Article Text

Abstract
Background Nigeria, the most populous country in Africa, is faced with several health challenges including neglected tropical diseases, non-communicable diseases and emerging infectious diseases. Unfortunately, the country has a weak health system to tackle these health challenges. Creative solutions for solving these systemic health challenges through social innovations are therefore needed in Nigeria. Hence, Social Innovation in Health Initiative (SIHI) Nigeria conducted a pilot crowdsourcing challenge to identify social innovation solutions in Anambra State, Nigeria.
Method A crowdsourcing approach was used to identify social innovations in healthcare delivery that has been applied in Nigeria for a minimum of 1 year. The six-stage process of the crowdsourcing challenge contest included: (1) selection of challenge focus, (2) organising community steering group, (3) engaging the community to contribute, (4) receiving and evaluating contributions, (5) recognising finalists and (6) sharing solutions. The crowdsourcing challenge was hosted by SIHI Nigeria, based at the Nnamdi Azikiwe University, Awka, Nigeria.
Result Seventeen innovations were received in the crowdsourcing challenge. Five of the innovations were eligible based on criteria developed and were sent to the panel of experts for review. Following the review of the average score and case study research, the panel of experts selected top three innovations, which included a digital health solution, a mobile clinic and a community-based health insurance programme.
Conclusion Top three social innovations were identified in the crowdsourcing challenge. These innovations could be refined and scaled up to increase universal health coverage in Nigeria by subjecting them to further research.
- Public Health
- Primary Healthcare
- Delivery of Health Care
Data availability statement
Data are available upon reasonable request. The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution 4.0 Unported (CC BY 4.0) license, which permits others to copy, redistribute, remix, transform and build upon this work for any purpose, provided the original work is properly cited, a link to the licence is given, and indication of whether changes were made. See: https://creativecommons.org/licenses/by/4.0/.
Statistics from Altmetric.com
What are the new findings?
The practical application of crowdsourcing in the Nigerian context led to the identification of several homegrown healthcare solutions.
The entire crowdsourcing process led to the selection of a digital health solution, a mobile clinic and a community-based health insurance programme.
These solutions characteristically engaged the local population/beneficiaries with the aim of improving the access to and quality of healthcare received.
How might it impact on healthcare in the future?
The crowdsourcing challenge provides a unique opportunity for the Nigerian healthcare sector to identify and support the upscaling of healthcare solutions that engage the population at the grassroots level.
Introduction
Nigeria is the most populous country in Africa with over 200 million people. The country is faced with several health challenges including neglected tropical diseases, non-communicable diseases and emerging infectious diseases. Unfortunately, with a weak health system, the country will be unable to tackle these health challenges. For instance, only 20% of primary healthcare facilities are functional in Nigeria.1 The functional facilities are not only readily inaccessible but are also saddled with a large number of patients at the doctor–patient ratio of 1 doctor to 2500 patients.2 This has resulted in poor health outcomes with under-5 mortality as high as 119 per 1000 live births, while maternal mortality is as high as 814 per 100 000 live births. Consequently, Nigeria ranks among the countries with the lowest life expectancy with an average life expectancy of 54.3 years.3
The Nigerian healthcare system favours a top-bottom or verticalised approach to healthcare delivery in Nigeria. This is distributed into three levels—federal, state and local government. The Federal Ministry of Health is responsible for policy formulation and provision of technical support to the overall health system, handling international relations on health matters, managing the national information system, and providing health services through the tertiary and teaching hospitals and national laboratories. The State Ministries of Health (SMOHs) manage the secondary hospitals as well as regulate and provide technical support for primary healthcare services. The local governments manage the primary healthcare centres instituted in each ward. Each local government is subdivided into 7–15 wards. In addition, there are multiple vertical programmes such as the HIV programme, Neglected Tropical Diseases Eradication Programme, etc that are run by government partners and non-governmental organisations. Although the organisation of the Nigerian healthcare system appears synchronised, its practical functioning is not seamless with duplication and confusion of roles and responsibilities among the different levels of government. The Nigerian healthcare system has been described as poorly developed and lacks functional surveillance and medical intelligence systems typical of the modern health sector.4 In the current scenario, healthcare does not reach the majority of Nigerians particularly those in the lower socioeconomic status and hard-to-reach areas. Very few of the populace (3%) are health insured and government provision for health is insignificant (ie, 3.89% of Nigeria’s gross domestic product).5 6 Huge out-of-pocket payments for healthcare are non-affordable or catastrophic for many households as over half of Nigeria’s population lives on less than $1.90 a day.7
To address the challenges associated with the top-down approach, there are growing interests of bottom-up approaches which can be identified by crowdsourcing. Crowdsourcing is a term used to indicate the identification of relevant information from individuals and groups, therefore leveraging on the bottom-up crowd-derived inputs.8 This has resulted in identification of several social innovations across lower middle-income countries in Africa such as the Last Mile Health in Liberia, Kaundu Community-based Insurance in Malawi, among others.9 With the application of the crowdsourcing approach, the Social Innovation in Health Initiative (SIHI) Nigeria hub aims to change the current narrative by approaching healthcare delivery through a new lens. SIHI Nigeria searches for creative solutions to systemic health challenges developed through social innovations and applied to reach vulnerable populations in communities.10 After identifying these innovations, the hub will work towards increasing uptake through further research to establish their effectiveness, understand their implementation challenges and position them for scale-up. SIHI Nigeria engages communities, government’s representatives and other stakeholders within and outside the health system throughout the identification process and in scaling up delivery of these social innovations and increasing their uptake.
