Article Text

Abstract
Introduction Acquired brain injury (ABI) is a major cause of morbidity and mortality in childhood. Specialist rehabilitation services are often situated far from families and local services may be non-standardised and fragmented. A strategic level of understanding is needed to improve patient care and outcomes. Roadmapping techniques are commonly used in industry settings to discover and present a systematic understanding of structures; however, they are rarely used in the healthcare setting. With continuing pressures on healthcare systems worldwide, they provide an effective method for examining services.
Methods The Institute for Manufacturing (IfM) strategic roadmapping method was used to identify areas of difficulty and opportunities in paediatric neurorehabilitation. Participants included stakeholders from a wide range of professions and sectors who have input with children after ABI.
Results Delegates identified a range of ‘layers’ covering trends, drivers, current experience and unmet needs. From these layers, four priorities were identified and further expanded.These included: ‘access to medical and therapy expertise close(r) to home’, ‘shared understanding across family, school and health’, ‘family and professional awareness of resources and support’ and ‘establishing a centre for rehabilitation technology evaluation, advice and co-ordination of services and research’.
Conclusion The IfM strategic roadmapping method identified and developed key areas for development in the field of paediatric neurological rehabilitation. Healthcare professionals looking at strategic level difficulties should strongly consider the use of such systematic tools when evaluating areas of practice.
- delivery
- neurology
- economics
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction and background
Acquired brain injury (ABI) is a major cause of death and disability in the UK and worldwide with approximately 35 000 children admitted following an ABI annually in the UK from traumatic causes alone.1 Non-traumatic brain injuries are less consistently defined but estimated to effect 82.3 children per 100 000 each year.2 The acute management of these children has improved significantly in recent years.3 However, while there is agreement that rehabilitation is required after such an injury, services remain variable and the exact components of optimal clinical management are not well understood.4
Due to the complexity of the developing childhood brain, the full extent of the functional impacts of the injury may not be evident until decades after initial insult.5 While historically patients who appeared on the surface unimpaired after an ABI would have been discharged rapidly from services and left with a possible lifetime of neurocognitive difficulties from what appeared to be a ‘mild’ brain injury,6 there is now a greater understanding about the importance of long-term follow-up and specialist input as people who suffer a brain injury in childhood are at increased risk of offending behaviours7 and mental illness.8
This complexity has led to a lack of standardisation of care. Considerable waiting lists for specialist services which are often a long distance from patients’ homes9 mean that a significant proportion of a child’s rehabilitation journey occurs in their locale. The quality and quantity of these non-specialist services may vary and pathways are not always in place.10
To gain an understanding of the difficulties that are faced, as well as identifying opportunities for service development, the University of Cambridge Institute for Manufacturing Education and Consultancy Services employed the Institute for Manufacturing (IfM) strategic roadmapping11 method with a selection of regional stakeholders in paediatric neurorehabilitation. While this methodology has been used extensively in industry settings previously to identify and solve areas of difficulty,11 this is the first report in the medical literature of its use.
Methodology
The IfM strategic roadmapping method is a workshop-based approach for the identification and exploration of challenges and opportunities within a system. Roadmapping methods are a way of bringing complex system level knowledge into a forum and translating them into a simple format such as a graph or table.12 These were originally piloted by Motorola to support strategic planning. However, they are traditionally difficult to manage due to the high level of expertise and tailoring required for each setting.11
The IfM roadmapping method is classed as a ‘fast-start’ procedure which simplifies the method into a more user friendly format without losing the strategic benefits it brings. The method used was the S-Plan workshop process as described by Phaal et al.11
Participants
The organisers of the workshop invited professionals in the region to gain a cross-section of the neurorehabilitation services in the region. Thirteen delegates attended from a cross-section of those involved with the patient pathway for paediatric neurorehabilitation. These included:
A Paediatric Neurology Consultant and Paediatric Major Trauma Rehabilitation Lead.
A Consultant Paediatric Intensivist, and Paediatric Major Trauma Lead.
A Consultant Paediatrician, and Lead for Paediatric Audiology.
Five Allied Health Professionals (two speech therapists, one physiotherapist and two occupational therapists) including coverage from acute and community services as well as specialist brain injury services.
A Community support officer from a leading charity working with children after neurological injury.
A Deputy director of NIHR Brain Injury Healthcare Technology Cooperative.
