Article Text

Abstract
Background Successful development of a novel medical device requires an early understanding of anatomical feasibility and acceptance by both patient and clinician. In the absence of acceptable artificial anatomical test models, short-term evaluation with controlled observation in a small number of patients can be pursued to demonstrate initial feasibility. The vaginal bowel control (VBC) system, a non-surgical device for faecal incontinence (FI), is difficult to evaluate in artificial models. In-person usage was required to understand the potential for a vaginal insert to provide comfortable, dynamic rectal occlusion.
Methods This prospective, open-label study was conducted at a single urogynaecology practice at an academic medical centre with 13 female subjects ≥18 years with self-reported FI. The VBC therapy consists of a vaginal insert and pressure-regulated pump. The vaginal insert includes a balloon that, when inflated, creates an occlusion of the rectum. Subjects’ FI symptoms were collected in a baseline questionnaire. The investigator fitted subjects with multiple sizes of VBC inserts and evaluated the fit, position and degree of rectal occlusion. Subject comfort levels were assessed throughout the fitting process with a verbal response and on a subject questionnaire using a 10-point scale (1=no discomfort, 10=extremely uncomfortable). The insert was returned at the end of the study visit.
Results The majority of the rectum was occluded in 77% of patients. Furthermore, comfort scores during insertion (2.1±2.0), inflation (3.3±2.6) and ambulation (2.6±2.0) states indicated minor discomfort with 42% of women indicating no discomfort in any states. No adverse events were reported.
Conclusions Pilot evaluation of an early VBC system design and its delivery during a single study visit provided evidence for effectiveness, patient comfort and ease of use of a novel VBC for FI in women. This first-in-woman study confirmed feasibility of VBC and informed continued product development and subsequent clinical research.
- feasibility study
- fecal incontinence
- vaginal bowel control system
- accidental bowel leakage
- fecal urgency
- vaginal insert
Statistics from Altmetric.com
- feasibility study
- fecal incontinence
- vaginal bowel control system
- accidental bowel leakage
- fecal urgency
- vaginal insert
Introduction
Faecal incontinence (FI), also referred to as accidental bowel leakage, is the involuntary loss of solid or liquid stool that can be both physically and psychologically debilitating. Women with FI often suffer from social withdrawal and hygiene problems.1 It is a complex disease that can result from abnormalities in the coordination between the anal sphincters, pelvic floor function, stool consistency, rectal compliance and neurological function.2 3 In women, FI is often due to damaged or weakened anal sphincters which can result from childbirth,4 reduced pelvic floor function, disturbed rectal sensation or decreased rectal capacity.5
Prevalence rates in community-dwelling women in the USA are estimated to range from 12% to 25% with the average age of onset between 47 and 55 years.4–7 About 5%–10% of women report one or more FI episodes each month.8–10 The prevalence of FI is expected to increase significantly as the population of the USA continues to age.11
Conservative treatment options for FI include dietary changes, medications, pelvic floor muscle training and anal plugs. However, prospective observational studies report that <25% of patients describe adequate relief with conservative management intervention.12 13 Anal plugs provide a conservative and low-risk option for patients, although many experience discomfort or an increased sensation of faecal urgency while wearing a plug.14 15 In patients who have failed conservative therapy, surgical options include sphincteroplasty, sacral nerve stimulation, injection of bulking agents and placement of an artificial sphincter. Surgical treatments for FI can be costly, invasive and can require complex management or the need for additional follow-up. Furthermore, surgical intervention is associated with a 30%–50% failure rate during long-term evaluation.16–22 When all other options have failed, faecal diversion is a surgical option of last resort (for review, see ref.23).
Given limitations in existing therapies, an unmet medical need remains for new, effective and minimally invasive treatments for FI. The vaginal bowel control (VBC) system is a novel vaginal insert that dynamically deflects the rectovaginal septum to occlude the rectum and prevent bowel accidents. The device can be easily fitted in the clinic, then inserted, controlled and removed by the patient. This therapy fills a gap in the continuum of treatment for FI between conservative therapy and invasive surgery.
