Article Text

Abstract
Objective Organ transportation requires innovation. We recently showed that unmanned aircraft systems (UAS) could transport human organs. There are no data addressing UAS acceptance among healthcare providers. Conceptually, UAS implementation may improve delivery of care through improved efficiency. We sought to learn surgical perspectives on current and innovated organ transport systems.
Methods An Institutional Review Board exempt, pretested, 5-point Likert scale web-based survey was undertaken. Transplant surgeons taking kidney transplant offers in the USA (n=174) were sampled.
Results Of 174 surveys, 122 were delivered successfully, and 55 responses collected. Mean age was 48.1 (range 34–64), and 80% were male. Forty-two (76.4%) surgeons felt cold ischaemia time reduction to 8 hours would increase organ acceptance rates. More than 23% of respondents were fearful and 34.5% nervous regarding drones. Nearly all (92.7%) respondents believed drones could help people; 90.9% felt the mode of transportation was irrelevant to their decision to accept an organ but that speed and quality were most important. Only 16.4% of surgeons believed the current system is adequate for our transportation needs.
Conclusions Surgeons feel the present system of organ transportation needs reform, and an innovated system using UAS might improve care. An innovated organ transportation system involving UAS may lead to fear and anxiety among transplant surgeons, suggesting that research and education are required ahead of adoption.
- clinical decision-making
- delivery of health care
- ethics
- health care facilities, manpower and services
- health care quality, access and evaluation
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- clinical decision-making
- delivery of health care
- ethics
- health care facilities, manpower and services
- health care quality, access and evaluation
Introduction
There is a critical shortage of donor organs in the USA, and this shortage leads to deaths on the transplant waiting list.1 2 Even so, many high-quality organs with low kidney donor profile index (KDPI), a marker of organ quality based on 10 donor factors, are declined for transplantation due to the challenges and logistics of organ delivery.1 3 4 A recent study observed that as many as 3500 organs yearly are discarded that could be transplanted within the current donor pool.3 5 This is because the current system of organ shipment employs a complicated, inefficient network of non-specialised commercial couriers, without any real-time monitoring of organ location. Transportation of a single organ requires significant coordination between transplant coordinators, organ donation organisations, both the recipient and donor hospital surgical teams, and transportation couriers (commercial or private airplanes, car services). Accordingly, when shipment is inefficient or prolonged, organs experience increased cold ischaemia time (CIT), which is associated with increased morbidity and mortality for the patients.6
The current average CIT for kidney transplantation is between 18 and 21 hours. Organ handling and shipment times are the most significant contributors to the CIT.2 7–10 With accepted maximum CIT of approximately 24 hours, even ‘average’ kidneys in the current transportation system experience high CITs, driving up rates of delayed graft function (DGF) and impairing long-term graft survival.11 12 Beyond shipment time, the complexity of the present system increases expenses, particularly in the case of chartered shipment.11 Travel safety for the transplant team recovering organs is also a critical concern in the current organ transport system.13 14 Despite these significant challenges, minimal progress has been made to innovate the current system of organ shipment.
The current organ transportation system involves an organ procurement organisation (OPO) that coordinates matching the organ to a recipient in a computer system based on blood type, wait time, survival benefit and the donor hospital zip code, among other factors. This allocation system uses a computer program that identifies the best match candidates based on the above factors, and the hospital at which these candidates are on the transplant list are contacted. Due to higher than necessary discard rates of kidneys, variability in access for difficult to match candidates and inequities in waiting time, the allocation system has been modified multiple times to address these issues. A consequence of the new allocation system is longer travel times and distances for transplant organs. The accepting transplant surgeon then decides based on the organ information, location and logistics whether they will accept or decline the organ offer. Depending on the distance and resources, organs are either procured by the recipient transplant team who flies to the donor hospital to recover the organ, or the organ is shipped nationally on commercial airplane couriers to the recipient hospital, known as an imported organ.