Two representatives of a private rehabilitation/care facility.
A Director of a Consultancy firm.
While these participants were largely self-selected, the coverage of organisations who work in the area was significant and provided useful perspectives.
Process
The process starts with a plenary ‘landscaping’ process activity, based on the following questions:
Why do we need to act (particularly with regard to developing needs)?
How can the patient pathway experience be developed to respond to those needs?
What enabling projects and resources are required to deliver that pathway experience?
The IfM landscaping process employs individual reflection, group discussion and voting to generate information and ideas, capturing and developing these on a large wallchart (visually highlighting potential gaps, links, opportunities and challenges prioritised by voting) (figure 1).
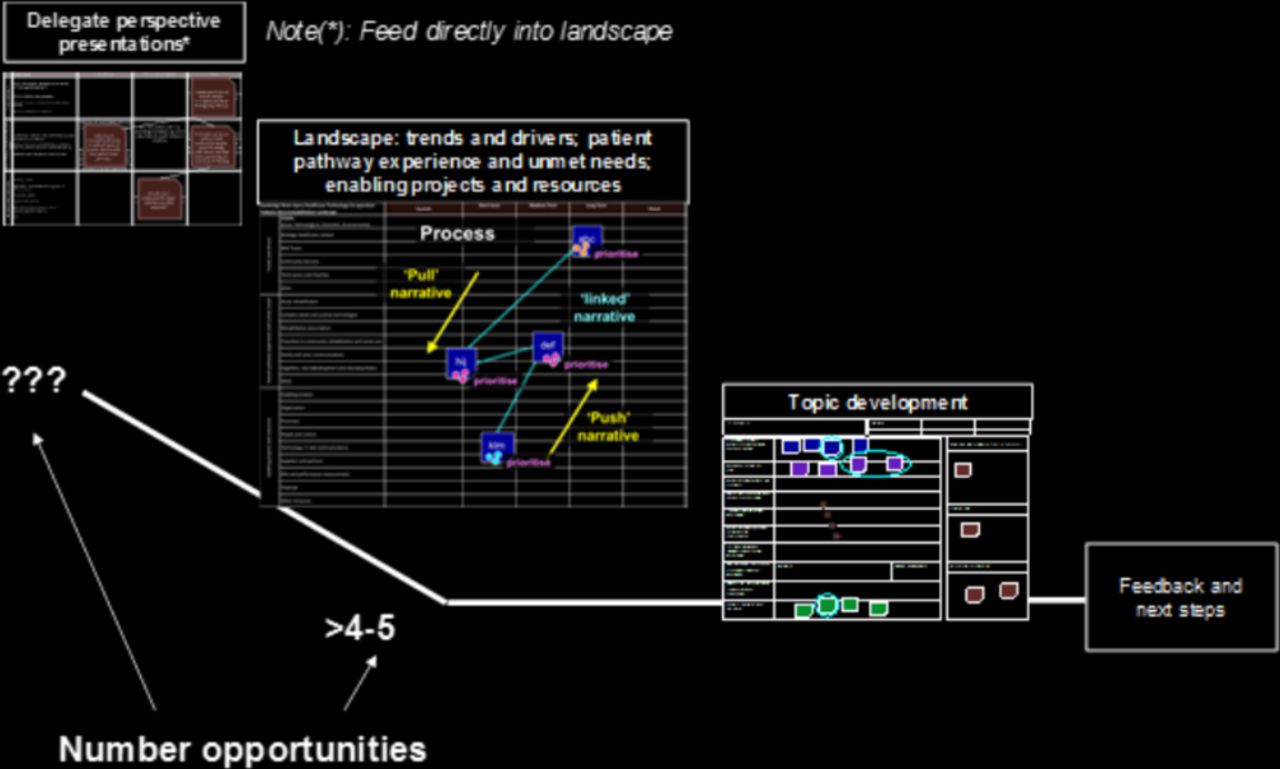
A diagram of the roadmapping process.
Three layers of ‘landscape’ are created: The first layer covers trends and drivers; the second patient pathway, experience and unmet needs; and finally, enablers and resources. The three layers of the landscape are aggregated to identify linkages and clusters (on a ‘linkage chart’), and hence possible priorities for action. In this ‘fast-pass’ version of the process, delegates prepared their individual narratives and then presented their key perspectives directly onto all three layers of the landscape in a series of 2–3 min ‘pitches’.