Introduction of a new medical technology requires clinical studies to mitigate key technological risk, such as safety, effectiveness, mechanism of action or patient adoption. Prior to testing in humans, feasibility work is often necessarily completed on artificial (ie, bench-top) models of relevant anatomy, cadaveric models and/or animal models to develop confidence that the device will mechanistically function as intended. However, since the function of the VBC system relies heavily on the specific anatomy of the human female pelvis, such models could not provide sufficient insights into device performance. Artificial models do not exist that accurately simulate the complex and highly adaptable morphology and tissue compliance of the vagina, rectum and surrounding structures, and all these aspects of the anatomy vary from patient to patient. While cadaver studies provided some use in the prototyping of device concepts, utility was limited due to the lack of muscle tone in non-living tissue and the lack of feedback on comfort and tolerability. Finally, no animal has sufficiently similar vaginal and rectal anatomy to justify its use as a model. Therefore, a study was designed to bridge this gap by allowing a closely controlled, acute evaluation of the device’s mechanical action (dynamic occlusion of the rectum) and patient tolerability under the administration and continuous observation of a physician. In this way, the basic premise of the device—a comfortable vaginal insert that could safely create an occlusion in the rectum—could be vetted prior to initiating clinical studies that could evaluate the clinical effect of this occlusion on FI symptoms, which requires longer-term daily use of the device.
Success of this new therapy would require the device to be comfortable, occlusive and appealing to patients. The objective of this initial first-in-woman study was to understand if the VBC could be comfortable while providing a substantial amount of reversible (dynamic) occlusion to the rectum, as well as to assess patients’ attitudes towards the therapy. This initial feasibility data and insight could then inform subsequent device development, clinical protocol development, data collection tools, clinical trial planning, and patient and physician education. Specifically, these results provided the foundation for recently reported clinical studies that describe the safety and efficacy of the VBC system (Eclipse System, Pelvalon, Sunnyvale, California, USA) as a low-risk and patient-accepted approach to treating FI (LIFE clinical trial24 25).
Materials and methods
This was a single-centre prospective, open-label clinical study approved by the Stanford University Institutional Review Board (IRB) for Human Subjects Research conducted from March 2011 June 2011. The study included consecutive enrolment of female subjects at least 18 years of age presenting to the Urogynaecology clinic at a university academic medical centre with complaints of FI, defined as at least one stool leakage (solid or liquid) episode per month, who were willing and able to give informed consent to participate. Subjects were recruited solely from within the investigator’s existing practice. Study exclusion criteria included the presence of genitourinary fistulas, tumours or anastomosis; wound or tear in vagina or rectum; and vaginal infection. Also excluded were pregnant women or subjects with any significant medical condition or factor that the physician believed would interfere with study participation and/or increase risk.
The VBC system is a novel, non-surgical and minimally invasive treatment for FI, which consists of a vaginal insert and hand-held, pressure-regulated pump. The vaginal insert includes a balloon that, when inflated, creates an occlusion of the rectum. This dynamic mechanism allows the patient to control her own bowel movements. When inserted, the vaginal insert rests in a similar position as a diaphragm or vaginal pessary.
Once consented, subjects were seen for a single clinic visit during which demographics, medical history and questions regarding subjects’ FI symptoms were collected in a baseline questionnaire. All evaluations were performed by single practitioner. A standard pelvic exam (vaginal speculum and digital rectal) was performed to assess the subject’s pelvic health prior to the initial fitting. During the fitting, the physician inserted the device into the patient’s vagina, assessing the fit and position of the insert. A digital examination was done to measure vaginal width and length as well as the clearance of the insert, both vaginally and rectally. Subjects were fitted with multiple sizes of inserts (45–57 mm base width, 65–85 mm base length) during their study visit to determine the most appropriate configuration.
In addition to degree of rectal occlusion during insert inflation, a primary outcome of this study was device comfort. The insert was assessed while deflated, during inflation, after inflation and after various types of subject movement (eg, sitting, standing and ambulating). The subject was orally queried regarding their comfort level at various stages throughout the fitting process, providing feedback using a 1–10 point Likert scale (1 = ‘no discomfort’, 10 = ‘extremely uncomfortable’). Comfort was also verbally assessed on a binary scale (comfortable vs uncomfortable) with the balloon inflated to pressures of 50, 100 and 150 mm Hg to determine tolerability. At the end of the visit, subjects returned the study device.