Recently, technological innovations have paved the way for unmanned aircraft systems (UAS, commonly ‘drone’) to deliver payloads such as defibrillators and medical materials.15–17 Civilian drones have the ability to travel more than 200 mph, carry a load greater than 500 pounds and travel more than 1000 miles.18 Currently, gas-electric hybrid devices are capable of staying airborne for more than 10 days without refuelling. Regulatory action by the Federal Aviation Administration (FAA) around UAS suggests that commercial and medical delivery will be available in the next 2–3 years.19–23 Such technology has the potential to improve the current organ transportation system and decrease CIT by bypassing traditional airport and courier systems and allowing direct travel from the donor to recipient hospitals.24 Our team recently demonstrated that UAS can be used to safely transport a human organ.25 Though unaccompanied by a courier, we showed that the organ’s geolocation and quality could be monitored real time during UAS flight with our innovative technology.25 26 In this way, we recently performed the first ever organ transplant of an organ shipped by UAS, carrying a payload weight of approximately 10 pounds.27 Furthermore, UAS organ transportation would eliminate the flight risk for transplant recovery teams. Conceivably, because UAS could provide for ‘on demand’ transportation, defined as drone flight availability whenever an organ becomes available for transplant, UAS technologies may be able to supplement the current transportation system.
Transplant physicians play a critical role in the logistics of organ shipment. Organ logistics are intertwined in organ acceptance. As such, travel challenges may hamper the ability to accept and transplant an organ, particularly in the case of imported kidneys.2 4 We have hypothesised that transplant surgeons would view on-demand transportation as favourable. Second, we have hypothesised that while surgeons are interested in innovation, the use of a novel UAS transportation network may cause anxiety and scepticism. To this end, we have attempted to learn the surgical viewpoints of both the current and innovated systems of organ shipment involving UAS.
We have conceptualised a novel construct for transplant care delivery involving the use of unmanned aircraft in order to efficiently transport an organ from the donor to recipient hospital. Such an innovation requires significant dialogue among stakeholders in advance of implementation. Prior studies have demonstrated that the public’s perception of drone use is mixed, although use for humanitarian purposes is supported.28–30 We performed a 5-point Likert scale web-based survey emailed to 174 transplant surgeons identified from the American Society of Transplant Surgeons (ASTS) member directory as kidney transplant surgeons practising in the USA.
Taken together, we found that surgeons feel the current system of organ transportation needs innovation. We found that surgeons were unaware of significant advances in drone technologies and that introduction of UAS for the purposes of moving organs will likely cause anxiety among a portion of transplant surgeons. We additionally observed that, irrespective of the innovation (eg, UAS), technologies which improve CIT and organ quality are of great interest to the field. Further research and testing are needed to evaluate the medical, human, technological, logistical and regulatory aspects of drone transportation ahead of implementation.
Methods
Conceptual model of future organ delivery
At present, more than 50 individuals are involved in the complex network required to move a single transplantable human organ from a donor to recipient hospital, leading to excessive time and cost, and reduced organ quality. We have proposed a new innovative construct in which unmanned aircrafts move organs directly from donor hospital to recipient hospital, theoretically reducing cost and shipment time, while improving organ quality (figure 1). This study aims to address the human impact of drone use for organ transportation.
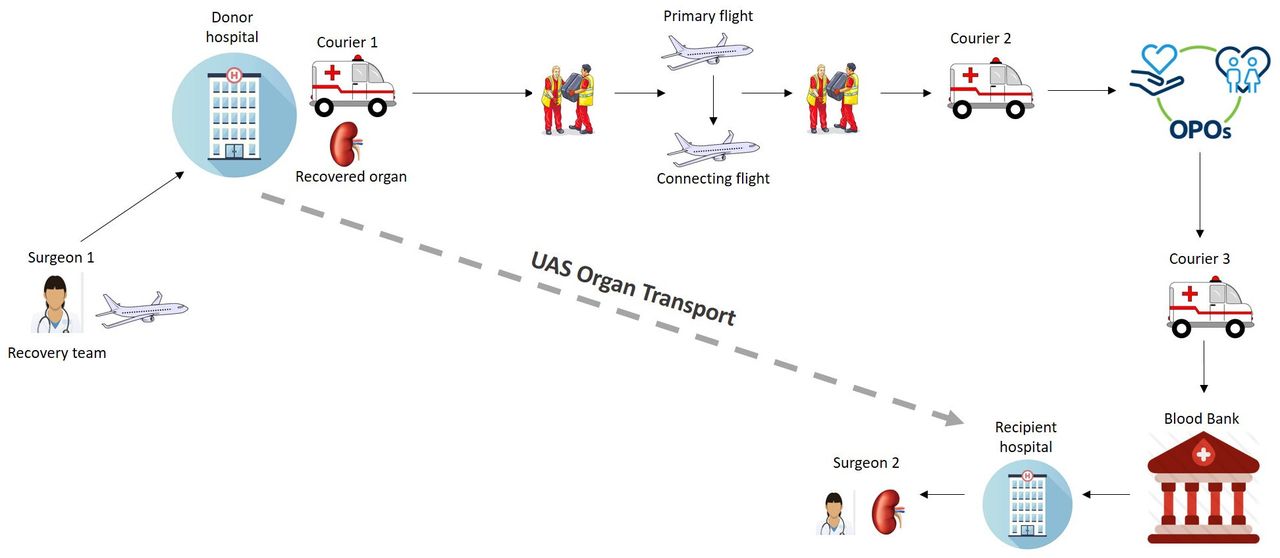
Conceptual model of the current organ transportation system versus the novel UAS transportation (grey dashed line). OPO, organ procurement organisation; UAS, unmanned aircraft system.