Prioritising the findings
Delegates collectively reviewed the importance of the items identified then voted on priorities for each layer. The facilitator and client lead then proposed which themes to investigate.
Having identified several priority opportunities by this method, delegates formed syndicate groups, each to develop one outline research or enabling project, using a ‘project proposal exploration’ template. In the final session, syndicates presented their findings for whole-group review.
Results
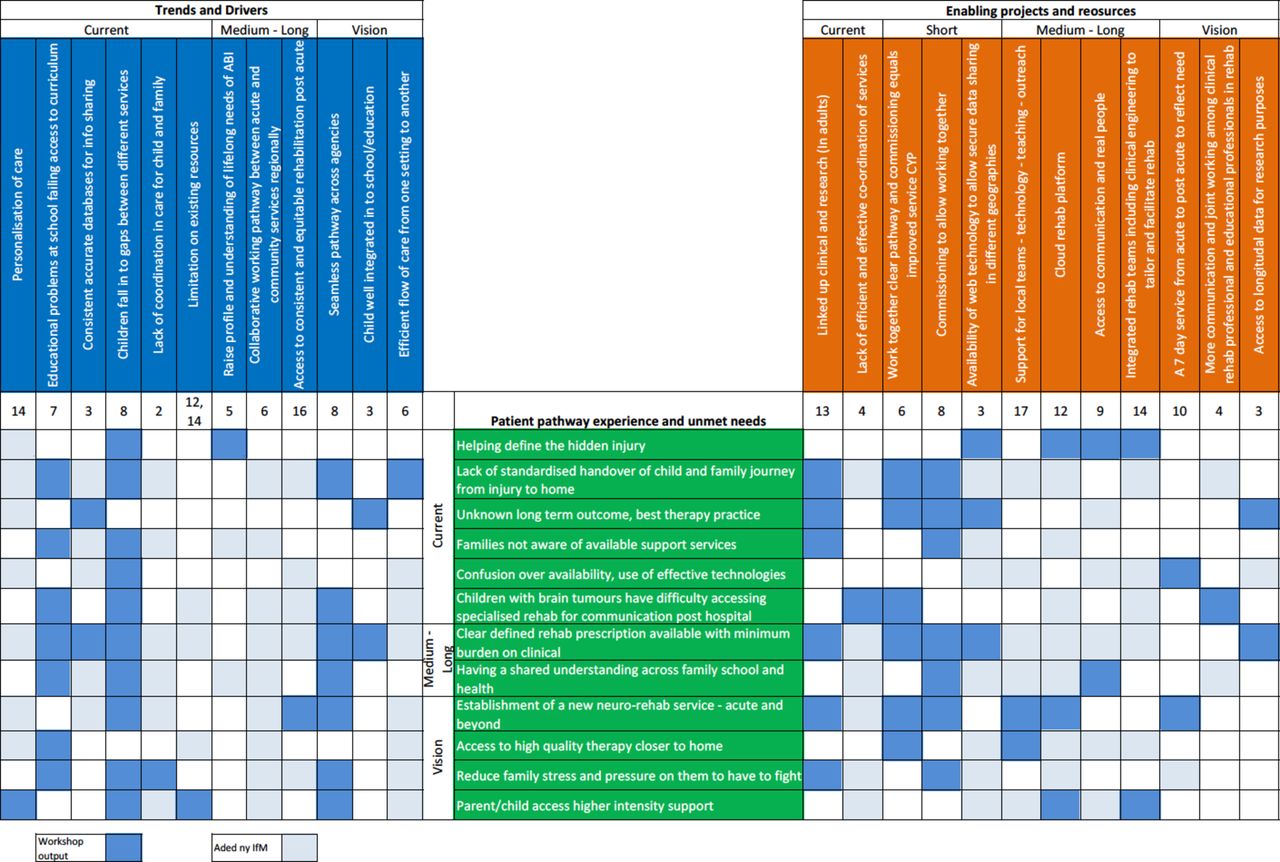
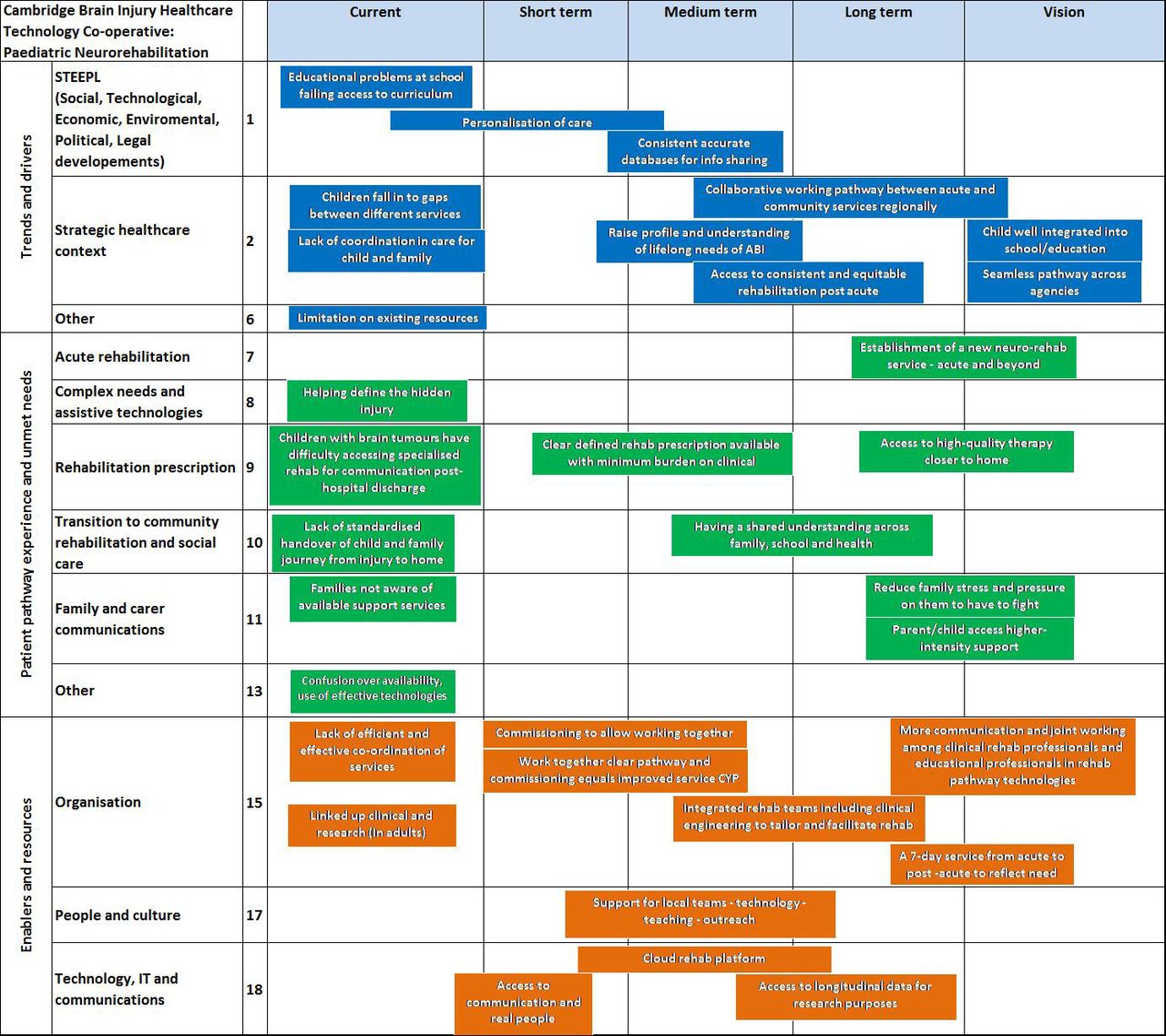
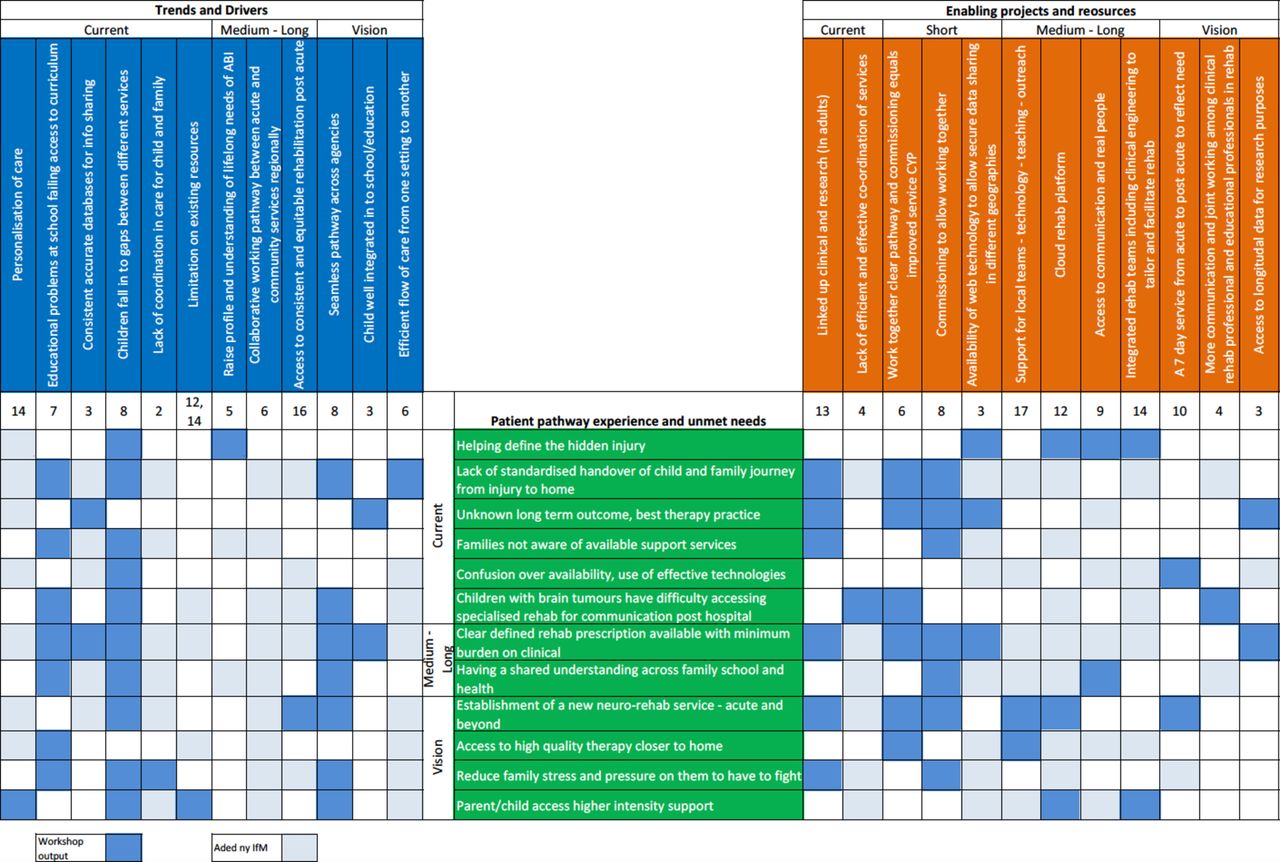
The process created a landscape of paediatric neurorehabilitation as seen by the delegates (figure 2). Areas of difficulty ranged from educational problems faced by children to lack of parental awareness of available support systems with opportunities such as health technology