Article Text

Abstract
Background To develop a new accelerated in vitro model that has implications for investigating the mechanism of biliary stent occlusion and help in the development of new materials that can alleviate this problem.
Methods We employ a combination of reconstituted animal bile, bacteria and cellulose fibres optimised to reproducibly generate accelerated occlusion of stents, and produce occlusions that closely mimic those found in clinical studies.
Results Our model affords repeatable, highly accelerated occlusion (within 2–3 days, compared with between about a week to 2 months in previous models). Our results highlight the role of dietary fibre in blockage of stents and demonstrate their importance in the onset of occlusion.
Conclusions This accelerated model may have implications for developing biliary stents with enhanced patency.
- gastrointestinal
- biliary stent
- in vitro model
Statistics from Altmetric.com
Introduction
Stents are used in the treatment of numerous biliary tract diseases, ranging from benign biliary diseases to malignant strictures. Two types of biliary stents find extensive use: plastic Amsterdam-type stents and self-expanding metallic stents. The more commonly used Amsterdam-type plastic stents are tubular structures with diameters ranging from 7 to 12 Fr. Further increase in the diameter of plastic stents is precluded by the working channel diameter of side-viewing endoscopes. The major limitation of these plastic stents is their limited patency (with an average time of failure of 82.7±5 days). The primary reason for failure is complete obstruction of bile flow due to occlusion by biofilm and biliary sludge.1 The obstruction rate was found to be 27% in the first 30 days of plastic stent deployment.2 The risk of occlusion increases progressively after 3 months with a median patency of 4–5 months.3 Nevertheless, plastic stents are widely used because of their low cost and their ease of removal when occluded for replacement by a new stent.4
The alternative to plastic stents is self-expanding metal stents that are made from shape memory alloys like nitinol and can expand up to three times their original diameter after deployment in the biliary tract. Self-expanding metallic stents are expensive, but offer several advantages. Their larger diameter allows them to remain patent for periods exceeding 6 months, before they become completely occluded.5–7 Tissue growth through the meshwork of the self-expanding metal stents inhibits their migration. However, this poses a challenge if the stent needs to be removed and replaced. Thus, a gap exists in terms of the cost, ease of operation and patency between plastic and self-expanding stents. Several groups are, therefore, investigating polymeric/composite stents that could bridge this gap.8–11
Screening a range of materials to develop better stents necessitates fast-throughput, reliable in vitro models (IVM) for investigating stent occlusion. A few IVMs (table 1) have been reported to investigate the nature of occlusion in plastic stents.12–16 We note that many of these reported IVMs (table 1: IVMs 1, 2, 5) employ physiological human bile. This poses technical challenges in ensuring reproducibility in stent blockage due to person-to-person variation in bile characteristics. While animal bile has been used in a few IVMs, these models reported occlusion times exceeding 28 days which are not suitable for rapid screening. Surprisingly, none of the reported studies used dietary fibre as a constituent of the fluid circulated through the stent though it has been implicated as one of the reasons for stent occlusion.13 In summary, the existing IVMs either do not lend themselves to accelerated studies of occlusion (required for new device development) or they do not mimic conditions that cause stent occlusion in patients with biliary diseases.3 16 Thus, there is a need for a new model for stent occlusion that allows reproducible accelerated occlusion and closely mimics the composition of biliary fluids and biliary sludge.
Comparison of experimental conditions of the existing in vitro models
A novel model would also help improve our understanding of the mechanism of stent occlusion. Most of the existing knowledge of stent occlusion is based on clinical investigations of discarded stents obtained from patients. Analysis of these data has revealed that occlusion is initiated by the formation of a bacterial biofilm.8 Subsequently, biliary ‘sludge’ forms, that is, a composite of bacteria, cholesterol crystals, calcium bilirubinate and palmitate, microbial by-products and glycoproteins.3 Further, biliary sludge is almost always observed to contain dietary fibre.17 These dietary fibres enter the stents since the sphincter of Oddi (that prevents food fibre from entering the common bile duct in healthy individuals) is compromised by stent insertion through the sphincter and/or by biliary sphincterotomy. We note that studies of stent occlusion have been performed on a variety of Amsterdam-type stents including those with side holes. The formation and morphology of occlusion, however, appear to be largely independent of these details in stent construction.