A report of the crowdsourcing challenge with the aim of identifying creative, effective, inclusive and affordable healthcare solutions, conducted in Anambra State, Nigeria, is here presented.
Methods
Study area
In April 2020, the WHO awarded a grant to Nnamdi Azikiwe University, Nigeria and School of Public Health, University of Ghana (both new generation hubs) to collaborate with Makerere University, Uganda (a first-generation hub) to disseminate social innovation in health in Africa. Through the grant, SIHI Nigeria based at Nnamdi Azikiwe University conducted two crowdsourcing challenges (pilot and national) to identify social innovation solutions in Nigeria.
Study design
A crowdsourcing approach as described by the TDR (The Special Programme for Research and Training in Tropical Diseases) ‘Crowdsourcing in Health and Health Research Practical Guide’ was used.11 The six-stage process of the challenge contest included:
Selection of challenge focus.
Organising community steering group.
Engaging the community to contribute.
Receiving and evaluating contributions.
Recognising finalists.
Sharing solutions.
The crowdsourcing challenge was hosted by SIHI Nigeria, based at Nnamdi Azikiwe University, Awka, Nigeria.
Challenge focus
An advocacy visit to the Anambra SMOH was carried out to decide on the challenge focus for the crowdsourcing challenge. This was accomplished through a formal meeting with the Anambra State Commissioner for Health and Directors of the different departments under the Ministry of Health Anambra State, held on 1 July 2020. In the meeting, SIHI Nigeria was introduced and the team also agreed that the pilot crowdsourcing challenge should focus on solutions that improved:
Access to healthcare.
Quality of healthcare.
Diagnosis, treatment or prevention of infectious diseases.
Community steering group
Given that this crowdsourcing challenge was principally for the staff and students of Nnamdi Azikiwe University and the surrounding community, a seven-member university committee comprising multidisciplinary faculty members (who hold academic and administrative roles within the university community) was set up as advisers to oversee the running of the SIHI Nigeria hub project. These individuals were invited to serve as members of the expert panel.
Patient and pubic involvement
Due to the competitive design of the crowdsourcing challenge and its focus on identifying healthcare interventions, no patients were involved.
Crowdsourcing of innovation
Participant recruitment was achieved using materials designed to crowdsource for innovations. A nomination platform was designed to receive innovations (https://socialinnovationshare.org/login/index.php), while emails were sent to different organisations through mailchimp requesting support for the call dissemination, nomination flyer explaining the call, challenge focus, timelines, eligibility criteria, benefits of participation and social media advertisement of the innovation call. The innovation call ran for 6 weeks.
Receiving and evaluating contributions
All the innovations received after the close of crowdsourcing challenge call were reviewed by the primary implementation team (SIHI Nigeria). The team shortlisted those who were eligible based on the following exclusion criteria:
The application was incomplete (has insufficient information for a fair review).
The solution was a medical, scientific or advanced device innovation.
The solution has been operating for at least 1 year.
The solution was not implemented in Nigeria.