Survey and content validation
We conducted an Institutional Review Board exempt survey comprising 40 questions using a web-based survey tool. The survey was designed by the authors in conjunction with the expertise of a social epidemiologist. The survey used novel fixed-choice questions to target specific constructs and response frames using a 5-point Likert scale. The survey questions were broken into six subsections: demographics, knowledge of drones, consideration of CIT and donor parameters in organ selection, surgeon perception of drones, willingness to accept drone-transported organs and need for real-time organ data during transport. The responses were anonymous and survey participants did not receive any compensation. Prior to implementation, the survey was pretested using the content validity technique, with the survey reviewed independently by five experts in the field of transplant surgery.31 In this way, the survey tool was pretested on a sample (n=5) of transplant surgeons.
Sample
The sampling pool for survey participants were surgeons identified through the ASTS directory. As of 2018, there were 1800 ASTS members of which approximately 1000 were physicians in various stages of training and practice, including residents, fellows and attending-level physicians. Of those physicians in the ASTS directory, 174 were identified as meeting our inclusion criteria: attending-level kidney transplant surgeons who accept organ offers for their institution, practised in the USA and had a listed email address. Surgeons must actively take organ offers to ensure familiarity with the project scope. Surgeons were invited to take the survey through a link sent by email. Of the emails sent, 122 were successfully delivered and 62 responses (36%; 62/174) were received. This represented 50.8% (62/122) of successfully delivered surveys.
Statistical analysis
Descriptive analyses and statistical analysis using Fisher’s test were performed to address our research questions. SPSS statistics 15.0 software was used for performing the data analysis. A p value <0.05 was considered to be statistically significant.
Results
Respondents and demographics
Of the 62 survey responses received, 3 (4.8%) survey responses were excluded because of missing data and 4 (6.5%) additional survey participants were excluded from the final data analysis as they did not meet the inclusion criteria of the study (figure 2). Thus, the total number of completed survey responses of transplant surgeons meeting inclusion criteria was 55 (32% response rate). The mean age was 48.1 (SD 8.67, range 34–64) years. Eighty per cent of the sample identified as male. Demographics can be found in table 1. Most survey participants (92.7%) were from academic institutions and the majority (61.8%) performed an average of 10–50 kidney transplants per surgeon per year. The remaining 38.2% perform greater than 50 kidney transplants per surgeon per year.
Characteristics of sample population

Survey sampling.
Current system: consideration of CIT and donor parameters in organ selection
Among respondents, 92.7% felt that the KDPI, CIT and biopsy results were all factors impacting their decision to accept an organ (online supplemental table S1). Most respondents (76.4%) felt a reduction of CIT to less than 8 hours from the current average of 18 hours would allow them to accept and transplant more organs (online supplemental table S1). For high-KDPI organs, again, surgeons felt they were more likely to accept a kidney if CIT was <8 hours (76.4%) compared with 8–24 hours (65.5%) or >24 hours (25.5%) (online supplemental tables S2).
Supplemental material
Background knowledge of tested innovation: knowledge of UAS
We found that 23.6% of surgeons had flown or piloted a UAS. The majority of participants ranked their knowledge of drones as average or below average (90.9%) (online supplemental table S3). Most respondents believed the primary use of drones was for military (63.6%) (online supplemental table S3) purposes, with the correct answer being recreational use. The majority (89.1%) believed it is possible to move an organ over 3 miles. Fewer (47.3%) correctly believed it is possible to move an organ over 250 miles (online supplemental table S3). The majority of respondents correctly believed that drones could fly autonomously (47.3%), while the minority of respondents correctly selected the maximum speed of a civilian drone to be 200 mph (7.3%) (online supplemental table S3).