Here, we present a new accelerated IVM that is suitable for high throughput screening of novel stent materials. Our model includes dietary fibres in the simulated bile that results in sludge that is reminiscent of that extracted from human patients and that exhibits reproducible, highly accelerated stent occlusion.
Materials and methods
Medical grade Amsterdam-type plastic stents with different sizes were acquired from Biorad Medisys, India. Oxgall bacteriological grade bile (1 kg purified and solidified) was obtained from US Biologicals, USA. Dietary fibre (Jelucel PF 30, 90, 300) used in this study was obtained from Jelu-Werk, Germany. Glass bottles and stoppers used in this study were obtained from Borosil, India and Scott-Duran, Germany, respectively. Tygon tubing was procured from Tarsons, India. The minimal media (which included sodium chloride, dextrose anhydrous, magnesium sulfate heptahydrate, ammonium chloride, disodium hydrogen phosphate, potassium dihydrogen phosphate) was obtained from Merck Chemicals, USA. All glassware and constituents were autoclaved before the start of the experiment to maintain the sterility of the set-up.
Ten per cent ox bile stock solution was prepared by dissolving 100 g of as-received ox bile in 1 L of distilled deionised water from a Milli-Q system along with the essential nutrients present in minimal media. These were thoroughly dissolved to obtain a particulate-free reddish orange solution, which was transferred into beakers with adequate aeration. This was then autoclaved at high pressure (15 psi) and temperature (120°C) for sterilisation. After cooling, bacteria were introduced into the bile. Bile-resistant Escherichia coli from the strain ATCC2931 was developed by subculturing it in the aforementioned 10% bile solution for 10 generations. These strains were stored as stocks at −20°C. Bacterial stock was introduced into the autoclaved bile in a minimal quantity (150 µL for 300 mL) and they were allowed to grow for 48 hours at 37°C while shaking at 150 rpm. We introduced this into our set-up after the bacterial optical density (OD) reached 0.4–0.8. All the tubings in the set-up were autoclaved and sterilised before use. The bile containing growing bacteria, along with fibre, was used as the reservoir fluid and was pumped through the set-up to mimic the flow of biliary fluid.
Instruments
Shaker Incubator (Spectralab Instruments, India) was used for growing bile-resistant bacteria. The bile reservoir was kept in a shaking water bath (Equitron, India) at a controlled temperature of 37°C. Autoclave (Equitron) was used for sterilisation and decontamination. Peristaltic pumps were procured from Baoding Longer Precision Pump, China. The transfer of bacteria growing bile was performed in a laminar flow hood to maintain sterility. Optical densitometer from Eppendorf, Germany, was used for measuring OD. Dissection tools (blade, scalpel) were used to cut open the stents for assessment of the occlusion. Scanning electron microscopy (SEM) was performed using FEI ESEM Quanta 200-3D, USA. A small portion dissected from the clogged stent was fixed on a stub using carbon tape. Samples were gold coated before SEM. Stents were imaged at several places along their length.
In vitro model
In our IVM, bile reservoirs were connected to Amsterdam-type stents using autoclaved Tygon tubing. These reservoirs contained approximately 450 mL of bile infected with bacteria (grown to an OD of 0.4–0.8). A unique feature of our model is the inclusion of cellulosic dietary fibre. Through systematic studies, we have determined that addition of 2.5 g of fibre (average fibre length=90 µm) per 450 mL of bile resulted in reproducible occlusion of stents within 3 days. The reservoir containing all ingredients (bile+bacteria+fibre) was kept under constant shaking condition at 37°C. Shaking was controlled so as to prevent the settling of fibre and to prevent bile from frothing in the reservoir. The bile with bacteria and the fibre was drawn into the stents at a flow rate of 0.5 mL/min using a peristaltic pump. After flowing through the stent, the bile was recirculated to the reservoir. Bile flow in the in vitro set-up was monitored visually and the time taken for complete stoppage of bile flow was recorded. Occlusion was further investigated by dissecting the stents and observing the sludge adhered to the stent surface. All the experiments were performed with new, unused stents.
