Article Text

Abstract
Medical education reforms are a crucial component to ensuring healthcare systems can meet current and future population needs. In 2010, a Lancet commission called for ‘a new century of transformative health professional education’, with a particular focus on the needs of low-income and-middle-income countries (LMICs), such as Vietnam. This requires policymakers and educational leaders to find and apply novel and innovative approaches to the design and delivery of medical education. This review describes the current state of physician training in Vietnam and how innovations in medical education curriculum, pedagogy and technology are helping to transform medical education at the undergraduate and graduate levels. It also examines enabling factors, including novel partnerships and new education policies which catalysed and sustained these innovations. Our review focused on the experience of five public universities of medicine and pharmacy currently undergoing medical education reform, along with a newly established private university. Research in the area of medical education innovation is needed. Future work should look at the outcomes of these innovations on medical education and the quality of medical graduates. Nonetheless, this review aims to inspire future innovations in medical education in Vietnam and in other LMICs.
- policy
- global health
- health
Data availability statement
No data are available.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Summary box
What is already known?
Medical curricula and pedagogy in many countries, particularly in low-income and middle-income countries (LMICs), are based on traditional approaches to teaching and learning.
Innovations in medical education are needed to ensure that healthcare services can meet current and future population health needs.
What are the new findings?
Innovations in medical education are possible in LMICs such as Vietnam.
Innovations are introduced and enabled through novel partnerships and government and institutional policies.
Innovations require local experts and stakeholders to lead the work of adapting, planning and implementing, ensuring that innovations are contextually and culturally appropriate.
Introduction
Current evidence suggests that, in low-income and middle-income countries (LMICs), healthcare system improvements are necessary to ensure healthcare services can meet current and future population needs, including evolving epidemiological disease patterns, shifting demographics, new infectious disease health threats and the health impacts of climate change.1 Medical education reform is an integral component of any such effort, and is an area of significant concern for LMICs, which struggle with recruiting, training, retaining and distributing a high-quality physician workforce.2 3 In 2010, a Lancet commission called for ‘a new century of transformative health professional education’, with a particular focus on the needs of LMICs.4 The Lancet report is a call to action to transform healthcare education worldwide by providing a framework and recommendations to reform healthcare education, including much needed political, financial and leadership commitments.4 Achieving this ambitious goal requires policymakers and educational leaders to find and apply novel and innovative approaches to the design and delivery of medical education.5 6
Medical education in Vietnam
Vietnam, an LMIC in Southeast Asia, has a medical education system (figure 1) which, until recently, had changed little despite substantial advancement in most other parts of society and in the health needs of patients.7 Previous medical education reform efforts have been sporadic and limited to single medical universities in specific departments, and not comprehensive or widespread.8 Starting in 1999, medical educators across Vietnam collaborated to promote a community orientation to undergraduate medical education (UME), and identified learning objectives and outcomes in the form of the knowledge, attitude and skills expected of a medical school graduate.9 10 This was the groundwork for the Ministry of Health (MOH) to issue the first set of standard competencies for general doctors in 2015. However, their implementation has been limited.8

