Article Text

Abstract
Introduction Contact tracing is an integral component of the overall public health strategy for controlling the outbreak of infectious diseases such as COVID-19. In addition to the conventional contact tracing, Qatar has implemented Ehteraz, a proximity-tracing mobile phone App using global positioning system and Bluetooth technologies. In this paper, we aim to evaluate the accuracy of Ehteraz as a contact tracing App based on the WHO contact tracing criteria and compare its effectiveness to the traditional human led case investigation.
Methods A cross-sectional study was conducted using two databases, including Ehteraz proximity data and swab collection and case investigations reports for the same period.
Results 46.9% of contacts identified by the Ehteraz app did not meet WHO duration and distance criteria. Among the 5650 contacts flagged by Ehteraz during the period, 4973 (88.0%) of contacts did not share any known relation with the index case they are linked to.
Conclusion The study highlighted the inaccuracy of the Ehteraz tool as its technology enables signals passing through walls, so people in different rooms could be unnecessarily flagged as having had contact. Big segments of the population (eg, Children) do not necessarily use smartphones and are not, therefore, flagged by Ehteraz digital contact tracing App. Similarly, Ehteraz rarely flags close contacts identified by human investigation as Bluetooth is usually turned off in a household or at a workplace. These findings highlight that digital contact tracing would be an efficient public health strategy when integrated to and complementing human investigation.
- COVID-19
- Public Health
- Environment and Public Health
Data availability statement
Data are available upon reasonable request. The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Summary box
What are the new findings?
Ehteraz Bluetooth technology-based contact tracing applications do not match the accuracy and targeted approach of conventional contact tracing methodologies.
One of the key characteristics of contact tracing is the timely identification of close contacts followed by the implementation of appropriate measures such as isolation, testing, quarantine. The delay of digital contact tracing methods in identifying close contacts has an adverse impact on the overall management of the COVID-19 outbreak.
How might it impact on healthcare in the future?
The integration of digital contact tracing with conventional intervention to fully benefit from available tools to curb the outbreak and to optimise the overall contact tracing strategy.
Community engagement should occur as early as possible in the design, adoption and use of a digital platform for contact tracing to ensure all the segments of the population and relevant parameters are taken into consideration.
Introduction
Contact tracing is an integral component of the overall public health strategy for controlling the outbreak of a highly infectious disease such as COVID-19. It is an essential part of epidemiologic investigation and active surveillance and is crucial in identifying the source of cases, containing them and preventing further spread of the virus.1 Number of countries, for example, Singapore, China, Taiwan and South Korea have developed digital contact tracing mobile apps that depend on various technologies such as Wi-Fi, QR Code, Bluetooth or global positioning system (GPS) to track the confirmed COVID-19 cases’ interaction with other individuals during the incubation period and to enforce self-isolation for patients and quarantine for close contacts.2–4
COVID-19 has shaken the way individuals and communities think, operate and live. The pandemic had considerable socioeconomic repercussions, which increased inequalities among vulnerable populations. It demonstrates the importance and needs to consider socioeconomic factors when implementing public health interventions and specifically new strategies of contact tracing to mitigate and alleviate the disparities in the impact of COVID-19 on distressed communities.5–7 During the different waves of the COVID-19 pandemic, Qatar has strategised and implemented restrictions to curb the virus spread through its COVID-19 Qatar National Response Action Plan.8 Widespread testing and regular screening had been executed and recommended by the health authority—as well as a comprehensive and traditional contact tracing strategy centred around the significant function of the investigation team. Contact tracing is the process of identifying and subsequently acquiring information from persons potentially exposed to infectious diseases.9 Through a process of interviews with the COVID-19 cases, the trained contact tracers and case investigators manage to locate and notify all persons identified as contacts with the infected person.10 If contact tracing is conducted rapidly, it can prevent onward transmission and mitigate further spread. Additional measures, such as electronic medical record (EMR) reviews, have been deployed for contact tracing in healthcare settings. These processes are crucial for stemming the spread of the infectious disease at the emergence of an outbreak.11
In addition to the conventional contact tracing to keep the epidemic under control, several nations, including Qatar, have implemented application-based contact tracing, aimed at flattening the curve of the virus.12 13 Digital contact tracing techniques typically depend on applications installed on smart mobile phones. These contact tracing apps trace individuals’ meet-ups by using different technologies for location tracking.14 The expected advantages of this technology over the traditional method of contact tracing include speed, specificity and mass reach.14 Moreover, several studies have been published illustrating the increased use of contact tracing and exposure notification application that can play an important function in a pandemic management strategy.15
Ehteraz is the Qatari proximity-tracing mobile phone App using GPS and Bluetooth technologies for the use of population living in Qatar, which was implemented in May 2020 to help flatten the curve of the COVID-19 pandemic. The application aims to assist in digitally tracking and notifying users of their interactions with potentially infected individuals and, thus, identifying disease transmission chains, alerting individuals and stakeholders to expedite the provision of medical support and prioritising testing.16
Objectives
In this paper, we aim to evaluate the accuracy of digital contact tracing app (Ehteraz) as a contact tracing app based on the WHO contact tracing criteria and to compare the effectiveness of Ehteraz with the traditional human-led case investigation. The findings may be used to explore challenges associated with the digital contact tracing solutions in terms of their methodologies and technologies.