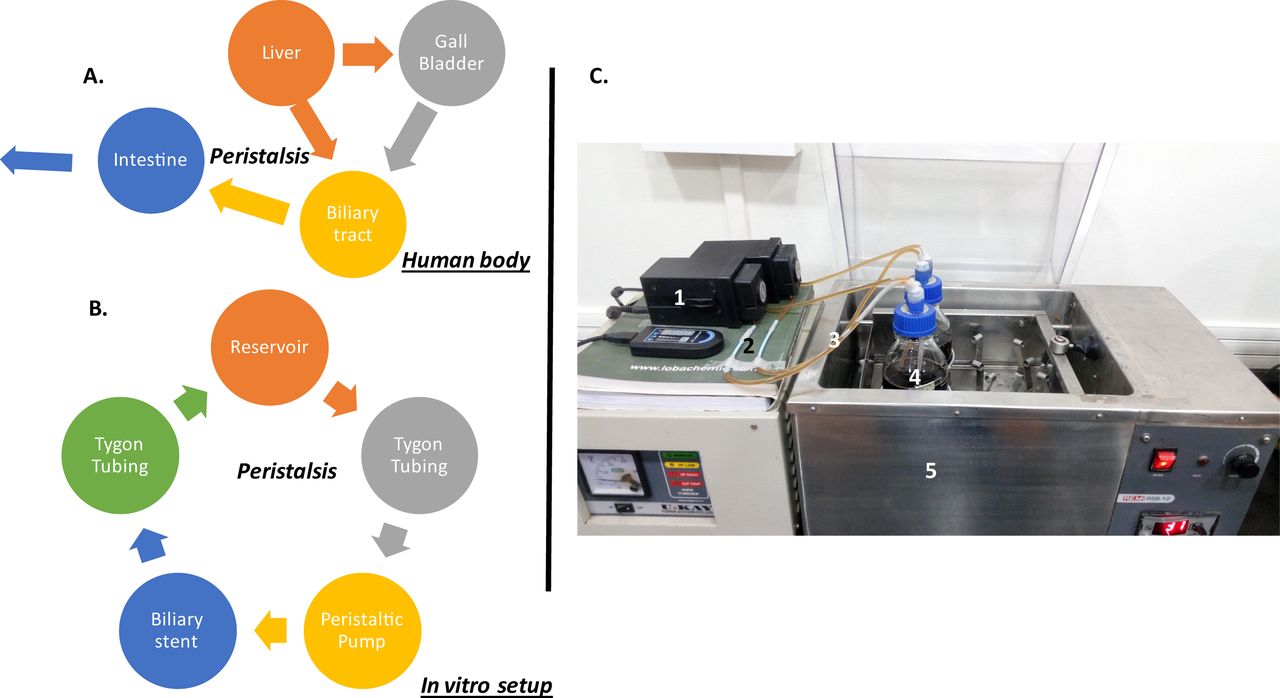
Comparison of natural biliary system with our in vitro set-up and the actual photograph of the in vitro set-up are shown in table 2 and figure 1.