Surgeon perception of UAS
We observed that 23.6% of respondents believed civilian drones were scary (online supplemental table S4). Further, 34.5% stated that civilian drones made them nervous (online supplemental table S4). Nearly all (92.7%) participants believed drones have the potential to help people and 72.7% believe that there is a role for drones in medicine (online supplemental table S4). There was no significant difference in fearfulness of drones as stratified by age (figure 3) (p=0.4898 and p=0.7600, respectively). Surgeons who had previously flown a drone were not less likely to view drones as scary compared with surgeons who had never flown a drone before (figure 4) (p=0.6893 and p=0.4885, respectively).

The effect of age on surgeon’s perspective of drones. (A) demonstrates the results based on age group for the survey question ‘drones are a scary concept’ and (B) demonstrates the results based on age group for the survey question ‘civilian drones make me nervous’.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
The effect of previously piloting a drone on surgeon’s perspective of drones. (A) demonstrates the results based on prior drone experience for the survey question ‘drones are a scary concept’ and (B) demonstrates the results based on prior drone experience for the survey question ‘civilian drones make me nervous’.
Innovated system: willingness to accept UAS-transported organs
Surgeon’s willingness to accept UAS-delivered organs was assessed. 90.9% of respondents felt the mode of transportation was irrelevant to their decision to accept an organ and that speed and quality of the organ were the primary concern (online supplemental table S5). Furthermore, we observed that only 7.3% of respondents believed drones for organ transportation would change their patient’s decision to accept an organ, while only 12.7% of surgeons believe their patients know how organs are currently transported (online supplemental table S5).
Innovated system: need for real-time monitoring
Of the respondents, 84.4% believed an organ transported by UAS should be monitored real time during transport (online supplemental table S6). A large majority of surgeons (85.5%) felt it would be beneficial to know when an imported organ would arrive, regardless of whether it was shipped by UAS (online supplemental table S6). Only 16.4% of surgeons believe that the current transport communication system is adequate and provides them with sufficient information (online supplemental table S6).
Discussion
Organ transportation is a timely and significant topic in American healthcare. With the ongoing organ shortage and changing allocation practices more organs are travelling further distances, complicating an already challenged system of organ transit.2 9 10 32 Indeed, the supply chain for human organs in the current system involves a complex network of non-specialised commercial couriers which are hurriedly arranged by OPOs. The current system has lagged behind non-transplant technological advancements. To this end, minimal attention or advancement has been applied to the practices of organ shipment over the last 60 years. Here, we continue a dialogue surrounding an innovated construct of transplant care delivery in which unmanned aircrafts are used to move organs from donor to recipient hospital.
In the current system, the timing for organ transplants, particularly imported kidneys, is frequently dependent on ill-timed commercial flights, adding unnecessary CIT that subsequently results in an increased organ failure and often precludes transplantation. This problem was made more complex in the last decade with the consolidation of the commercial airline industry.33 Increased CIT has also resulted from recent redistricting efforts by the kidney allocation system in an effort to improve access to transplantation nationwide.2 9 10 For some organs, the distance has increased by 60% to an average of 706 miles.2 More than 22% of kidneys are now transplanted after 24 hours of CIT which has contributed to the increase in DGF rates from 25% to 31% that subsequently results in increased patient morbidity and excessive financial cost.2 11 34 Beyond timing and price, team safety remains a major concern of transplant professionals. While UAS may not be a panacea for the challenges facing organ shipment, they may be an innovative supplementation to the current system in a way that allows a portion of organs to be moved faster, safer and cheaper. Furthermore, this novel organ transport system would not require changes to the current organ offering computer system used by OPOs. It will likely, however, require a shift in organ shipment infrastructure from commercial airline tracking to real-time drone tracking and monitoring.
Technical, regulatory, human impact and logistical challenges surround the use of UAS for the purposes of organ shipment. Engineers are addressing technical challenges, and the FAA is augmenting the regulatory environment to allow for UAS medical payload delivery.22 23 35 Indeed, the human impact of UAS will affect (1) transplant professionals, (2) transplant candidates, and (3) donor families. As an example, for transplant professionals, if UAS are believed to be unsafe, hasty adoption of UAS for organ shipment may lead to fewer transplanted organs. From the standpoint of a transplant candidate, if UAS are perceived as negative or ‘scary’, this too may lead to disinterest in organ acceptance. Indeed, each of these areas is presently unstudied. Here we have addressed one of the three elements of UAS potential human impact. Furthermore, as a novel form of organ transportation, there will be logistical challenges that arise and will need to be addressed.
