Article Text

Statistics from Altmetric.com
Introduction
In September 2017, Médecins Sans Frontières (MSF) held a hackathon—a concentrated event that brings together various professionals and end users to build innovative solutions to challenges end users face in their work1—in Tokyo for 2 days. The event aimed (1) to identify new ideas to address challenges in humanitarian surgical care and (2) to deepen innovation networks in the humanitarian medical aid sector. This paper describes how MSF organised the hackathon and subsequently supported four projects launched at the event. The paper shares lessons learnt based on this experience for others holding hackathons with similar aims.
Challenge selection
To identify the challenges to tackle in the hackathon, we interviewed a range of surgical experts within MSF. Numerous challenges were raised. Following the Field Guide To Human-Centred Design, we tried and devised five possible solutions to each challenge in just a few minutes2: this tests their suitability for a hackathon-type event. We also narrowed the scope of our challenges by giving them a specific context while still trying to provide enough latitude for creative solutions to emerge.
Mentors and participants
MSF asked Japan Biodesign—a partner of the Stanford University Biodesign programme with trained leaders in innovating medical devices using design thinking principles3—to mentor participants. MSF surgical care experts also provided medical advice. Fifty-seven people, comprising medical professionals, engineers, developers, business people and students, were recruited mostly from MSF and Biodesign’s own networks. While several participants worked at medical device companies, all came representing themselves.
Group work
Mentors strongly encouraged participant groups to employ principles of design thinking. In contrast to more conventional hackathons,4 therefore, participants began the hackathon by thoroughly investigating and fully deconstructing their chosen problem and identifying the specific needs arising therein. Only then did they ideate solutions.
Awards
We employed three specific criteria to judge solutions: originality, impact and viability. Our four winning teams each received money for materials and technical and clinical advice. Furthermore, MSF and Japan Biodesign gave significant support to these teams to advance their projects further. However, as shown in table 1, after 2 years, none of the teams remain active. We return to this later.
Award-winning teams and their project status 2 years after the hackathon
Following up the award-winning teams
After the hackathon, members of winning teams worked on their projects as volunteers. Teams 1 and 4 met regularly and advanced their ideas significantly. Team 1 developed their specification for a headlamp and received generous support from a medium-sized enterprise to build a prototype. However, that prototype did not meet all necessary design criteria, and the team was unable to reiterate to overcome certain technological difficulties. Team 4, in contrast, dramatically reiterated to make their initial, highly sophisticated proposal more feasible for the contexts in which MSF works. However, the revised solution’s impact was too limited for MSF’s purposes. Team 4 did not reiterate the concept thereafter as the interest of the team diminished to continue working.
Team 2 held only one meeting. Around the same time, another company approached MSF and offered to adapt a similar existing product for MSF’s needs. MSF is pursuing this further; thus, MSF and team 2 decided not to continue their project.
Team 3, pushed mostly by one very motivated individual, elected to investigate their problem further by conducting a survey of MSF surgeons. That research found that improper use of different types of scissors might be damaging them. However, the team leader was reassigned within his company and was unable to continue managing this project. Lacking this leadership, the team disbanded; however, MSF continues to investigate these findings internally.
Lessons learnt
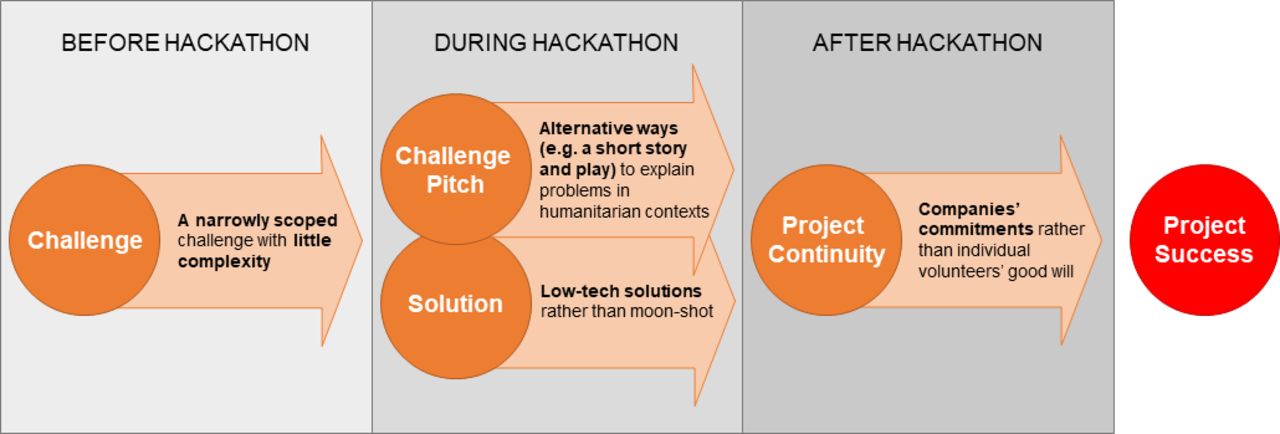
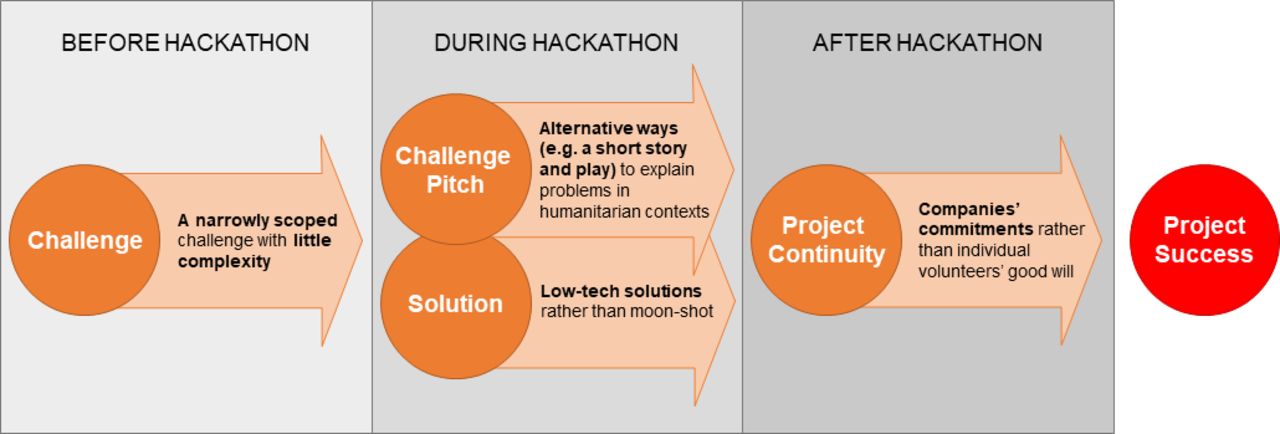
Our experience highlights four lessons learnt, which are described further in detail. Recommendations based on the lessons learnt are summarised in figure 1.