Methodology
A quantitative cross-sectional study was conducted to analyse the effectiveness of the digital contact tracing app ‘Ehteraz’ during the first phase of its implementation. Ehteraz app uses a central server that enables the app to keep track of infected COVID-19 cases and notify individuals who are suspected to be exposed to a confirmed COVID-19 case through Bluetooth signal exchange between two mobile devices in proximity.
The study collected the data through two databases that were made available from Qatar Health Authorities, including Ehteraz app proximity reports for 1–10 July 2020, and the data available from swab collection and case investigation reports for the same period. All laboratory-tested positive COVID-19 cases during the aforementioned period and close contacts of the laboratory-tested positive COVID-19 patients during the same period were included in the study.
WHO defines a contact as anyone exposed to COVID-19 cases, 2 days before or 14 days afterward. The exposure is confirmed if the contact has interacted within a proximity of 1 m and for more than 15 min with the positive COVID-19 case. Contacts could also have provided direct care for COVID-19 patients without personal protective equipment or could be sharing the same household or a close confined space with the infected person—for instance, a workplace or nursing home.17
The nationality of tested individuals was established based on the official identification state card, the card is issued for all the residents and nationals in Qatar. Demographic characteristics were derived from their EMRs. The available employer details or guardian details refer to the different types of residency visa available in Qatar: The Work Residence Permit where employer is identified, the Family Residence Visa available to the immediate family of resident who has a Work Residence Permit, or, if Qatari, the name of the guardian or spouse. The age of the tested persons was categorised into five age-groups (<15; 15–24, 25–44, 45–64 and ≥65).
The compiled data extract was imported into STATA V.15.1—(StataCorp. 2017. College Station, Texas). The aggregated data set based on the above mapped data sources included specificities for each method on:
Number of index cases.
Number of positive cases.
Number of contacts.
Cases and contacts demographics.
Reporting date.
Swabbing date.
National address.
Employers’/guardians’ details.
The study was approved by the scientific research committee of Primary Health Care Corporation—Qatar under the reference number PHCC/DCR/2020/12/149.
