intercompatibility with electronic medical record (EMR) systems.
Policy and economical challenges:
Replacement of care rather than being supplementary.
Proper business model.
Governmental policies and regulations.
Extensive investments required.

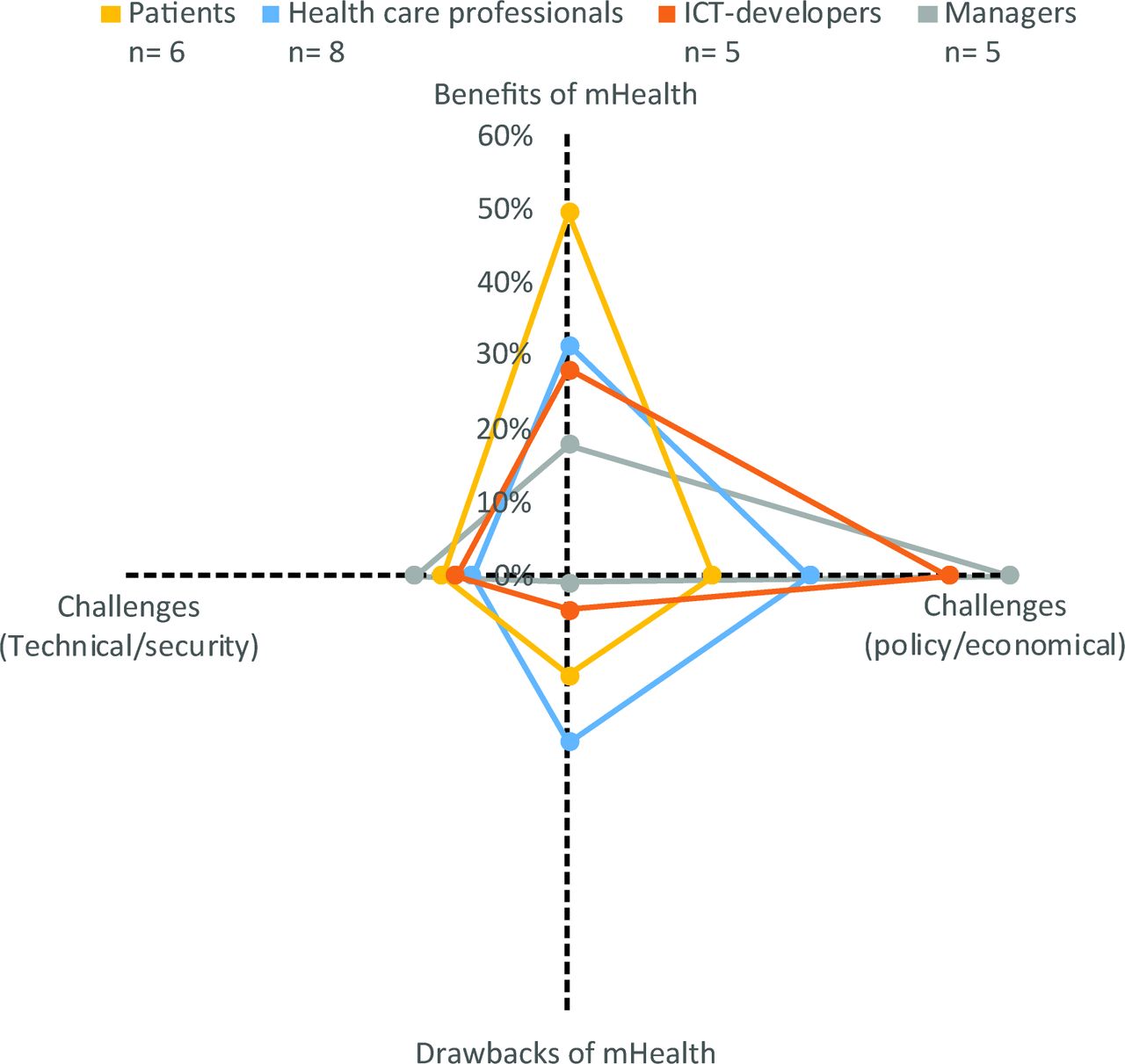{kind=link}
Frequency of themes per subgroup (% of total). ICT, information and communications technology; mHealth, mobile health.
Most important benefits and drawbacks of mHealth per subgroup
Benefits of mHealth
The majority of all participants (n=20, 83%) reported remote care as one of the most important benefits of mHealth. The ability to monitor patients between hospital visits and deliver care at the comfort of home was considered a major improvement compared with usual care (online supplementary table 1, 1.1). Mentioned examples were patients with hypertension, in whom mHealth enabled home monitoring of blood pressure, providing more data as well as enabling rapid treatment adjustments. Also, in patients with episodes of an irregular heartbeat, mHealth facilitated on-demand recordings of heart rhythm (online supplementary table 1, 1.2–1.4).