{kind=link}
Recommendations based on the lessons learnt.
Select appropriately scoped challenges
Commentators note that if a challenge is too broad and/or complex, hackathon participants struggle to narrow the scope sufficiently to enable them to start work.2 However, a challenge that is too specific will limit room to explore creative solutions.2 So what is the proper balance? For organisations that are relatively new to facilitating hackathons—like MSF—leaning towards a relatively narrow scope and low complexity appears advisable. ‘A way to provide an appropriate surgical headlamp for surgeons in humanitarian surgical care’, which team 1 chose to address, exemplifies this. Here, the narrow scope and low complexity fostered a rapid reiteration process that gave momentum to the project and thus ensured the continued engagement of the team. In contrast, ‘a way to enable MSF surgeons to obtain new skills to perform better and more types of surgery in the field’ proved too broad and difficult a challenge to scope down ahead of a thorough problem analysis within the hackathon’s time limits.
Find alternative ways to explain problems in humanitarian contexts
Participants’ general unfamiliarity with humanitarian medical work was a significant challenge to problem analysis. MSF has since experimented with alternative ways to explain the problems at the core of the challenges selected for the hackathon. At another event hosted by Japan Biodesign and MSF in June 2019, the core challenge was pitched within a short story and play.5 Such methods help participants without direct experience of humanitarian work to better understand the contexts in which their proposed solutions must function.
Feasibility versus desirability
Technological infeasibility is a common pitfall for projects conceived during a hackathon.6 Team 4 originally developed a so-called moon-shot concept. However, even after various attempts to adapt and simplify the proposal, the team members were unable to continue such a project on a voluntary basis. Even team 1, whose concept was much simpler, still faced technological challenges during the iteration phases that ultimately discouraged them from refining their prototype further.
The experiences of teams 1 and 4 indicate that technological feasibility should be assessed early and ideas refined accordingly with particular attention paid to the impact of such refinement on the effectiveness of the proposal. More generally, organisations with extremely limited capacity for product development projects—like MSF—should only consider proposals requiring minimal levels of this sort of investment.
Measures to consider for encouraging project continuation
MSF and Japan Biodesign offered significant posthackathon support to winning teams. While the importance of this is often stressed to encourage project continuation,7 the dissolution of all our winning teams before the end of their respective design processes suggests that follow-up support alone is insufficient. Two specific observations bear highlighting.
First, while the moon-shot proposal initially provoked a noticeably higher level of motivation among the team to continue work, that excitement appears to have been much more vulnerable to the realities of humanitarian work. As those realities forced reiterations that scaled back the ambition of the project, the interest of the team to continue working concurrently diminished, and the quality of their reiterations dropped. This again highlights the benefits of steering teams early towards technologically less-demanding solutions, which are more realistic in typical medical humanitarian contexts.
Second, it is worth inquiring into the interests of volunteers’ respective employers in the project their staff produced during the hackathon. This gives opportunity to negotiate a time commitment for which they may release their staff and even explore additional ways those employers might offer help. Employers, especially large companies, may be motivated by a corporate social responsibility policy, development of their human capital or opportunities to raise their own public profile.8 On the other hand, small-sized and medium-sized medical device companies may be motivated by finding a new business portfolio by a hackathon. Without such commitments, our experience again highlights the difficulties volunteers face to give sufficient time.
Conclusion
Our Hackathon for Humanitarian Surgical Care produced four interesting projects. We attribute that success to appropriately scoping most of our challenges, emphasising a narrower scope even at the cost of some creative latitude for problem solving. Committing significant posthackathon support to winners allowed the development of some of their ideas to continue for a good amount of time after the event. Nonetheless, all our teams ultimately stopped before reaching the end of their respective design processes. This suggests follow-up support alone is insufficient to achieve tangible solutions from hackathons. We suggest hackathon organisers should additionally steer participants away from technologically demanding solutions, as such moon-shots appear particularly complex to manage and progress with high risk of failure. Organisers should also try and secure a reliable time commitment for the subsequent volunteer work necessary to bring proposals to fruition. This may involve exploring the interests of winners’ respective employers in the continuation of winning projects.
Acknowledgments
We thank the hackathon participants for their dedication to the projects. We also thank Sally Moss (of Sally Moss Editorial) and Martin Searle for their excellent editorial support.
Footnotes
Contributors MK, FI, MY and SDC all contributed their ideas and reflections to write this article. All authors provided approval of the final submission.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.