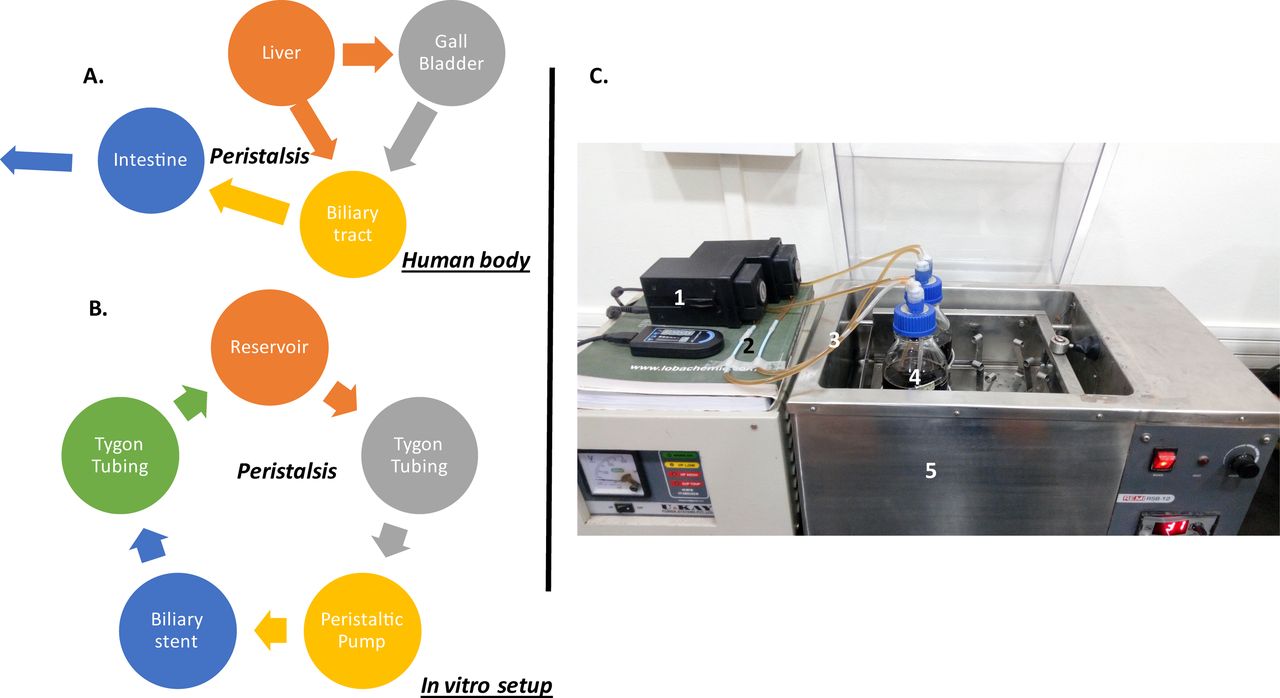
(A) The nature of the biliary flow in human body. (B) The flow chart of the biliary flow in the current in vitro set-up. (C) The actual photograph of the in vitro set-up: (1) peristaltic pump, (2) biliary plastic stents, (3) Tygon tubing, (4) reservoir, (5) shaker water bath maintained at 37°C.
Comparison of natural biliary system with our in vitro set-up
Results
Accelerated time scale for occlusion
We started our investigations by carrying out a series of control experiments (each of which was repeated using six fresh stents) using varying bile composition. In the first control experiment, pure bile (without bacteria or fibre) was allowed to flow through the stents. No occlusion was seen for flow of pure bile even when flow was continued for 5 days. We then performed an experiment by flowing bile containing bacteria and minimal media. In this case, too, no occlusion was seen after 3 days. After 3 days, the bacterial concentration declined—hence, we did not continue the experiment. For flow experiments where bile containing media and food fibre (without bacteria) was allowed to flow through the IVM, no stent occlusion was observed even after 3 days of the flow experiment.