The shortlisted innovations were sent to the 10-member panel of experts who reviewed and scored them according to the selection criteria in table 1. Members of the expert panel were selected because of their deep awareness of the local context with expertise in infectious disease, innovation and public health. Also, two staff members of the SMOH were appointed as members of the expert selection panel in addition to eight other professionals selected. The scores (for each criterion) from the 10-member panel of experts were averaged, converted to a 5-point scale and subsequently used to rank the innovations (table 2).
Selection criteria used by the panel of experts
Average score of innovation
The operation offices of the top innovations were visited by the SIHI Nigeria team for case study research. The case study research used a descriptive and explorative design to understand the value, examine how the innovation operates and learn transferable lessons from the innovations.12 In the case study, the context, the inventing actor, the solution and the implementing organisation were examined. Methods used for data collection included document reviews, participant observations and semistructured interviews. All data collected were de-identified, while recorded interviews were transcribed.
Finally, averaged and ranked scores from expert panel members as well as updated information from case studies were collated and presented in a physical meeting to the 10-member panel of experts, SIHI Nigeria team and the Anambra State Commissioner of Health with other staff members of SMOH. At the meeting, the top three innovations were selected.
Recognising finalists and sharing solutions
The top three innovations were unveiled on 25 March 2021, at a ceremony held at Nnamdi Azikiwe University, Nigeria. The Anambra State Commissioner for Health, directors of different departments in the Ministry of Health, the Management of Nnamdi Azikiwe University, Nigeria, and a host of other philanthropists and important stakeholders in health were invited to the ceremony. The case reports of the top three innovations were also shared via the SIHI website, TDR-WHO newsletter and social media. The innovations were also promoted via case brochures and peer-reviewed articles.
Results
Seventeen innovations were received during the crowdsourcing challenge. Five of the innovations were eligible and were sent to the panel of experts for review. Figure 1 shows the pictorial decision grid used during our crowdsourcing process and the average scores of the innovations are shown in table 2. Following the review of the average score and report of the case study research, the panel of experts and our stakeholder (SMOH) selected the top three innovations. These included a digital health solution, a mobile clinic and a community-based health insurance programme. The top three innovations are summarised in table 3.

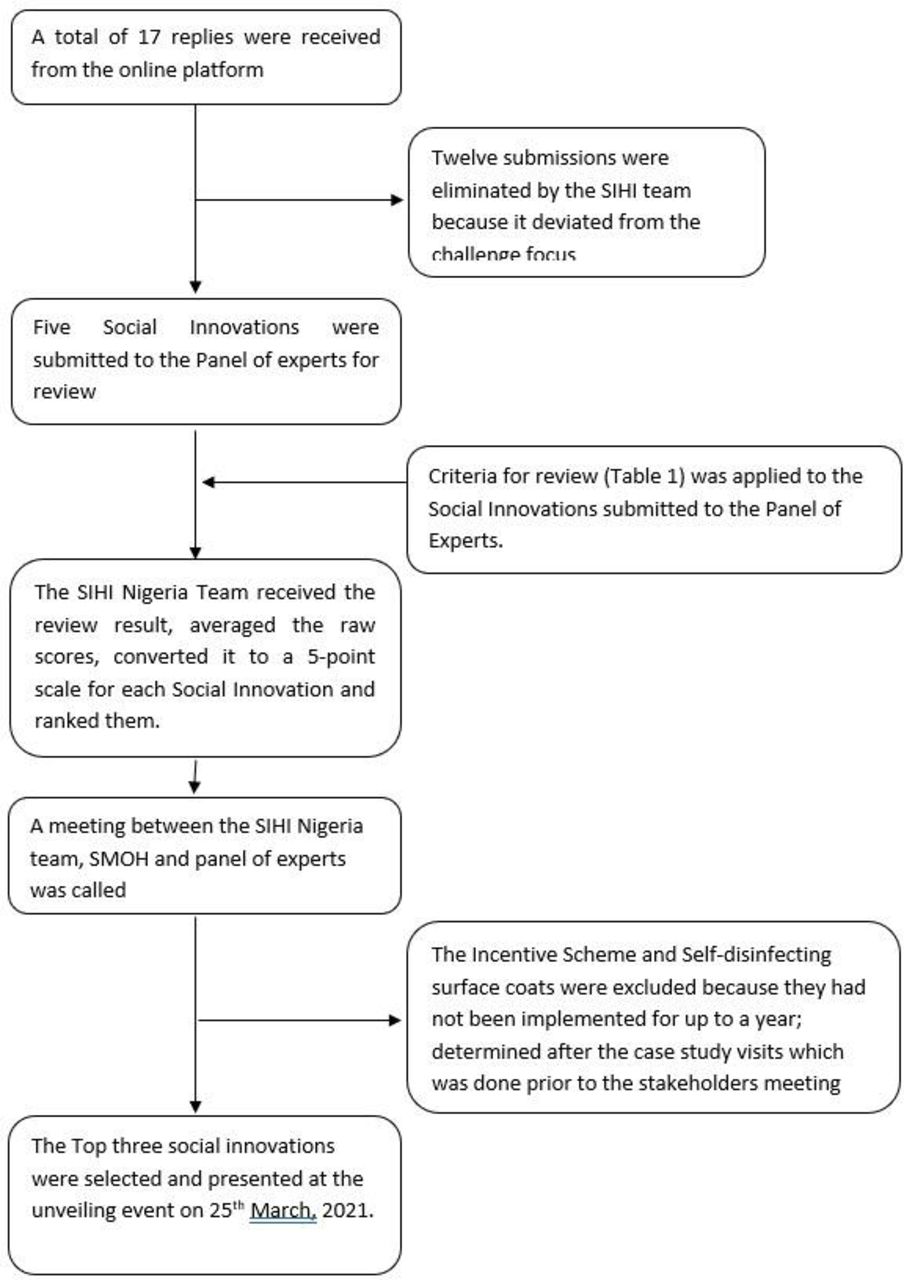{kind=link}
Pictorial decision grid for the crowdsourcing process. SIHI, Social Innovation in Health Initiative; SMOH, State Ministry of Health.