As this was a single-visit study designed to assess concept feasibility, no objective measures of device efficacy were collected. Patients were asked to complete questionnaires related to FI symptoms and future device usage. Due to the nature of qualitative data, descriptive statistics were used to summarise study results. Comfort scores after vaginal insert placement and inflation were analysed using analysis of variance with repeated measures with post hoc pairwise comparisons to the deflated state.
Results
Thirteen subjects were enrolled from 28 February 2011 to 22 June 2011. Prior hysterectomy was present in 62% (8/13) of subjects. The mean age of subjects was 70.7 years with a range from 40 to 90 years. Two subjects did not complete questionnaires, thus data regarding FI symptoms and device usage are presented for 11 subjects for descriptive purposes.
At study initiation, five subjects (5/11; 45%) reported experiencing solid or liquid stool leakage ≥2 times per day, five (45%) reported leakage ≥2 times per week and one (9%) reported leakage 1–3 times per month. Fifty-eight per cent (7/11) were not currently sexually active. Previous or current use of a vaginal pessary was reported in four subjects (4/11; 36%). All but one were determined to have stage 1–3 prolapse. A full list of subject demographics and baseline FI characteristics is included in table 1.
Subject baseline FI characteristics
During the digital rectal exam, the physician made a subjective assessment of the percentage of rectal occlusion provided by the insert’s balloon when inflated. The majority (≥50%) of the rectum was occluded in 10/13 subjects (77%), with 54% (7/13) subjects achieving ≥75% rectal occlusion.
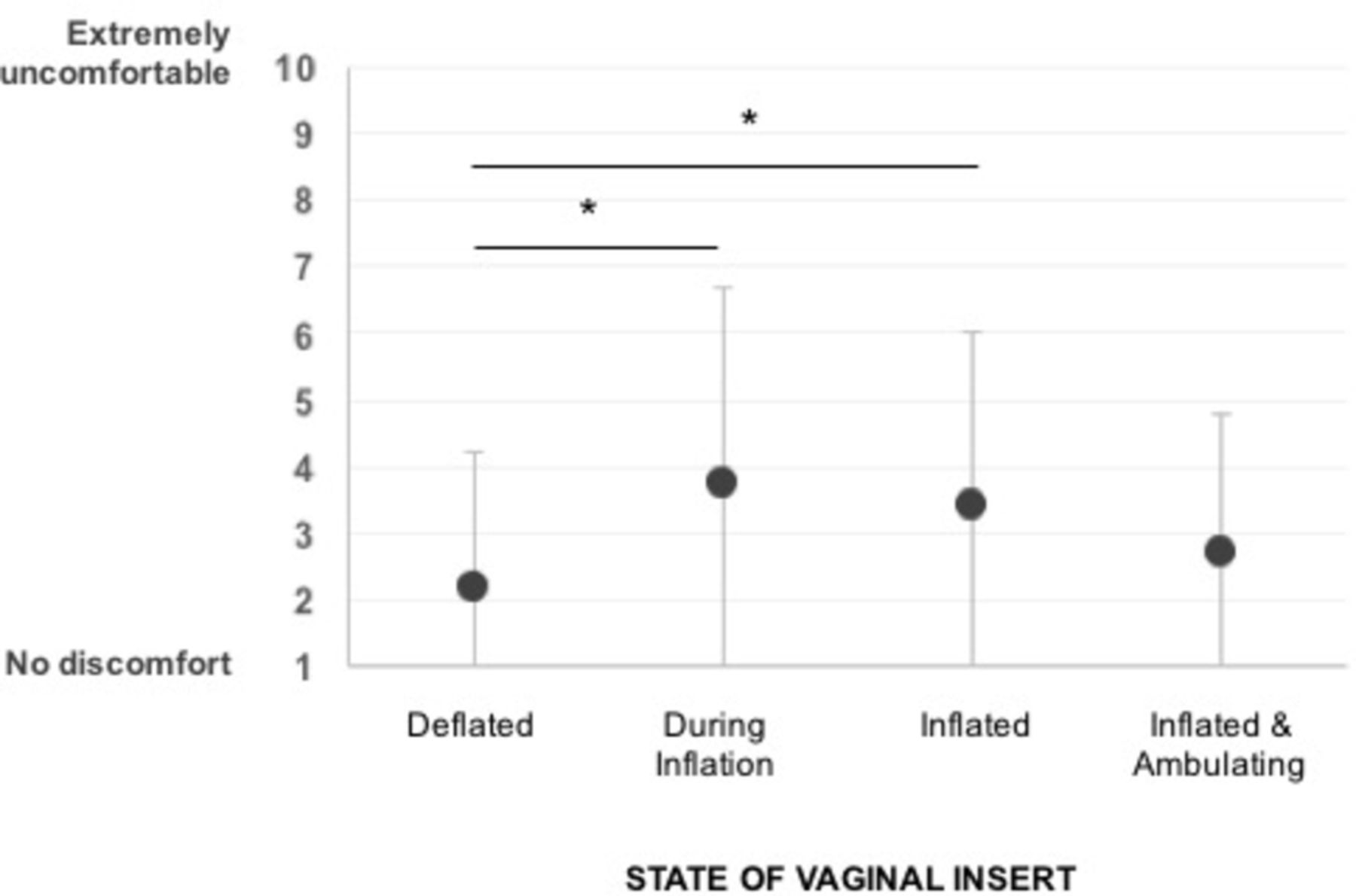
After initial device insertion, subjects rated their comfort level in different categories: after insertion (deflated), during inflation, post inflation and while ambulating on a questionnaire using a 10-point rating scale (1 = ‘no discomfort’, 10 = ‘extremely uncomfortable’). Oral responses from one subject were not obtained regarding comfort, thus comfort data are presented for 12 subjects for descriptive purposes. Mean discomfort level while deflated was reported as 2.2±2.0 (n=12) with eight patients (67%) reporting no discomfort (score=1) during the deflated state. A significant effect of the inflation action on comfort levels was found (F(3,33)=3.25, p=0.034), although comfort improved again with ambulation. Comfort decreased with inflation as represented by scores of 3.3±2.6 during inflation (p=0.024) and 