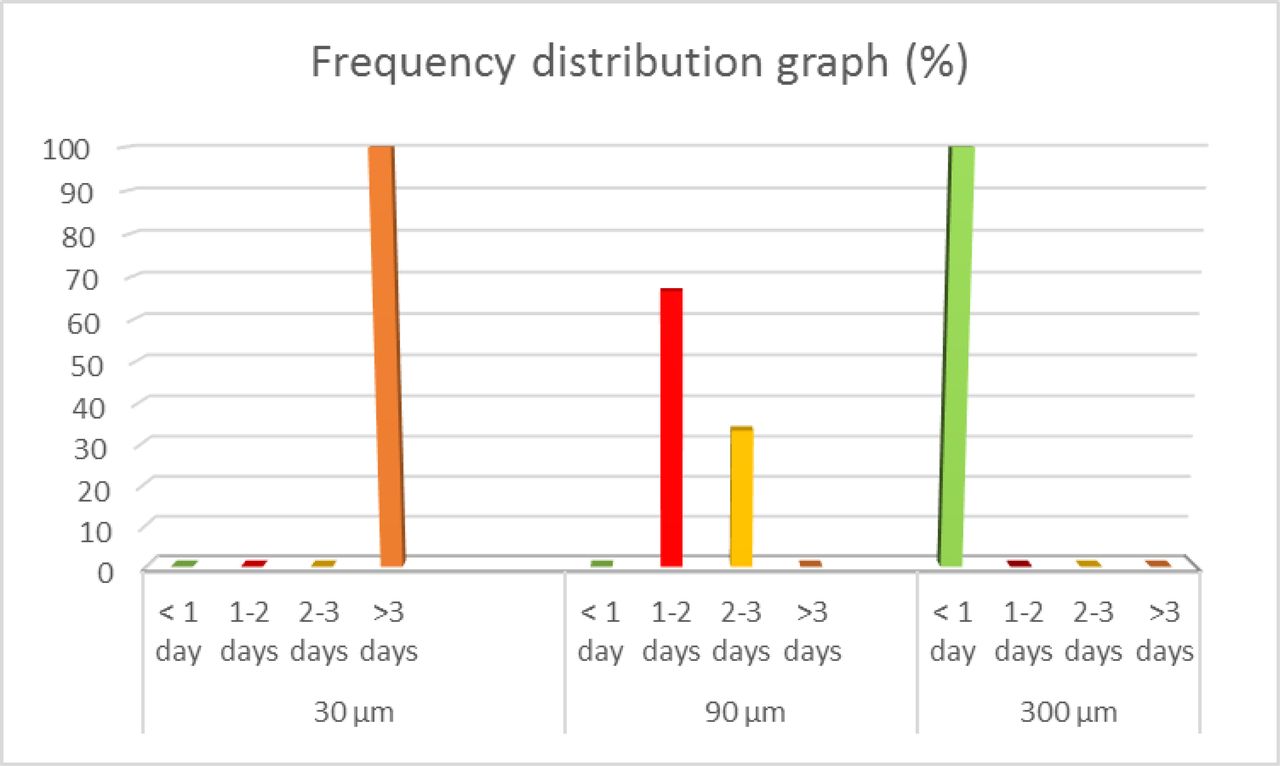
Finally, we allowed ox bile containing bacteria, minimal media and cellulose fibre to flow through the experimental set-up. It may be noted that the use of bile-resistant bacterial cultures is necessary to maintain adequate colony-forming units for biofilm development (online supplementary figure S1). The optimised biliary fluid composition that yielded reproducible stent occlusion within 3 days was as follows: 2.5 g of cellulose fibre/450 mL of bile, bacterial OD=0.4 and fibre length=90 µm. With these conditions, this experiment was repeated using 18 plastic stents with 10 Fr diameter. Of these, 12 stents were occluded within 24–48 hours while the rest were occluded within 48–72 hours (figure 2). As mentioned previously, occlusion was identified by complete obstruction of bile flow in the course of the experiments. Sludge formation that led to stent occlusion was seen exclusively inside the stents. No sludge formation was observed in the connecting Tygon tubing (that had a higher diameter than the stents) or in the bile reservoir.