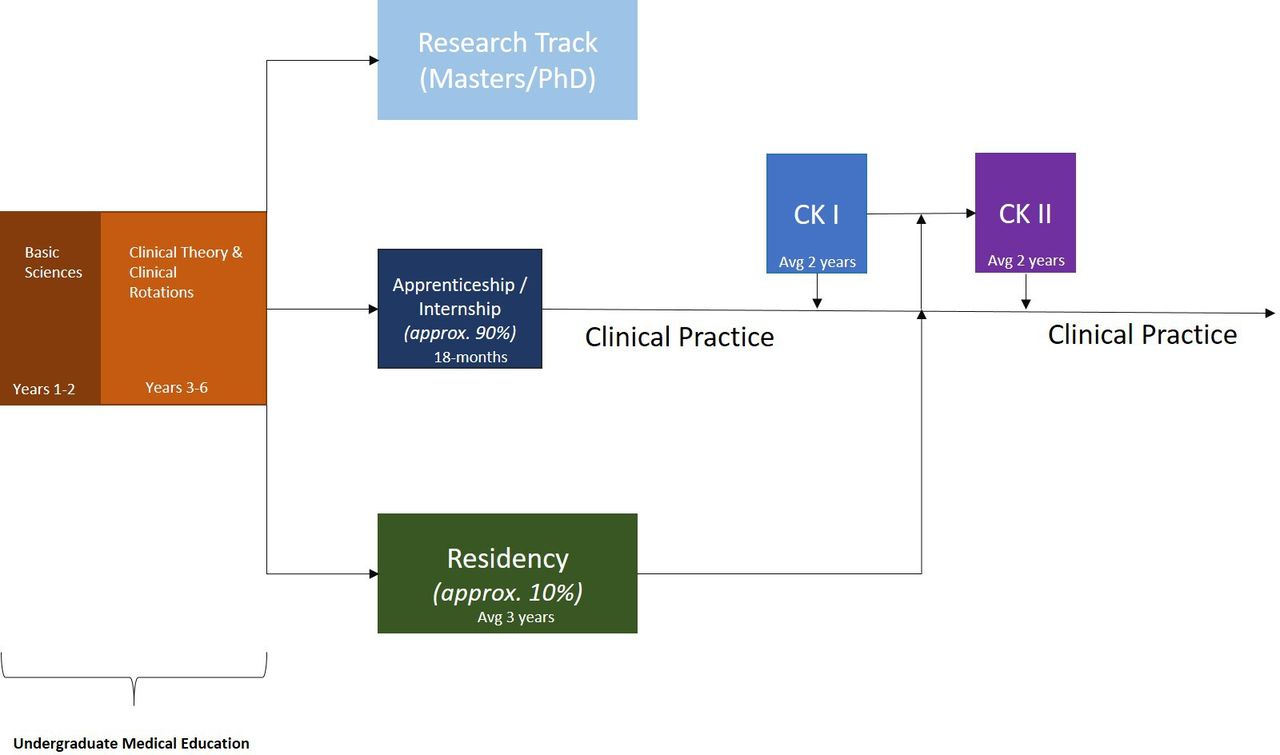
Summary of medical education system in Vietnam.
Currently, there are 29 medical universities in Vietnam, with an average of 400–600 medical students matriculating per year at each school.11 UME is a programme of 4–6 years following the completion of secondary education.7 Most programmes are 6 years in duration and are organised in a traditional format of 2 years of basic science with minimal early clinical exposure, followed by clinical theory and hospital rotations through national and provincial hospitals in the remaining 4 years.7 On completion of UME, there are two major pathways for graduates. The first is the residency track, modelled after the French competitive interne des hôpitaux system.12 These take place at major academic medical centres and include both specialty and subspecialty programmes. Currently, approximately 10% of graduates enter the residency track in Vietnam. The remaining graduates find their own placement at various hospitals and enter apprenticeship-style internships for 18 months, after which they are eligible to register for a medical licence from a provincial department of health. After completing internship and attaining a medical license, physicians can practice in the area of their training or immediately pursue further specialist-level ('chuyên khoa' (CK)) training (specialist level 1 or CK I) and then further subspecialist training (specialist level 2 or CK II). Both CK I and CK II take an average of 2 years to complete. Physicians completing residency are able to either practice after obtaining a medical licence or enter CK II training directly. Currently, there is no national examination prior to licensing, although a plan has been set for its establishment in the near future.7
There is currently wide consensus among policymakers in Vietnam on the need to reform and modernise the country’s educational system due to increasing incidence of non-communicable disease, emergent infectious diseases, health challenges arising from the global climate crisis and widening inequalities.10 13 14 In particular, curricular reform in medical education, both undergraduate and graduate, has been prioritised.7 9 15 The MOH has catalysed reform efforts through investments and policy changes with a vision towards integration with the international medical community.8 Such national-level commitment has created an enabling environment for educators to develop and share innovations. UME curriculum reform is currently under way at five public medical universities, including the University of Medicine and Pharmacy (UMP) at Ho Chi Minh City (HCMC), Hue UMP, Thai Binh UMP, Hai Phong UMP and Thai Nguyen UMP. Graduate medical education (GME) reform is currently under way in HCMC. Additionally, a new private not-for-profit health sciences college at VinUniversity (VinUni), has recently launched in efforts to increase the quality of healthcare professionals in Vietnam.
In this article, we describe two areas of innovation in medical training in Vietnam (curriculum and technology) and we review how these innovations were enabled through partnerships and policy changes. These innovations are de novo (arising within Vietnam) or they are Vietnamese adaptations of practices from other countries but are considered new for the Vietnamese context. They address challenges experienced by medical universities in Vietnam. Our review is based on the published and grey literature, as well as the collective experience and knowledge of the authors on this manuscript.
