Article Text

Abstract
The use of smartphones, mobile networks and associated health applications (known as apps) is now almost universal. Countries with low medical resources need assistance in their delivery of healthcare. This is particularly true where there are limited numbers of specialised physicians or nurses with respect to cancer screening. As smartphones become more universal, real-time and near-real-time expert medical consultations and telediagnosis are becoming more common. This leads us to believe that there will soon be a demand for mobile cancer screening services, which will be particularly useful for women living in rural areas or doctor-less inner city communities. The smartphone would seem to have almost limitless possibilities to address this need. As a first step in studying how cervical cancer screening using a smartphone could have widespread implementation, we conducted a pilot study to evaluate the utility of a smartphone to diagnose cervical intraepithelial neoplasm or invasive cervical cancer in 20 patients having an abnormal cervical cytology. Our results indicate that continuing progress in digital imaging devices may allow the quality of cervical cancer screening to be improved.
- Cervical cancer screening
- Cervical intraepithelial neoplasm
- Colposcopy
- Smartphone
- Tele-diagnosis
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
As of 2015, 43% of the world already owned a smartphone.1 Continuing progress in digital imaging devices may allow the quality assurance of cervical cancer screening to be improved. We conducted a pilot study to evaluate the utility of a smartphone for diagnosing cervical intraepithelial neoplasm (CIN) or invasive cancer.
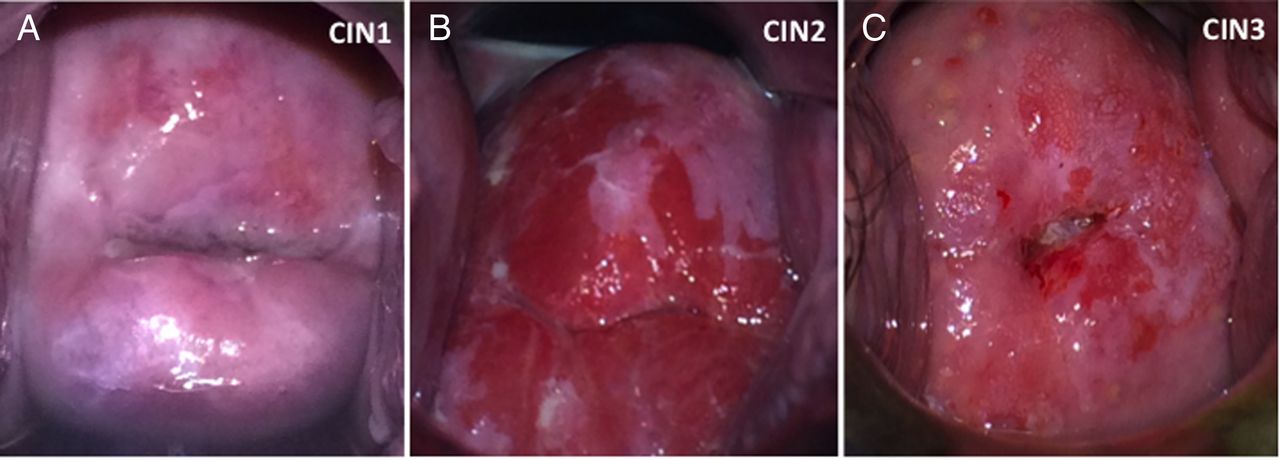
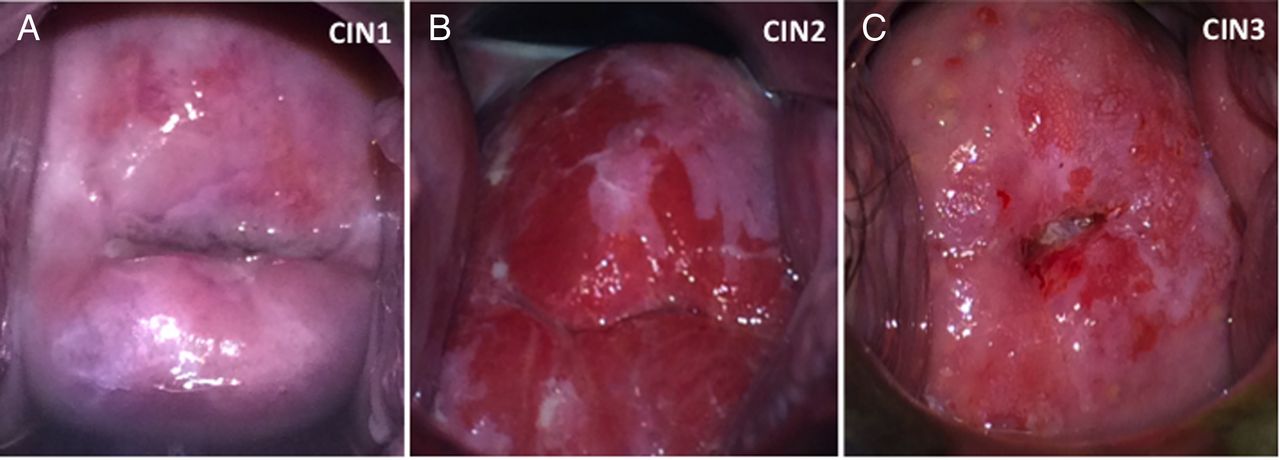
For our study, we used the iPhone 5S (Apple, California, USA) to inspect the uterine cervix of 20 patients with abnormal cervical cytology. The iPhone 5S has an 8 megapixels camera, with an aperture size of F2.2, focal length of 30 mm and a pixel size of 1.5 μm. For this purpose, we called the device, and its use as a cervical scope, a ‘Smartscopy’. The institutional review board of Osaka University Hospital approved the present study. A written informed consent was obtained from all patients. After the application of a 3% solution of acetic acid to the cervix for 1 min, a gynaecologist (Dr A) inspected the cervix using Smartscopy with the activated flash mode (figure 1). Dr A next captured still and moving pictures of the cervix. Dr A then recorded the most prominent areas of ‘smartscopically’ revealed abnormal epithelium. Subsequently, another gynaecologist (Dr B), who was not informed of the smartscopic findings, inspected the cervix of the same patient using traditional colposcopy (OCS-500; Olympus, Tokyo, Japan). Dr B then conducted a biopsy based on the colposcopic findings. The correlation between the smartscopic findings and the histological diagnosis was evaluated.
{kind=link}
Uterine cervix after application of the acetic acid, captured by the smartphone. (A) CIN1, note the acetowhite epithelium at 12 o'clock. (B) CIN2, note the acetowhite epithelium at 12 o'clock. (C) CIN3, note the acetowhite epithelium and mosaic at 1 o'clock.