It is great, especially for arrhythmias, we have had great success with that. Patients usually consult the general practitioner, then they are referred to the cardiologist, who then performs a 24 hours Holter monitoring and finds nothing. With the help of mHealth they can now record an EKG during an episode of palpitations. (Healthcare professional 5)
All patients (n=6, 100%) reported increase of self-care as a major advantage of mHealth. Enabling patients to measure vital parameters at home and providing the results of these measurements to them, increased patient’s health insight and self-empowerment (online supplementary table 1, 1.5). Furthermore, all patients (n=6, 100%) reported remote reassurance as a large benefit of mHealth. To receive reassurance at home when symptoms were present was empowering to patients (online supplementary table 1, 1.6).
Healthcare professionals mentioned improvement of service for the patient as an important advantage of mHealth. They stated that delivering care at the comfort of home was a significant improvement for the patient. Managers added that care was no longer time and location dependent, making healthcare for chronic patients more scalable while also providing care when the patient really needed it (online supplementary table 1, 1.7–1.8).
The majority of all participants (n=22, 92%) considered future use of mHealth in cardiac patients to be promising.
Drawbacks of mHealth
Patients (n=4, 67%) mentioned medicalisation as pitfall for mHealth. They reported that performing measurements tended to confront patients with their health more frequently than in usual care, which could have had a negative impact on their mental well-being. Cardiac patients are currently used to visiting their cardiologist yearly and are sporadically confronted with their health in-between visits. However, when enrolled in an mHealth programme patients are confronted with their health daily or weekly as they evaluate vital parameters at home (online supplementary table 1, 2.1–2.2).
If you feel like you always have to be in control, you might get miserable from performing measurements. It might take over your life. (Patient 9)
Healthcare professionals (n=4, 50%) mentioned that all patient-generated data have to be analysed, to not miss clinically relevant events. This might result in an increase of workload. Healthcare professionals (n=6, 75%) also stressed the relevance of adequate instructions for patients enrolled in mHealth programmes. Patients, if not instructed properly, may assume that they are being monitored continuously, possibly preventing them from contacting emergency services in acute situations (online supplementary table 1, 2.3–2.5).
It generates a lot of data and also a lot of noise, which you are required to analyze to make sure there is nothing relevant you miss. That generates a lot of work. (Healthcare professional 2)
Furthermore, healthcare professionals (n=3, 38%) also mentioned that, for mHealth to be effective, adequate patient motivation and patient selection are required (online supplementary table 1, 2.6–2.7).
Technical challenges
Reliable devices, applications and software were mentioned by patients (n=5, 83%), healthcare professionals (n=5, 63%) and managers (n=5, 100%) as an important requirement for successful use of mHealth. Many participants argued that devices and software of adequate quality are already available and should thus be used (online supplementary table 1, 3.1).
It was stated by the majority of patients (n=4, 67%) and ICT developers (n=4, 80%) that user-friendliness of devices and applications is very important. It was mentioned that, as most patients will use the devices and applications for the first time, these should thus be easy to install and intuitive to use (online supplementary table 1, 3.2).
Patients of 70 years or older have more difficulty in handling new technologies, especially in the first few weeks. But it’s just like a new television, once you get used to it, it is fine. (ICT developer 22)
Privacy and security of patient-generated data was also an important challenge reported by patients (n=4, 67%), managers (n=4, 80%) and ICT developers (n=3, 60%). Many participants cautioned that privacy is an important issue and should be secured in every new mHealth programme (online supplementary table 1, 3.3).
Most ICT developers (n=4, 80%) stressed the importance of compatibility of mHealth interventions with current EMR systems. Integration of patient-generated data in the EMR was deemed important for the use in daily practice. Accessing these data should be easy and straightforward to encourage healthcare professionals to use it (online supplementary table 1, 3.4–3.5).
Economical and policy challenges
Interestingly, predominantly patients (n=4, 67%) and ICT developers (n=4, 80%) estimated that mHealth would reduce healthcare costs. Reduction of the number of hospital visits, through reassurance at home and early detection of deterioration, was mentioned as an explanation. Additionally, as a result of mHealth, patients were expected to generate less travel costs and by requiring less formal care, also diminishing the waiting list for the outpatient clinic (online supplementary table 1, 4.1–4.2).
The majority of healthcare professionals (n=7, 88%) and ICT developers (n=4, 80%) mentioned that new mHealth programmes should replace parts of usual care, rather than being an additional tool, in order to prevent an increase in healthcare costs and workload for healthcare professionals (online supplementary table 1, 4.3–4.6).
Eventually, it will be more work in the beginning, but it has to replace care. It should not be just an extra gadget. (Manager 15)
The majority of the managers (n=4, 80%) emphasised that an adequate business model should be employed. This implies cost-efficiency of the programme and the possibility to expand on large scale (online supplementary table 1, 4.7–4.8). Furthermore, managers mentioned a mismatch exists between available mHealth interventions (such as remote monitoring) and current governmental policies in regulating these mHealth interventions (n=4, 80%).
Finally, it was mentioned by managers (n=3, 60%) that healthcare professionals, when initiating an mHealth programme, are required to invest in the implementation of these programmes at the initial expense of their own revenues. As governmental policies are not yet fully established to compensate healthcare professionals for delivered care through mHealth, this is still a pressing issue for the success of mHealth. Managers addressed these issues and argued that this might be the reason why many healthcare professionals are still hesitant to start using mHealth (online supplementary table 1, 4.9–4.12).