Summary of the top three social innovations identified through the crowdsourcing challenge
One of the social innovations identified is Drugmedics.com. It is a digital solution that was founded in October 2018 by a young pharmacist after having worked in primary healthcare centres and tertiary healthcare hospitals in Nigeria and realising a huge gap in access to quality healthcare and supply of medicines in Nigeria. The solution provides access to health information and offers access to healthcare and supplies medicines to Nigerians. Clients could request to chat with a medical professional or request for a drug particularly those uncommonly found in the drug shops and pharmacies. The clients are then connected to suitable medical personnel depending on the type of request. For drug requests, the requested drug is sourced and delivered at the client’s doorstep.
The second top innovation identified is Parker’s Mobile Clinic. The solution was founded in 2019 by a young medical doctor. The solution aims to bring affordable healthcare to people’s doorsteps. The founder believed that this would help in eliminating the challenge of inaccessibility of healthcare among the target beneficiaries, which include the elderly, handicapped, incarcerated, chronically sick and rural dwellers. This was based on the observation that the healthcare needs of this group of individuals are often neglected resulting in high rate of morbidity and mortality among them. Through social media platforms, a variety of healthcare services including family planning, treatment for malaria, pneumonia, hypertension and other common ailments as well as first aid for medical and surgical emergencies could be booked. Services are provided by the doctor and or nurses. The project has a network of nurses who reside in different parts of the states including rural communities, which are used for administering healthcare to clients in their vicinity.
Ukana West II Community-Based Health Insurance (CBHI) is the third top innovation that was borne out of concern for the increasingly poor and inequitable access to quality and affordable healthcare. In August 2014, Ukana West II CBHI, a non-profit community-based organisation, was established to address the issue of ailing health facilities, poor service delivery and uptake, and inequitable access to quality healthcare services. The CBHI aims to ensure that health service is affordable and accessible for all, and also eliminate the out-of-pocket payment at the point of healthcare need through resource pooling. In the CBHI scheme, there is full participation of the community in healthcare service delivery and health financing for the sustainability of the programme. Currently, the Ukana West II CBHI operates as a model where people pay a premium of ₦10 000 ($26.25) per head per year to benefit from the health insurance programme. Some of the most indigent persons from the catchment area are paid for through resource mobilisation from philanthropists.