3.5±2.9 post inflation (p=0.048), although scores remained on the comfortable side of the scale (<5). Further, discomfort during inflation and ambulation (2.6±2.0) was not significantly different from scores reported during the initial deflated state (p=0.309) (figure 1). Of 11 patients queried about comfort at various balloon inflation pressures, 11 (100%) were comfortable at 50 mm Hg and 8 (73%) were comfortable at both 100 and 150 mm Hg. Overall, five subjects (45%) reported a comfort level of 1, ‘no discomfort’, for both deflated and inflated states.
{kind=link}
Patient-reported comfort scores during inflation of vaginal bowel control vaginal insert. Patients indicated comfort levels during different states of vaginal insert inflation. * indicates statistical significance.
Subjects also reported on a number of device usage questions at the conclusion of their participation. As stated earlier, two subjects did not complete this portion of the questionnaire, thus data are presented for 11 subjects for descriptive purposes. The majority of subjects (9/11; 82%) indicated willingness to adopt the VBC system poststudy participation. Seven women expressed willingness to wear daily, with four women responding that they would wear the insert all day and night (4/7; 57%) and three indicated they would wear the insert only during the day (3/7; 43%). The remaining two subjects reported that they would wear the VBC insert only when outside the house or on special occasions. Eight subjects (8/11; 73%) said that they would continue long-term use of the device if it provided at least 50% improvement in their FI symptoms. There were no reported adverse events in any subjects.
Discussion
This initial case series provided the first evidence that the novel concept of a vaginal insert for FI occluded the rectum and was well-tolerated by women suffering from FI. Physician assessment of rectal occlusion established the mechanical functionality of the device, and subject-reported comfort levels established that the vaginal insert induces minimal discomfort. Although relative discomfort increased during inflation and post inflation of the insert, the insert was consistently comfortable throughout the study and initial comfort levels were restored during movement about the clinic. Although discomfort was minimal in all patients, these findings suggest that patients should be counselled prior to initial inflation to expect some pressure and care should be taken to inflate the insert slowly, verbally checking patient comfort through the inflation process.