and visions for improved local joined-up services. Relationships were explored between the different layers of pathway experiences/unmet needs and (1) trends and drivers and (2) enabling projects and resources. A linkage chart was developed (figure 3).

Paediatric neurorehabilitation landscape. ABI, acquired brain injury; IT, information technology.
{kind=link}
{kind=link}
{kind=link}
Paediatric neurorehabilitation linkage chart.
Exploring priorities
Delegates voted on the priorities that should be explored. Four were selected and expanded on by teams of delegates.
Access to medical and therapy expertise close(r) to home
Shared understanding across family, school and health
Family and professional awareness of resources and support
Establish centre for rehabilitation technology evaluation, advice and coordination of services and research
Access to medical and therapy expertise close(r) to home
Delegates discussed the difficulties that patients and their families often have in travelling long distances for specialist care including medical and therapy input. This was identified as important due to an increased risk of entering the youth justice system, more difficulties with building relationships and the challenges children may have with the education system which are worsened by lack of access to local specialist services.
The outcome of a prompt and responsive outreach service in a hub and spoke design was the ideal with a strong emphasis on the education and development of local services. At present, there is no accurate directory of services either locally or nationally. Delegates identified the development of the key worker role for each patient and the identification and training of local hub contacts for services around the region would move the local services toward this goal.