Curricular innovations
Like many institutions around the world, those in Vietnam are embarking on curricular reforms aiming to train physicians better prepared to meet population health needs. Five public UMPs are transforming their UME programmes to a competency-based curriculum. Competency-based medical education (CBME) focuses on outcomes, emphasises application of knowledge and practice, and promotes greater learner-centredness.16–18 In 2015, the Vietnam MOH created standard UME competencies based on the population health needs of Vietnam.19 To develop the new curriculum based on these competencies, UMP faculty used the principles of backward course design, defining subcomponents for each competency, creating milestones, selecting appropriate assessment tools and strategies, and finally designing educational activities and teaching methods.20 The application of milestones in the UME curriculum is a novel approach. Developmental milestones have been applied in various GME programmes; however, its implementation in the UME context is relatively new and varies globally.21 22 Milestones increase transparency for both the learner and faculty as they define the minimum standard that learners need to accomplish at a point of time along their pathway towards competency.23
The reformed curriculum is characterised by interactive teaching and learning activities constructively aligned to the achievement of the expected learning outcomes. In delivering the curriculum, reform efforts have focused on implementing active pedagogical approaches, reducing time spent in passive lectures. Passive learning approaches have been shown to negatively affect student understanding and discourage problem-solving, self-directed learning and other critical skills needed for healthcare professionals.24–26 This is a particular challenge in the Vietnam context due to large class sizes (400–600 medical students per year per UMP) and low faculty-to-student ratios. To overcome these challenges, faculty reviewed pedagogical approaches used in other settings and iterated and adapted them to fit the needs of Vietnamese classrooms. While small group learning is desired, the large class size necessitates strategies for bringing active learning to a large group setting. One such strategy is the use of an audience response system (ARS) with think–pair–share approach to generate discussion and peer learning.27 28 However, in lieu of expensive technology-based ARSs, faculty developed a colour-coded paper-based system which could be quickly scaled up and implemented. A second strategy is the use of team-based learning (TBL). TBL increases learner-centredness, promotes active learning with peers and, unlike more traditional problem-based learning approaches, can be implemented in settings with low faculty-to-student ratios.29 In the Vietnamese adaptation of this approach, approximately 40 students are provided a faculty facilitator who engages with teams of five to eight students. Student teams work together and are held accountable to one another in the three distinct phases of TBL: (1) a preparation assignment prior to the in-person session, (2) individual and group readiness assurance tests consisting of multiple choice questions focused on the preparation assignment, and (3) a group application activity that requires students to apply the material from the preparation assignment to a ‘real-world’ scenario.29 The approach has been successful in Vietnam because it allows for a problem-based approach to learning, enables peer-to-peer learning and accountability, promotes teamwork and can be implemented with fewer faculty resources than other small group learning methods.
UME competencies in Vietnam include teamwork and interprofessional collaboration. Although interprofessional collaboration is a core competency in many countries’ medical education frameworks, including those from the Accreditation Council for Graduate Medical Education and the Royal College of Physicians and Surgeons of Canada,30 models for authentic interprofessional education are still limited, even in high-resourced settings.31 32 Prior to CBME reforms, medical students in Vietnam learnt nursing skills through both simulation and practice on the wards. Students are taught by nursing faculty, observe nurses on the wards and participate in patient care under the supervision of nurses, prior to entering clerkship rotations. This novel interprofessional education model was maintained in the new curriculum. To further promote interprofessional education, UMP at HCMC introduced a new course in September 2019 for medicine, pharmacy, nursing and rehabilitation students. Faculty members from the different disciplines cooperated to design a course which promotes student collaboration and foster skills related to interprofessional practice including: (1) understanding the value of interprofessional care, (2) effective communication, (3) professionalism, and (4) team leadership skills. This is the first course in Vietnam taught to an interprofessional group of students by an interprofessional faculty.
Technological innovation
Integration of technology into medical curricula can catalyse the application of adult learning theory in medical education and help to transform the learning environment from solely a distributor of content and knowledge into a space which facilitates the learning process and the assessment of the learner.33 In doing so, learning environments can be expanded beyond the traditional domains of classrooms, lecture halls and libraries into virtual spaces. A key pillar of the reform at medical universities in Vietnam has been to adapt new learning technologies and invest in network infrastructure to enable their application.