Supplementary file 1
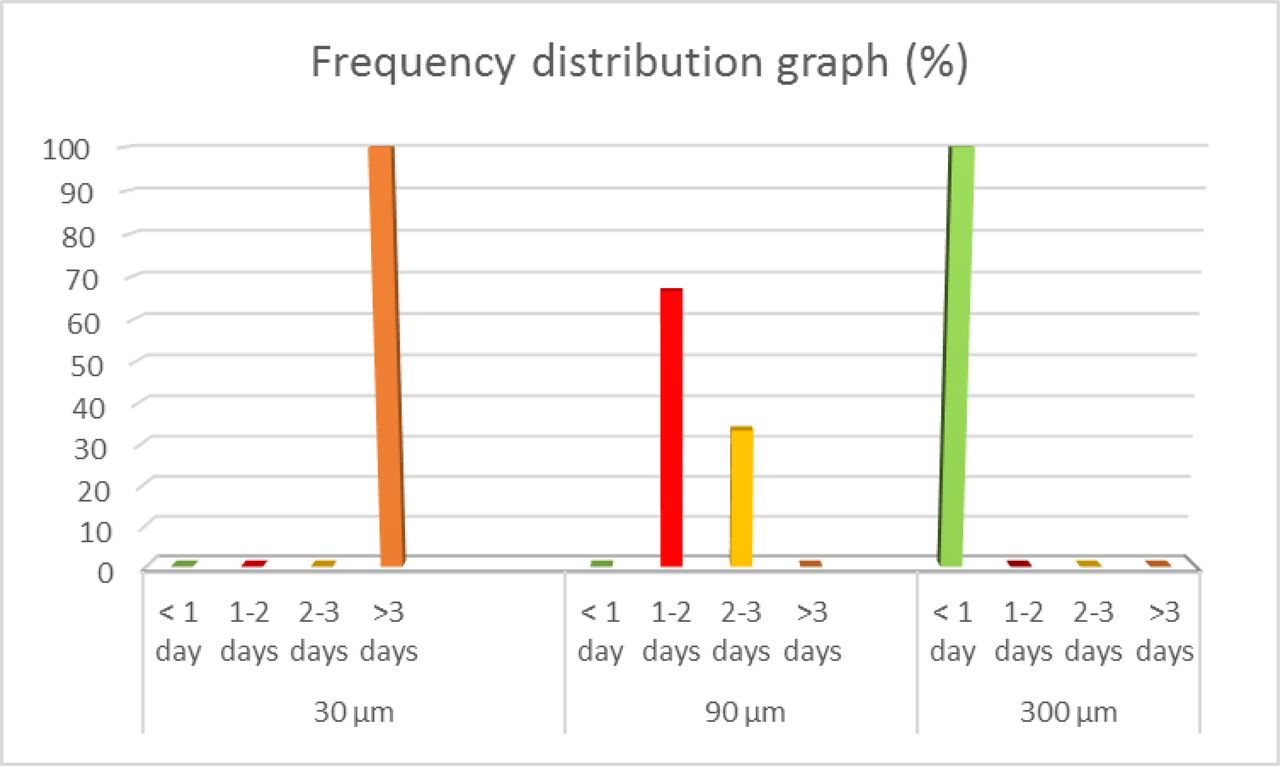
Dependence of clogging time on the length of cellulose fibre used. Time taken for clogging when (A) short (L=30 µm), (B) medium (L=90 µm) and (C) long (L=300 µm) fibres were used.
Effect of dietary fibre aspect ratio
We then performed flow experiments where we used cellulose fibre with different average lengths, viz 30 and 300 µm (compared with the 90 µm average length of the fibre used in the first set of experiments). Interestingly, we noted that in all stents through which the bile+bacteria with 300 µm fibre flowed, the stents were found to be occluded in less than 24 hours (figure 2). When experiments were performed using 30 µm length fibre, the stents were not blocked even after 72 hours (when the experiment was terminated due to declining bacterial concentration in the reservoir).
Morphology of occlusion
Having determined the reliability of the accelerated conditions for occlusion, we then examined the sludge formed inside the stents, both by visual observation and by SEM. In a recent study,3 stents retrieved from 148 patients were analysed to show that sludge deposition occurred at various axial positions along the occluded stents, with no specific preference for the location of the occlusion. Our results corroborate these findings. We observed that the stent occlusion occurs randomly along the length of the stent, with no preferred location for clog formation.
Further, we compared the site and nature of occlusion of stents used in our in vitro studies with those stents retrieved from the patients, in whom the stents were used for various indications and were retrieved after occlusion. Visual inspection of longitudinally dissected stents indicates that the nature of the occlusion in the IVM bears a remarkable resemblance to those in stents retrieved from patients (figure 3).