Results
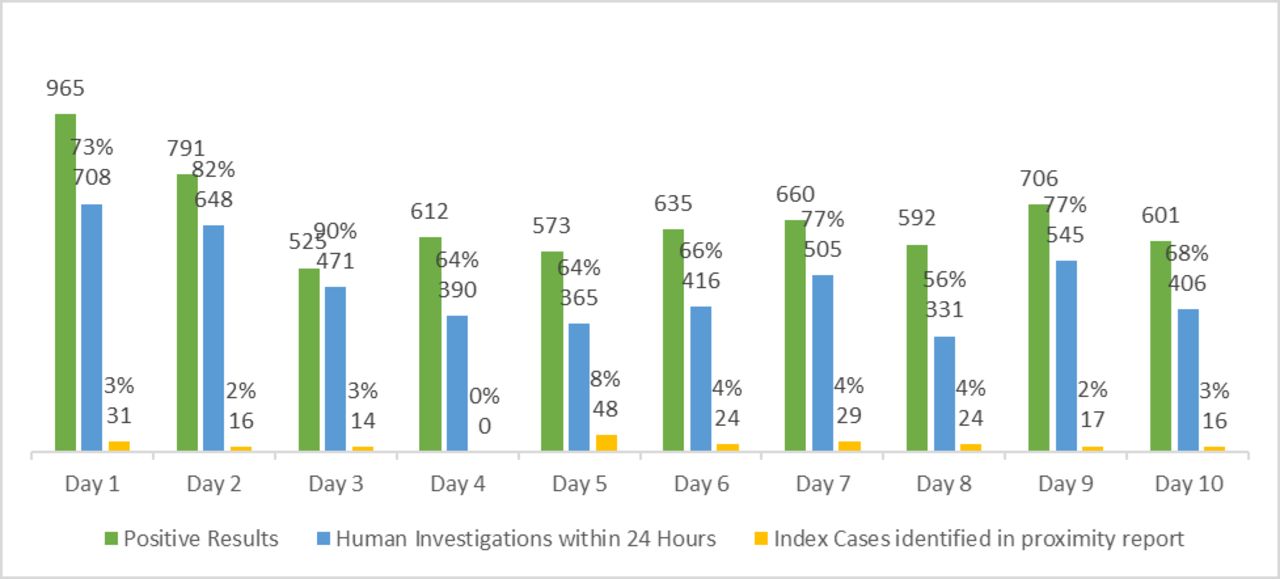
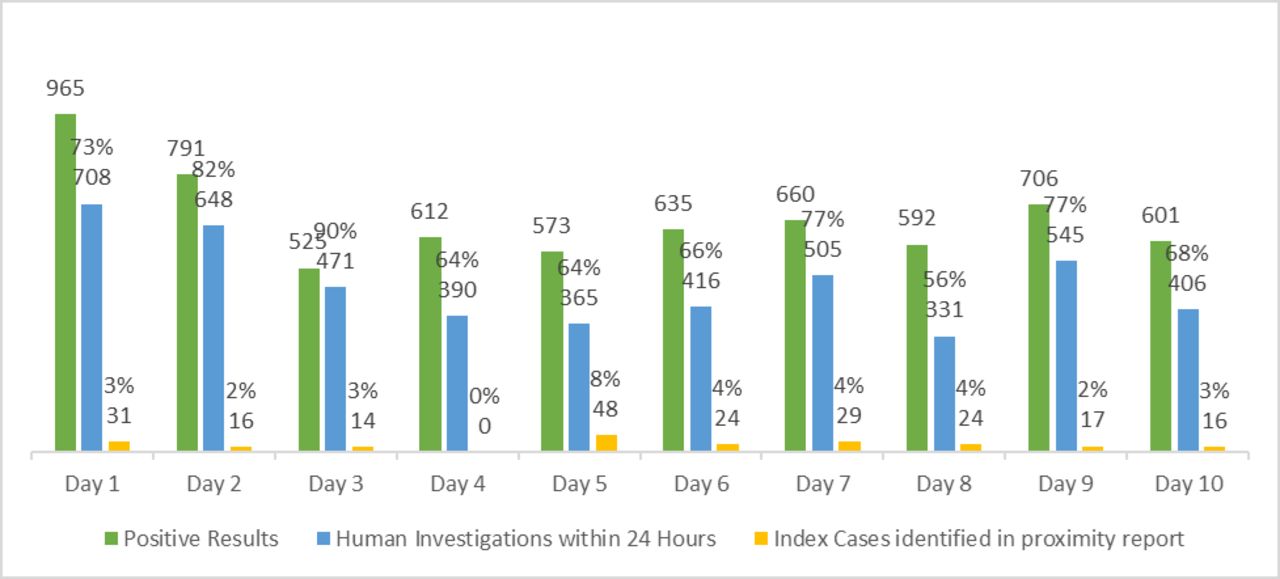
During the period ranging from 1 to 10 July 2020, a total of 6660 positive cases were investigated by the Contact Tracing Team. During that same period, 219 index cases were flagged in the Ehteraz proximity reports with a total of 5650 identified contacts. This shows an average daily Ehteraz detection rate of 3.3% (0%–8.4%) (figure 1).

Overview of positive cases detected, human investigation responsiveness in 24 hours and proportion identified as index cases by Ehteraz app.