Medical education programmes in Vietnam have expanded their virtual footprint through the use and customisation of free, open-source learning management systems (LMS) such as Moodle for public universities, and subscription-service LMS such as Canvas and One45 for private universities such as VinUni. While some institutions have used the LMS solely as a platform to upload and download class materials, others have customised the LMS to allow for more advanced features, such as collecting feedback from students and faculty, creating message boards and discussion forums, administering assessments, developing online resource centres or libraries and implementing online learning courses. For example, in collaboration with the Surgical Council on Resident Education (SCORE), a US consortium that created a standardised competency-based online curriculum for US surgical graduate programmes, the SCORE Portal was introduced and tailored for use in the general surgery residency programme at UMP at HCMC; VinUni also uses the SCORE framework as part of their GME programme. While still in a pilot phase, the application of competency-based on-line training materials ensures that all general surgery residents can receive a common curriculum and develop a common knowledge base. This is a novel approach for GME in Vietnam, helping to reorient the curriculum away from the more typical teacher-centred approach to a learner-centred approach in which learners can access online modules on their own time and proceed at their own pace.
Investments and innovations in technology, such as the implementation of LMS described previously, enabled universities in Vietnam to rapidly transition to online learning when the COVID-19 pandemic began in February 2020. Faculty and students were already familiar with LMS and online learning platforms, such as Zoom, Microsoft Teams and Google Hangout. As a result, disruption to the programme was minimised when social distancing measures were enforced. In addition, having capacity for online teaching and learning was beneficial for disseminating knowledge about the novel SARS-CoV-2 virus. The UMPs used their existing infrastructure to quickly roll out a virtual COVID-19 training programme for senior medical students. Students were trained, using a blended approach, on the epidemiology and prevention of SARS-CoV-2, including contact tracing, triage and testing. To date, over 720 medical students have been deployed in Vietnam’s COVID-19 response.34 35 As faculty and students become more familiar with virtual teaching and learning, some institutions have planned for 20% of the curriculum to be delivered virtually beyond the COVID-19 pandemic.
Enabling partnerships
A number of novel partnerships have helped to enable and catalyse innovations in medical education in Vietnam. Partnerships between industry and international institutions create an enabling ecosystem for innovation to thrive.36–38 In particular, international academic partnerships can provide a source of innovation. For example, Harvard Medical School (HMS) has partnered with the Vietnam MOH’s Health Professionals Education and Training for Health System Reforms Project and medical universities in Vietnam as part of the Improving Access, Curriculum and Teaching in Medical Education and Emerging Diseases (IMPACT MED) Alliance.39 With funding from the United States Agency for International Development, the IMPACT MED Alliance supports UME curricular reform at five medical universities through provision of technical assistance and knowledge transfer on curriculum design, development and implementation. Similarly, VinUni has a strategic alliance agreement with the University of Pennsylvania with a goal of innovating health professional education through technical support on curriculum development and implementation, and by improving service delivery and patient care.40 Both of these academic partnerships also involve student and faculty exchanges, and promote research collaborations. As novel concepts and approaches are introduced through these partnerships, local experts and stakeholders lead the work of adapting, planning and implementing, ensuring that innovations are contextually and culturally appropriate.
A second example is a public–private partnership between Microsoft and public UMPs, facilitated by the IMPACT MED Alliance, which initially provided free online access to the Microsoft Office 365 Suite for all university students, faculty and staff at the participating UMPs. With technical assistance from Microsoft, the full functionality of the Microsoft Office 365 Suite was introduced and incorporated into university operations, leading to transition to a discounted, full-access subscription. Using the Microsoft Office 365 Suite has helped to streamline the institutions’ communication and administrative functions. University administrators and leadership can easily communicate with all members of the university community; students have a single point of entry for virtual coursework and LMS access; and university administrative functions such as human resources management have been integrated into a common system. Prior to this, paper-based systems were employed; faculty communicated with students through various social media platforms; and communication was paper-based or via personal email addresses and mobile phones. This example demonstrates the importance of public–private partnerships with technology and technical skills transfer combined with appropriate financing mechanisms for introducing and sustaining technological solutions.
Another example of a private sector partnership which resulted in technology and technical skills transfer is between Samsung and the UMPs. Samsung invested in two demonstration ‘smart classrooms’ at two UMPs. The smart- classrooms were designed to promote group learning and are technology-enabled to facilitate access and sharing across the internet. Aligning classroom infrastructure and technology with the curriculum design and pedagogical method is vital to the success and sustainability of the new curriculum. Following a trial of the demonstration classrooms, students, faculty and leadership all recognised the value of this alignment, leading to university investment in classroom redesigns at all five UMPs.