The National Health Service (NHS) standard contract for Paediatric Neurosciences: Neurorehabilitation was an important resource as was local scoping data looking into current and ideal services and also the presence of the Brain Injury Health Technology Cooperative in order to facilitate the building of a cloud-based paediatric neurorehabilitation presence in the region. Barriers identified included: lack of information on current experience levels in the locality, funding, time and capacity for the current specialist team to develop this service.
Shared understanding across family, school and health
The second priority was seen to be the lack of understanding of ABI and ABI-related services among professionals and their families. The lack of one individual in charge of the care of these children was a significant gap in the patient’s journey. A lack of clear referral pathways to access services as well as handovers between professionals was a further difficulty. The importance of the family being able to access accurate and timely information and gaining support in returning to school were vital.
The outcomes envisioned are: a handover pathway process between healthcare, education and the family, and compulsory training on ABI for all education professionals. At present, teacher training does not cover ABI sufficiently, taking into consideration its frequency of occurrence; school nurse involvement is often unstandardised, and schools do not routinely have supportive input if the child has a mild or moderate brain injury.
Currently, training exists in the form of webinars and various online resources, but the development of an online training portal for people in the education sector was a better method to overcome this difficulty. Additionally, important information for this portal can be obtained from approaching families whose children have had brain injuries to identify what problems they have found about information sharing.
Family and professional awareness of resources and support
The third priority focused on the lack of awareness of support structures already available in the region. Delegates felt that families often missed out on vital support due to the lack of a central database of services. Currently, individual clinicians have knowledge of specific services with anecdotal evidence of their effectiveness. Due to the lack of central organisation, occasionally, there is duplication and there is no formal way to identify gaps in provided services. These gaps in information hamper the development of new services.
The development of a streamlined, searchable and regularly updated database of services available to children and their families with a means of auditing their effectiveness was the final outcome of this. As well as improving the access to resources, delegates felt it would reduce morbidity and empower families and professionals. Delegates felt they were unable to recommend services to families as they are unsure about what is currently available and what auditable benefits are present for families.
Currently, cloud databases focus on the management of clinical aspects of trauma patients. The setting up of a regional pilot of a database of appropriate services was the next step, with identification of funding streams and working group members seen as vital.
Establish centre for rehabilitation technology evaluation, advice and coordination of services and research
The final priority explored was focused around the understanding of, and access to, technological services in childhood ABI. The aim of this stream was to be able to answer patients’ and parents’ questions around the best technologies, at the best time for the best outcomes in this patient group. The current evidence base was poor and often not related to this cohort.
Delegates saw the development of a centre of excellence to evaluate rehabilitation technology as an outcome, with appropriate access to personnel, clinicians with special interest, facilities and a database of these technologies. It was felt that this would enable professionals to personalise patient care by accessing the right tools at the right time for the right patients to improve outcomes.
Currently, there is no systematic method of evaluating technology in the paediatric neurorehabilitation population. There is also little joined-up working between clinicians and technology professionals to enable pertinent problems to be addressed. Difficulties of funding were a particular barrier to this priority, especially with regard to demonstrating value to commissioning bodies in the current health economy.
Discussion
The use of the roadmapping tool enabled professionals to identify gaps in the paediatric neurorehabilitation provision. These gaps were then prioritised and current practice, facilitators, barriers and outcomes were identified. While this is the first time these have been documented in this way, the priorities identified do link with the current understanding of best practice.
The provision of care local to patients is controversial at present.13 Current squeezes on health budgets as well as a drive for specialisation of clinical expertise have meant that patients and their families often must travel long distances for their treatment.14 This is particularly true in paediatric neurorehabilitation where small patient numbers have traditionally meant that patients with severe disability often must travel across the country to access specialist services.9 The disruption that this can cause a family and the possibility of this disruption worsening the patient’s outcome have become a growing concern.15 There is a growing understanding of the effects that even ‘mild’ neurological trauma can have on a child, which has led to an appreciation of the importance of longer-term specialist follow-up of the larger number of children who appear functionally able.16 This has led to the need for further development of high-quality local services for these children and their families. While this is difficult especially in areas with lower population density, services have found the use of a hub and spoke type system highly effective17 and delegates identified this as a possible model for future development.