Regardless of travel, there is a paucity of data regarding organ offer decision-making. As such, we first addressed surgeons’ viewpoints of the current system. We found that 76.4% of transplant surgeons felt a reduction in CIT would allow them to accept more organs (online supplemental table S1). While it is widely known that CIT affects renal transplant outcomes, this is an important observation. As previously mentioned, a significant number of transplantable organs are discarded due to excessive CIT secondary prolonged transportation times. Further, most surgeons would be willing to accept a higher KDPI if the CIT was reduced. To this end, it is possible that innovations which allow for rapid, local shipment of higher KDPI kidneys may yield greater utilisation.
We performed content validity on our survey study prior to its administration using survey questionnaire feedback from five transplant surgeon experts. We were not surprised that surgeons’ understanding of drone technologies was limited (online supplemental table S3). This was important ahead of learning whether surgeons were also willing to accept organs moved by UAS. Additionally, most surgeons did not view drones as scary, and most believe drones have the potential to help people and can be used in medicine (online supplemental table S4). Further, more than 60% of surgeons thought that the current primary use of drones is for military purposes. This is potentially important, because this may imply a negative connotation among stakeholders. Previous studies on drone perception found that the public tends to favour drone applications for medical applications over military use.30 Education and research surrounding the technological capabilities, safety and feasibly of organ drone shipment will be needed for successful UAS implementation.36
Perhaps important is that the majority of surgeons felt time and quality were the priority. Indeed, the majority of surgeons agreed that the mode of transportation was irrelevant and that speed and quality of the organ were their focus (online supplemental table S5). Additionally, only 7.3% of surgeons believe that the mode of transportation of the organ would affect their patient’s willingness to accept the organ (online supplemental table S5). These results are interesting for two reasons. First, there are no large studies on the effects of current modes of transportation on donor organs. Second, while the transplant candidate is informed about the process of transplantation, surgery, recovery and even the quality of the donor organ, patients likely have little exposure as to the methods by which organs are moved.
As such, very few organs are monitored real time with regard to geolocation or organ status. Indeed, there is ‘radio silence’ from the time the organ is packaged to the time the organ is delivered. While this may be reasonable when organs are shipped by courier, if no human being accompanies the organ (as is the case of UAS), it may be necessary to employ advanced monitoring. While Global Positioning System technologies for organ shipment are in development, and while several centres are attempting implementation, there is no present standard for organ monitoring. To this end, even in the present system, the vast majority of surgeons (87.3%) felt it beneficial to have more data for in-transit organs. In this way, only 16.4% of surgeons believe the current transport system is adequate to meet present needs (online supplemental table S6).
This study has several limitations. These limitations include a small sample size, which could contribute to an underpowered study. Additionally, it is possible that surgeons who were more familiar with UAS technology were more likely to complete the survey, thus contributing to an inherent bias in the survey with results demonstrating a more positive perspective of UAS technology for transplantation than that of the general population of surgeons.
There appears to be support for a theoretical and innovative system of unmanned organ shipment in the USA, but this system would require significant testing, as well as surgeon and likely patient education in advance of implementation. It is possible that novel technologies capable of rapid, point-to-point transport could help reform the current system of organ allocation to improve access to transplantable organs. Furthermore, in the wake of the global pandemic (ie, COVID-19) and a significant reduction in commercial flights, the need for novel technological advancements in organ transportation, such as UAS, is even more apparent. Costs associated with using this novel technology may prove to be a barrier to implementation; additional cost analysis studies are needed to evaluate whether the incremental cost increase is offset by more significant savings from reduced rates of delayed graft function due to better quality organs. Innovated organ shipment using UAS can be reasonably expected to require changes in healthcare policy, organ acceptance practices and medical ahead of wide application.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @TalaieTara
Contributors SN assisted in planning the study. EV assisted in designing the survey and validation of the survey. TT conducted the survey and submitted the study. JS assisted in writing the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests JS has a financial interest in MissionGO, a startp-up company which developed as a result of the technologies referenced in this publication.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplemental information.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.