Discussion
To our knowledge, this is the first study that explored the experiences and challenges in the use of mHealth in cardiac patients among all stakeholders involved in daily use and development: patients, healthcare professionals, managers and ICT developers. All stakeholders foresee benefit of the use of mHealth in cardiac patients, especially for remote care and reassurance.
Group-specific challenges were identified. Medicalisation of patients should be prevented and healthcare professionals should therefore pay special attention to patient selection.11 Healthcare professionals warn against data overload as all patient-generated data require analysis, interpretation and intervention if needed. This emphasises the need for a triage process, which is currently often provided by nurses or service companies.14 32 The use of computer algorithms as initial analysis of patient data is currently being studied.33 Moreover, our participants felt that to prevent work overload of healthcare professionals, the primary goal of mHealth interventions should be to replace care. mHealth interventions should be developed in consultation with healthcare professionals to prevent mismatch between design and daily use in clinical practice. Furthermore, as reliable devices and applications are abundantly available in the current digital era, careful evaluation should continue to ensure reliability.12
Another technical challenge that becomes increasingly important, as patients generate more data every day, and is mentioned by the majority of our participants, is data privacy and security, which is essential and even legally required for every new mHealth programme.34 The European law on privacy, the General Data Protection Regulation (GDPR, which came into force in May 2018), aims to ensure a high level of protection against misuse of personal data.35 Since mHealth is heavily dependent on the processing of health data, patients should be specifically informed about this data processing before giving consent. Both the healthcare professional and the company that delivers the mHealth structure have responsibility in securing adequate data protection for patients, which are explicated in the GDPR.
A new European legislation that will be applicable to mHealth initiatives is the Medical Device Regulation (MDR). Compared with current legislation, the MDR requires increased and transparent clinical evidence for certification of medical devices to ensure patient safety. In general, the riskier a medical device, the more complex the certification process.36 The MDR will be applied from May 2021, 1 year later than earlier planned due to the COVID-19 pandemic.
Adequate collaboration between stakeholders in mHealth in cardiac patients seems to be lacking and appears to be essential for successful implementation of mHealth in clinical practice.27 Previous studies focused on patients and healthcare professionals, the clinical stakeholders, which showed similar experiences compared with the experiences identified in this study.25 37–39 However, in our study we also identified important challenges for managers and ICT developers, including reimbursement, governmental regulations and other financial aspects of mHealth which were not mentioned such as the overall costs of monitoring programmes, which all have to be overcome in order to improve success.
This qualitative study describes the challenges in using mHealth, as described by our participants. Previous quantitative studies have shown that younger physicians were more willing to start using eHealth and that the age of the patients also affects the clinical decision-making of the physician.40 41 This could hold specifically true for mHealth as elder patients tend to struggle with mHealth.42 Personality of patients and its effect on health and outcomes is another consideration: type D personality is associated with higher mortality and poorer health status, while it was also demonstrated that the effect of telemonitoring was less beneficial in patients with a major depression.43–45 These are factors that should also be taken into account.
Strengths of this study include our broad sample of stakeholders and independent coding by two researchers. However, there are also some limitations. Our goal was to provide diverse opinions from the various stakeholder groups, thus we did not expect or attempt to reach data saturation. Therefore, we expect that some minority opinions are not represented in our data. All the interviews were conducted by a single researcher, which could have resulted in non-neutral questions. However, the interviewer received instructions in conducting unbiased interviews prior to the study. Participants might have been more willing to participate if their previous experiences with mHealth were positive, resulting in a possible response bias. Finally, eligible participants were chosen for their willingness to participate in research projects, possibly introducing a selection bias.
Conclusions
All stakeholders, especially patients, foresee benefit of the use of mHealth in cardiac patients, especially for remote care and reassurance. Frequently mentioned challenges by the stakeholders included the need to replace care with mHealth, rather than adding more workload to daily practice and employing reliable devices and applications. Close collaboration might be of great importance to successfully address group-specific challenges and to make future use of mHealth a success.
References
Footnotes
Twitter @marliesschijven
DK and PRH contributed equally.
Contributors DK, PRH, SKM, MACK, AAH, MPS, BJMM, BJB, MMW and MJS planned the study. PRH conducted the interviews. DK and PRH analysed the data. DK, PRH, SKM, EW, BJMM, BJB, MMW and MJS helped to report the study. DK submitted the study and is responsible for the overall content as guarantor.
Funding This work was supported by the Dutch Heart Foundation (grant number 2017 T2) and the Dutch Federation of University Medical Centers (NFU). The work described in this study was carried out in the context of the e‑Health Citrien programme. The e‑Health Citrien programme is part of and funded by the Dutch Federation of University Medical Centers (NFU).
Disclaimer The providers of the funding had no role in the study design, collection of the data, analysis or interpretation.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The local ethical committee issued a waiver that committee approval was not required for this study.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information.