The return to school is often seen as a central goal for children after a neurological injury.18 This return is a significant landmark of normality and is also where many children will access their rehabilitation therapies. There are however significant barriers to this return and the outcomes are often far from ideal.19 One of the most repeated difficulties that families and students themselves report is the lack of knowledge of ABI within the educational sector. Parents and the child can find themselves constantly explaining that the child has difficulties with professionals and peers who have poor understanding of the behavioural, emotional and cognitive difficulties children may have as well as appropriate strategies to manage this.19 The provision of an online training package for professionals and an active development of the special educational needs coordinator (SENCO) role in this area therefore may provide an important point of knowledge to support the child in returning to school.
The appropriate identification and signposting of resources is a constant challenge in a dynamic and fluid health economy.20 The impact this has on patient experience and use of health resources has been well documented.21 The provision of an up-to-date database could lead to significant time saving to professionals as well as parents. The addition of a mechanism for auditing the effectiveness of these services would also provide a method of constant service evaluation and source of data for research questions in an area with a sparse evidence base.22 Such databases, however, require constant maintenance and the development of a nationwide system would be a considerable challenge and would require a significant investment. A regional pilot would therefore be indicated as a proof of concept and funding would be required to achieve this.
The development of a similar facility to audit and evaluate rehabilitation technology is another priority identified by the delegates. Again, this is likely to require designated funding to achieve a meaningful result. The benefits that technology has brought to various health sectors have been well documented,23 and this investment may lead to significant savings in the future both in terms of cost and morbidity. Rehabilitative technologies have been hypothesised to be of considerable benefit to patients after neurological insults and have been shown to be of advantage in adult patients, but the evidence in children remains poor.10 A centre to routinely audit and evaluate these technologies and to provide leadership in the use of these emerging techniques currently does not exist. The identification of a suitable location and team would again require an investment of funding but would be likely to deliver cost savings and improved outcomes in the future.
While roadmapping techniques have been used extensively in manufacturing and business,24 their use in medical care has not been documented previously. As well as providing useful insights into the current state of services and priorities for development, this paper provides a demonstration of the use of roadmapping. Efficiencies and improved outcomes have been shown in other contexts.25 It is likely, as health sectors become more pressured due to increased demand and limited resources, that techniques such as these will become more commonplace not only at a commissioner level but also led by clinician collaborations such as the one described in this paper.
Strengths and limitations
The use of a systematic and evidence-based technique to identify gaps and opportunities provided this investigation with considerable methodological strengths.11 Delegates were invited based on their knowledge of local services as well as expertise in treatment of the population group or applicable techniques. This diversity provides an improved validity of the results presented. The systematic production of a visual map followed by prioritisation and further development by delegates provides a transparent method of identification of service deficits and methods to improve them with targeted outcomes.
While a widespread of delegates was present, the absence of a parent or patient’s representative was conspicuous. Roadmapping techniques in the manufacturing sector have been limited to those who have been seen to have a strategic knowledge of processes. Consumers in the manufacturing sector differ from those in the health sector. In the health sector, patients and their families often take on the role of the ‘expert patient’ and have a detailed viewpoint of health systems which often differs from those of professionals25 and can be considered at a strategic level. The understanding of the importance of the involvement of patient and public in service development is becoming increasingly understood26 and their inclusion might well have provided different perspectives to those that were stated.
Conclusion
Using the IfM roadmapping procedure, a list of priorities for service development in the field of paediatric neurorehabilitation has been developed. While investment would be required to achieve these benefits, the contribution that they may have to patients’ and families’ experiences and outcomes is considerable. The use of the IfM roadmapping procedure has been shown to provide useful insights in a health sphere and this technique should be considered for all services that are looking to identify areas of difficulty and ways to improve their patient care.
Acknowledgments
This article would not have been possible without the contribution of the delegates who attended the exercise. Their knowledge and expertise provided valuable insights which will guide future service planning and patient care.
This article was commissioned by the National Institute for Health Research (NIHR) Brain Injury Healthcare Technology Co-operative. The views expressed are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health.
References
Footnotes
Contributors CH wrote the first and subsequent drafts. All authors contributed to drafts. AM is the Paediatric Rehabilitation theme lead and led the workshop described. AG and RP assisted with the use of and analysis of the IfM Roadmapping Process. MB provided project management coordination as well as facilitation of the workshop. JP provided oversite and review of the project and organisation of the work group.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement All pertinent data have been included in this paper. A full report is available for review on request from corresponding author.