Table 1 shows the results.
Characteristics of the 20 patients with abnormal cytology
The median age of the 20 patients was 39.5 years (range 26–49). The pathological diagnoses included CIN1 in 10 patients and CIN2+ in the remaining 10. In 17 of the 20 cases (85%), the CIN1+ could be diagnosed using Smartscopy (patients no. 1–11, 14–18 and 20). All 10 CIN2+ lesions could be detected using Smartscopy (patients no. 4, 5, 7, 9, 10 and 14–18). There were incongruities between the two approaches. For example, in the case of patient no. 12, the smartscopist noted that the most prominent smartscopic finding was acetowhite epithelium at the 9 o’clock position. However, the colposcopist did not perform a biopsy of this site; therefore, the pathological diagnosis of this site is unknown. In the case of patient no. 13, the colposcopy detected CIN1, as fine acetowhite epithelium at the 12 o'clock position, which was not detected by Smartscopy. In the case of patient no. 19, the histological diagnosis confirmed that the acetowhite epithelium at the 3 o'clock position noted by smartscopy was cervicitis. Our study also showed that video systems using a smartphone could be particularly useful for demonstrating the dynamic changes that occur in the cervical epithelium after application of acetic acid (shown in video 1).
Uterine cervix, 1 min after application of acetic acid. The smartphone revealed acetowhite epithelium throughout the entire transformation zone. The pathological diagnosis was CIN3 (9 and 12 o'clock).
The use of smartphones, mobile networks and associated health applications (known as apps) is now almost universal. Countries with low medical resources need added assistance in their delivery of modern healthcare. This is particularly true where there are limited numbers of specialised physicians or nurses with respect to cancer screening. As smartphones become more universal, real-time and near-real-time expert medical consultations and telediagnosis are becoming more common.2 This leads us to believe that there will soon be a demand for mobile cancer screening services, which will be particularly useful for women living in rural areas or doctor-less inner city communities. Smartphones would seem to have almost limitless possibilities to address this need for telemedicine. Further investigations will be required to confirm and improve the diagnostic capabilities of the smartphone.
Acknowledgments
The authors would like to thank Dr G S Buzard for his constructive critique and editing of our manuscript.
Footnotes
Contributors YT is responsible for manuscript writing. YU is responsible for study design and manuscript editing. AO is responsible for study design. MK is responsible for study design. SM is responsible for manuscript editing. EK is responsible for manuscript editing. KY is responsible for study design and manuscript editing. TK is responsible for study design and manuscript editing.
Competing interests None declared.
Patient consent Obtained.
Ethics approval Institutional Review Board.
Provenance and peer review Not commissioned; externally peer reviewed.