The results further suggest that subjects may take time to acclimate to the placement of the insert. The fitting process requires a high level of clinician engagement to determine that an insert is both appropriately sized and comfortable for the subject. As Clemons noted in evaluating fitting of a pessary for pelvic organ prolapse or urinary incontinence, it is important to allow patients sufficient time to replicate day-to-day movements and activities while wearing the insert and to be persistent in finding the most comfortable fit for the patient.26 In subsequent research on at-home evaluation of the VBC insert, 96% of patients who used the insert for 1 month reported that it was comfortable, with half reporting they could not feel it.25
A common endpoint in clinical studies for devices intended to treat FI is the reduction of accidents by ≥50%.27 28 In many therapeutic areas, this reduction in symptoms would not be sufficient for patient adoption, but the correlation of this endpoint with quality-of-life improvements has been demonstrated.29 Patient reports in this study that they would continue to use the VBC system for long-term usage if it provided this improvement provided substantiation of this endpoint as a valid one.
This study was not intended as a rigorous outcome study of the intervention, but was instead designed to provide initial inputs required to design physician training and patient education, and to further the development of the device (box 1). In addition, this experience provided valuable understanding of how to study the device and fitting procedure, a necessary preliminary step in anticipation of subsequent studies. A subsequent pivotal study by Richter et al25 reported treatment success, defined as 50% of greater reduction of incontinent episodes from baseline to treatment, after 1 month of wearing the VBC insert in 86% of subjects from the Per Protocol Cohort. Additionally, approximately 90% of subjects were satisfied with their use of the insert and 98% would recommend it to a friend. Furthermore, Varma et al30 have described that the use of the VBC insert for 1 month was associated in improved bowel function in women as reported by decreased frequency of bowel movements, improved stool consistency, less urgency and more complete evacuation.
1 Key findings to inform clinical protocol and trial design
Device fitting
Prior to initial inflation, patients should be counselled to expect some pressure.
Care should be taken to inflate the insert slowly, verbally checking patient comfort through the inflation process.
Subjects may take time to acclimate to the placement of the insert.
Encourage replication of day-to-day movements to determine comfortable fit.
Establish clinician–patient engagement in clinic that extends to home to ensure that an insert is both appropriately sized and comfortable for the subject.
Outcome measurement
Use standard in-office questionnaire and bowel diaries to capture patient perspective on treatment success.
50% improvement in faecal incontinence symptoms is acceptable to patients as a measurement of therapy success.
This feasibility study was limited by number of subjects, duration of time that patients experienced the VBC insert and evaluation of rectal occlusion from a single assessor. Although this was a small patient population, the general female FI population was well-represented with a large age range of subjects, various FI baseline characteristics (characterised by episode urgency and frequency, stool consistency and symptom history) and diverse vaginal anatomies including hysterectomised and non-sexually active women. Furthermore, the goals of this first-in-woman study to assess comfort and rectal occlusion of the VBC vaginal insert and to gain feedback from patient and physician were achieved during a single patient visit, informing next steps in device design, clinical delivery and evaluation.
This is the first time that a vaginal device has been implemented to provide bowel control. Although vaginal devices have long been used for other therapeutic purposes such as pelvic organ prolapse31 and stress urinary incontinence,32 manipulating the rectovaginal septum to provide rectal occlusion is a novel concept. Given the safety precedence of other similar vaginal devices such as pessaries which are intended for long-term use,33 34 this therapy falls on the less-invasive end of the FI treatment continuum. Further research of the VBC therapy has corroborated this notion—a larger study25 reported that there were no serious device-related adverse events up to 3 months of continuous insert wear. A multicentre, prospective, open-label, 1-year outcome clinical study is ongoing.35
In conclusion, this structured, succinct, in-clinic evaluation provided evidence that a novel VBC therapy for FI was well tolerated, introduced minimal discomfort and provided rectal occlusion. This pilot study was a cost-effective approach to gather critical information on device function as well as assess device features and qualitative feedback from physician and patient that would influence clinical adoption. Insight gathered here provided the foundation for recently reported clinical studies that describe short-term safety and efficacy of the VBC system (Eclipse System), validating the VBC system as a low-risk and patient-managed approach to treating FI (LIFE clinical trial24 25).
Acknowledgments
None
References
Footnotes
Contributors ERS planned the study in conjunction with the sponsor, Pelvalon, conducted the study, created the report and is responsible for the overall content as guarantor.
Funding This research was funded by the Wallace H. Coulter Translational Research Grant.
Competing interests ERS has received stock options in Pelvalon.
Ethics approval Stanford University Institutional Review Board (IRB) for Human Subjects Research.
Provenance and peer review Not commissioned; externally peer reviewed.