Enabling policies
Policy changes are often necessary to drive and sustain reform, as they can enable medical education institutions to adapt, implement and continue innovations. The Vietnamese government created an enabling environment for innovation in education through the implementation of national policies related to university autonomy in 2014.41–44 These policies promote public universities to become financially independent and encourage them to manage their own operations, human resources and strategies for growth. The new framework enables public institutions to seek partnerships with the private sector and international academic institutions, helping to prioritise investments in technology and to promote new curricula, pedagogy and educational approaches. In addition, institutions are empowered to redesign their management and administration structures. Such restructuring was important to the development of a more integrated CBME curriculum at the UMPs.45 In the traditional model, department chairs held decision-making authority over the teaching content, resulting in a curriculum organised around specific disciplines. To develop a more integrated curriculum, it was necessary to break down this governance structure and to provide authority to curriculum committees consisting of multidisciplinary teaching faculty (figure 2). Committee leaders decide what is included in each module, which faculty should teach and what adjustments should be made as part of the curriculum quality improvement programme.

{kind=link}
{kind=link}
Curriculum governance organisational chart.
Another policy enabler at the university level has been the development of a system for continuous quality improvement (CQI) of the curriculum and its implementation. Newly formed units within the university lead the CQI process by creating mechanisms for routine collection and use of student feedback and faculty and student evaluation data with a goal of continually improving the curriculum and teaching to match student needs. Data are shared to curriculum committees and university leadership and are used to make decisions regarding future adjustments to the programme. This system also provides data to faculty and administrators on the adoption of novel approaches and innovations, allowing them to continually iterate, improve and tailor for specific contexts. These units also generate supporting data for future accreditation processes.
Limitations
This review highlights several recent innovations in medical education in Vietnam. It is not intended to be a comprehensive review of the health professional education system or the curriculum reforms currently under way. Our review is shaped primarily by the coauthors’ knowledge and experience and to what is published in the English language literature. While the innovations described here may apply to other settings within and outside Vietnam, we recognise that barriers may exist to the successful uptake of these approaches. First, institutional reform requires forward-thinking and robust leadership at both the national and institutional levels. A lack of such leadership can limit the ability to enable and adopt innovative approaches. Second, resources (human, financial and infrastructural) can be a significant barrier to change, particularly in the resource-limited setting. For example, technology-enabled reforms require reliable internet connectivity, which may be a significant barrier in many resource-limited settings. This further highlights the importance of strong leadership commitment and novel partnerships to mobilise necessary resources. Third, the culture of an institution is a crucial factor in the creation and adaptation of innovations. Without a willingness to embrace new ideas and to take risks and fail, innovation would not be possible. Lastly, not all change leads to improvement. We have described innovations that proved successful, but others may have been less so. While there is still much to learn from less successful reforms, that was not our focus in this review.
Conclusion
It has been more than 100 years since the Flexner report inspired a transformation of medical education.46 Today, in the face of significant global health workforce challenges, there is again a need to rethink our approach to professional health education.4 Innovation and reform in medical education are needed, particularly in LMICs. In this review, we have shared examples of innovations developed as part of Vietnam’s current medical education reform, including those in the areas of curriculum design, pedagogy and application of technology. We have also described how partnerships and policy changes can enable, encourage and sustain innovation. While every healthcare system has unique challenges, we hope these examples from Vietnam can inspire future innovations in medical education.
Data availability statement
No data are available.
Ethics statements
Acknowledgments
The authors would like to express their gratitude to the Vietnamese Ministry of Health for their strong leadership in medical education reform. Additionally, we thank leadership at the five universities of medicine and pharmacy and VinUniversity, along with medical education collaborators at Harvard Medical School and University of Pennsylvania for their contributions to this project, and also Mr Mark Hickey from Surgical Council on Resident Education for his collaboration.
References
Footnotes
Twitter @DrDavidDuong, @NisaePakistan, @toddmpollack
Contributors The original conception of the idea was by TPo and DBD. The literature search was done by DBD and TPh. The manuscript was written by DBD with contributions from all coauthors. The guarantor of this manuscript is TPo.
Funding The IMPACT MED Alliance is supported through the generous donation of the American people through the United States Agency for International Development Cooperative Agreement No. AID-440-A-16–00002.
Disclaimer The views and opinions expressed in this paper are those of the authors and do not necessarily reflect the views and opinions of the United States Agency for International Development.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, conduct, reporting or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.