Out of the 5650 contacts flagged by Ehteraz during the period, 2650 (46.9%) contacts identified by the Ehteraz app did not meet WHO duration and distance criteria (table 1), which define a contact as anyone with the following exposures to a COVID-19 case, being within 1 m of a COVID-19 case for >15 min.
Percentage of Ehteraz accuracy against WHO duration and distance criteria for COVID-19 contact and the categories of the contacts
Among the 5650 contacts flagged by Ehteraz during the period, 319 (5.65%) were identified in the contact-tracing swab collection reports. Furthermore, 677 (12.0%) had one of the below relations with their index case (table 1): 339 (6.0%) share the same residential address, 435 (7.7%) same employer/guardian and 270 (4.8%) work for the same company.
The remaining 4973 (88.0%) of contacts did not share any known relation with the index case they are linked to.
Figure 2 highlights the age distribution of contacts for both human investigation and Ehteraz app investigation taking into consideration different age brackets. The positive case responsiveness has also been reported. Out of the 6 660 COVID-19-positive cases during the period 1 July to 10 July, 71.8% of the cases (4785) were investigated by human case investigation within 24 hours. Out of the 219 Ehteraz-positive index cases during the same period, the average Ehteraz reporting delay varies between an average of 1.3 and 3.3 days.
{kind=link}
{kind=link}
Age distribution of contacts for Ehteraz application and human investigation.
The difference between the two is considerable with the near absence of children younger than 15 years of age (0.63%) from the Ehteraz app reports, whereas they represent 28.5% of the human investigation contacts. The disparity is less significant with regards to elderly people 65 years of age and above, but here again the human investigation seems to identify a little more than double of elderly contacts than Ehteraz with 3.3% against 1.50%, respectively. The age range 25–44 represents more than two-thirds of Ehteraz contacts.
Discussion
Among the most critical public health strategies in managing the COVID-19 is notification of potentially infected individuals and the rapid contact tracing—Qatar has used both digital and conventional contact tracing tools to diminish COVID-19 propagation in the community.
The study revealed that the digital tool Ehteraz does not consistently follow the WHO Contact Tracing logic for all its identified contacts, with almost half of the contacts flagged by Ehteraz not fitting the WHO duration and distance criteria, which may be attributed to Bluetooth technology for which the range is much greater than 1.5 m.18 This proximity inaccuracy of Bluetooth Technology has been addressed as a main technical challenge for contact tracing apps used in the pandemic.3 This highlights the uncertainty in the detection range of the app, opposed to human contact tracing, which is based on thorough investigation, aiming at identifying close contacts based on WHO case definition. It is important to highlight that the app can only report the proximity status, that is, when two devices are in communication range, regardless of where their owners are and what is in between such as glass or wall, which is totally different from the definition of contact tracing.19
Furthermore, several studies agreed that the range of Bluetooth can vary greatly depending on how people hold their phones and whether they are indoors or outdoors. Signals pass through walls, so people in different rooms could be unnecessarily flagged as having had contact. The result could be a flood of false positives.20 21
In a paper providing an analysis of digital contact tracing solutions in terms of their methodologies and technologies, Bluetooth technology is considered unreliable for distance estimation. This fallibility can lead to false alerts of an infection risk despite contacts being separated by a wall, or on the contrary, it can induce a false level of security even in the proximity of an infected individual who is either not using the application now or if the proximity-based sensing fails to register the contact.14
Similarly, only 5.7% of flagged Ehteraz app contacts were defined as close contacts by the public health investigation team. It seems that Ehteraz app rarely flags close contacts and can be explained because Bluetooth is usually turned off in a household, at a workplace, and Ehteraz app will only likely be activated where and when mandatory. Some contacts do not always have smartphones (ie, domestic helpers, elderly) and children below 18 years old are very rarely detected as contacts by the app and, thus, are automatically excluded. Digital contact tracing is, therefore, missing out significant segments of the population, who represent a major contact tracing focus in human investigation as the outbreak of the virus had reached the community spread level.22
Distinctly, human investigation contact tracing conducts a focused approach investigation and makes a point to ask about close contacts at home, namely, spouses, children and elderly relatives. A study showed that household contact was the main setting for transmission of COVID-19, and the risk for transmission of COVID-19 among close contacts increased with the severity of index cases.23 Human investigation will focus primarily on human social and demographic interactions by initially identifying close contacts as a family, followed by close professional daily encounters at the workplace.