Discussion
This crowdsourcing challenge aimed to identify social innovations that have been operational in Nigeria for more than 1 year and have improved access to healthcare, quality of healthcare, and diagnosis, treatment or prevention of infectious diseases. Three innovations were identified as the best out of the 17 submissions received. This was lower than the number of responses identified from other studies due to the focus of our crowdsourcing challenge.13 14 While our challenge focused on identifying existing social innovations that had been implemented, the other studies identified ideas that could be used to inform existing programmes. Additionally, our challenge falls under the Tournament Crowdsourcing principle typically directed towards a more focused crowd or individuals with relevant knowledge or in our social innovations that fall within our scope from the healthcare perspective.15
The top three social innovations have the potential to improve access and affordable healthcare service to community members. Our challenge favours the bottom-up approach to ensure that social innovation programmes potentially scaled up already have a track record of positive impact and address the needs of the population while facilitating community engagement and prudent use of existing healthcare infrastructure within the country.16 This is particularly important in policy developments especially on programmes targeting hard-to-reach populations. For example, the CBHI and Parker’s Mobile Healthcare work with primary healthcare and the National Health Insurance Scheme; but while the former is focused on healthcare financing for healthcare delivery, the latter is primarily focused on healthcare delivery on patient request. All three social innovations were characterised by their potential for healthcare delivery to underserved populations. Similar social innovations such as the Pele smart boxes and the Safe Water and Aids Project in South Africa and Kenya, respectively, have been shown to improve healthcare delivery among underserved populations.17 18
However, the effectiveness of the innovations has not been assessed scientifically. Also, two of the innovations, that is, Drugmedics.com and Parker’s Mobile Clinic have barely started with several teething problems. It is therefore important to measure their success and understand the challenges they face in attracting more investments. This is important in convincing the government, development partners and philanthropists that it could be worthwhile to inject additional funds into these innovations for possible scale-up. Therefore, SIHI Nigeria, as part of her next steps, will identify postgraduate students whose role will be to research the following aspects of the innovations:
Clinical effectiveness–this will measure the effectiveness of the innovation on patients’ health (morbidity and health-related quality of life).
Patient perspectives–this will measure issues related to the perception of the patients/clients on the innovation.
Economic aspects–from a societal perspective, an economic evaluation comparing the innovation with the normal practice in terms of costs and consequences (quality-adjusted life years) will be conducted.
Implementation challenges–using qualitative studies, teething problems facing the innovations will be identified and ways to mitigate and upscale the innovations will be established.
Our crowdsourcing challenge process was significantly limited by the COVID-19 pandemic and the accompanying national lockdown in the country. This was largely due to the fact that SIHI Nigeria was still in the process of designing and adapting the crowdsourcing process, as well as identifying and contacting relevant stakeholders. As a result, there were delays and deviations from the initial work plan and all meetings, correspondence and expert panel result reviews were done virtually. Another limitation was the fact that only five (29.4%) of all submissions were within the preset scope. This may imply that the reach for participant recruitment process using the emails, flyers and social media engagement was suboptimal or reflects a poor understanding of the meaning of social innovation within the Nigerian context.
Conclusion
Using the crowdsourcing challenge process, top three social innovations were identified. These innovations could be refined and scaled up to increase universal health coverage in Nigeria by subjecting them to further research.
Data availability statement
Data are available upon reasonable request. The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and the Nnamdi Azikiwe University Teaching Hospital Ethics Clearance Committee provided ethics approval for the study (approval number: NAUTH/CS/66/VOL.13/024/202/024). Participants gave informed consent to participate in the study before taking part.
Acknowledgments
We would like to thank all the key informants who participated in the case studies. We would also like to thank Dr Phyllis Awor from SIHI Uganda at Makerere University, Uganda for her guide during the crowdsourcing challenge. We are also grateful to SIHI Ghana for sharing with us their experiences in conducting a crowdsourcing challenge. Finally, we wish to acknowledge the expert panellists who reviewed the innovations and Anambra State Ministry of Health for facilitating some of our activities during the crowdsourcing challenge.
Footnotes
Twitter @obinofanta
Contributors ON and OIE designed the study. All the authors participated in organising the crowdsourcing challenge. All the authors participated in the case studies. OIE, OBA and KCA wrote the case studies. OIE wrote the first draft of the manuscript. All the authors contributed to and critically revised the manuscript. All the authors read and approved the final manuscript. ON served as the guarantor for this research.
Funding The crowdsourcing challenge was funded by the WHO (approval number: 2020/1013604-0).
Disclaimer The study funder had no role in study design, data collection, data analysis, data interpretation or writing of the report. The authors alone are responsible for the views expressed in this article, and they do not necessarily represent the decisions or policies of PAHO or TDR. In any reproduction of this article there should not be any suggestion that PAHO or TDR endorse any specific organisation services or products.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.