Ehteraz seems to flag more people between the age range 25–44: this could be explained knowing that this age range represents the vast majority of the active population who will be more likely to have a mandatory active Ehteraz App although for a short period of time, at checkpoints or any other mandatory locations. This once again highlights the fact that Ehteraz relies only on a proximity tracking system without taking into consideration other aspects of social behaviour and human interactions, whereas effective contact tracing depends closely on how quickly, broadly, and accurately the contact tracing process is.
Duration or proximity by themselves does not represent a complete assessment of exposure since exposure may vary independently of proximity, such as being in an enclosed or an outdoor space and being protected or not wearing any protection.24 A case–control study in Thailand conducted on 211 patients with COVID-19 provided evidence supporting consistent mask-wearing, handwashing and adhering to social distancing recommendations to reduce COVID-19 or SARS-CoV-2 transmission in public gatherings.25
It is crucial to minimise delays in diagnostics, contact determination and detection as well as the subsequent isolation of all possibly infected individuals.26 In the present study, Ehteraz App showed a contact tracing delay of up to 3 days. A previous study evaluated the impact of the contact tracing delay on controlling COVID-19 pandemic and showed that when testing delay is 3 days or longer, even the most efficient strategy cannot achieve RCTS values < 1.27
The human case investigator conducts a direct phone interview with the positive case based on WHO’s very detailed case investigation form and identifies the positive-case close contacts. In addition, the contact tracing team do a complementary check at the swabbing location if there are any additional contacts not previously listed by the case investigator.28 All close contacts identified would undertake home quarantine for 14 days, including asymptomatic persons. In this way, contact tracing could prevent presymptomatic transmission. Satisfactory timelines are pivotal to the successful implementation of contact tracing as a control measure, as shown in previous modelling studies.
By flagging probable lower risk encounters and missing a substantive fraction of transmission events, Ehteraz app is unable to act like human contact tracing, which is an intensive process of interviews and investigator work, aiming at identifying solely real contacts that share the same house of the positive case or have been working together. One of the gold standard characteristics of an effective, high-quality contact tracing system for COVID-19 is the fast responsiveness and the identification of contacts in a timely manner, ideally, within 24 hours. Ehteraz app does not seem to satisfy this parameter, unlike human investigator. The only disadvantage of the human-led contact tracing method is that it greatly depends on the information collected from the confirmed cases and their willingness to disclose the information about who they met, at which time and at what location.3
The current study has some limitations that should be addressed. The study tests only one function of that application. Ehteraz app at the time of the study had just been deployed as contact tracing tool by health authorities and has currently been enhanced in terms of functions and capabilities to include quarantine and vaccination status. Ehteraz app has, for example, complemented human efforts through control of compliance with quarantine and isolation procedures and guidelines. Also, it is considered as vaccine passport for the people living in Qatar.
Despite these limitations, the used databases and cumulative records included all positive and investigated cases in Qatar during the time period of the study and, thus, offered a representative picture of the contact coverage and delay that might affect the containment of the transmission in Qatar.
In conclusion, these findings highlight that human investigation remains an essential tool of Qatar’s public health strategy that can identify most of the COVID-19 close contacts in a thorough and timely manner. Ehteraz contact tracing application showed some limits in identifying some important contacts, such as children and elderly individuals, in addition to the delay observed in tracing other contacts. Ehteraz technology should be integrated and complemented the conventional contact tracing to enhance Qatar Public Health’s efficacy in preventing and monitoring the COVID-19 infectious disease outbreak.
Data availability statement
Data are available upon reasonable request. The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statements
Patient consent for publication
Acknowledgments
We acknowledge Primary Healthcare Corporation Qatar as funding agency of this study.
References
Footnotes
Contributors Corresponding author, SS ensured all listed authors have approved the manuscript before submission. MGA-K acted as guarantor and conceived the study and oversaw overall direction and planning. JA and JMG and HEAR extracted and analysed the data. MGA-K, SS and AAAN analysed and interpreted the data. MGA-K, SS and AAAN and HEAR suggested the different points for the discussion section. MGA-K, AAAN, and SS were major contributors in writing the manuscript. All authors discussed the results and contributed to the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.