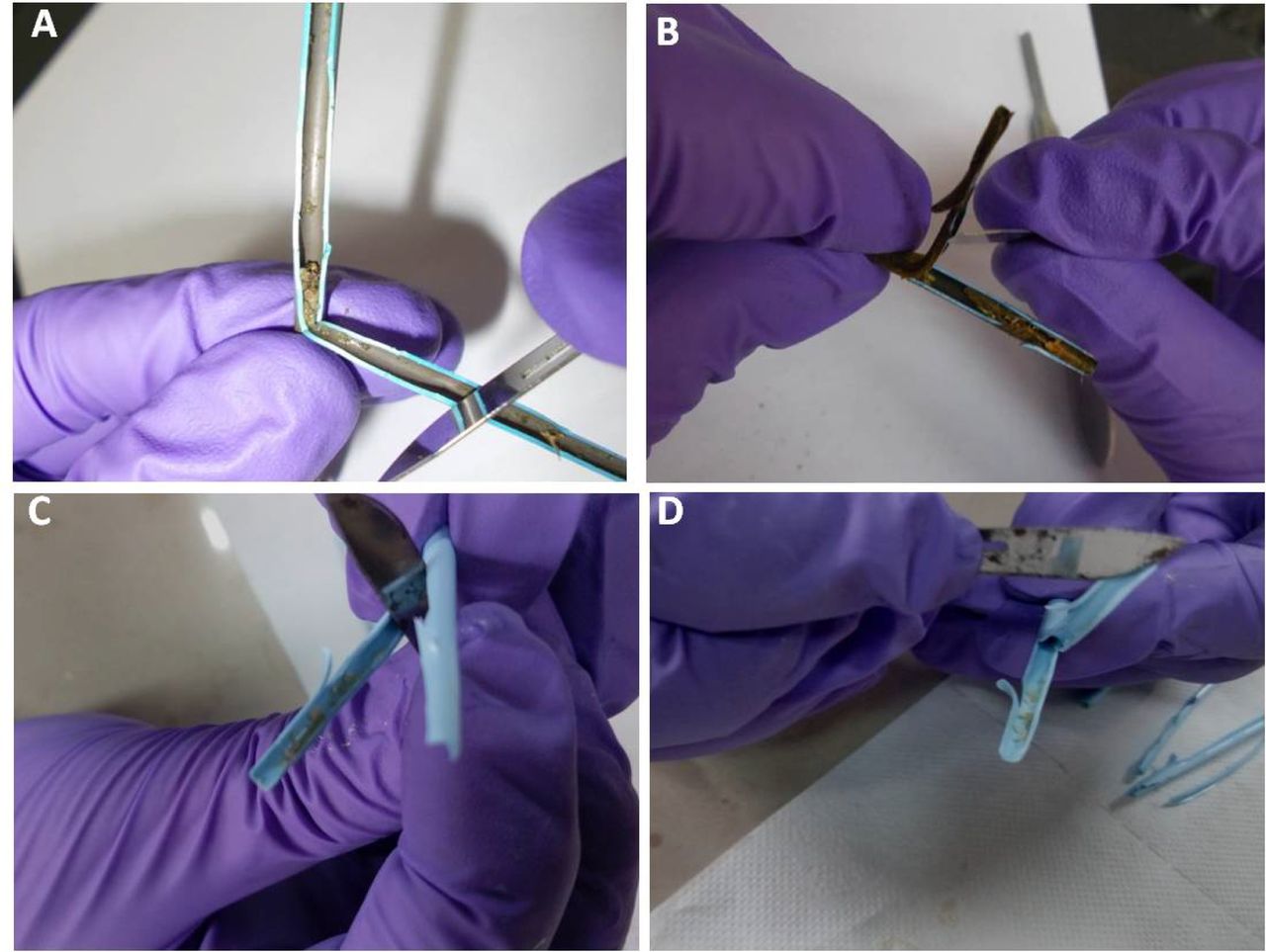
(A,B) Photographs of dissected clogged stents retrieved from patients. (C, (D) Photographs of the dissected clogged stents from our in vitro set-up.
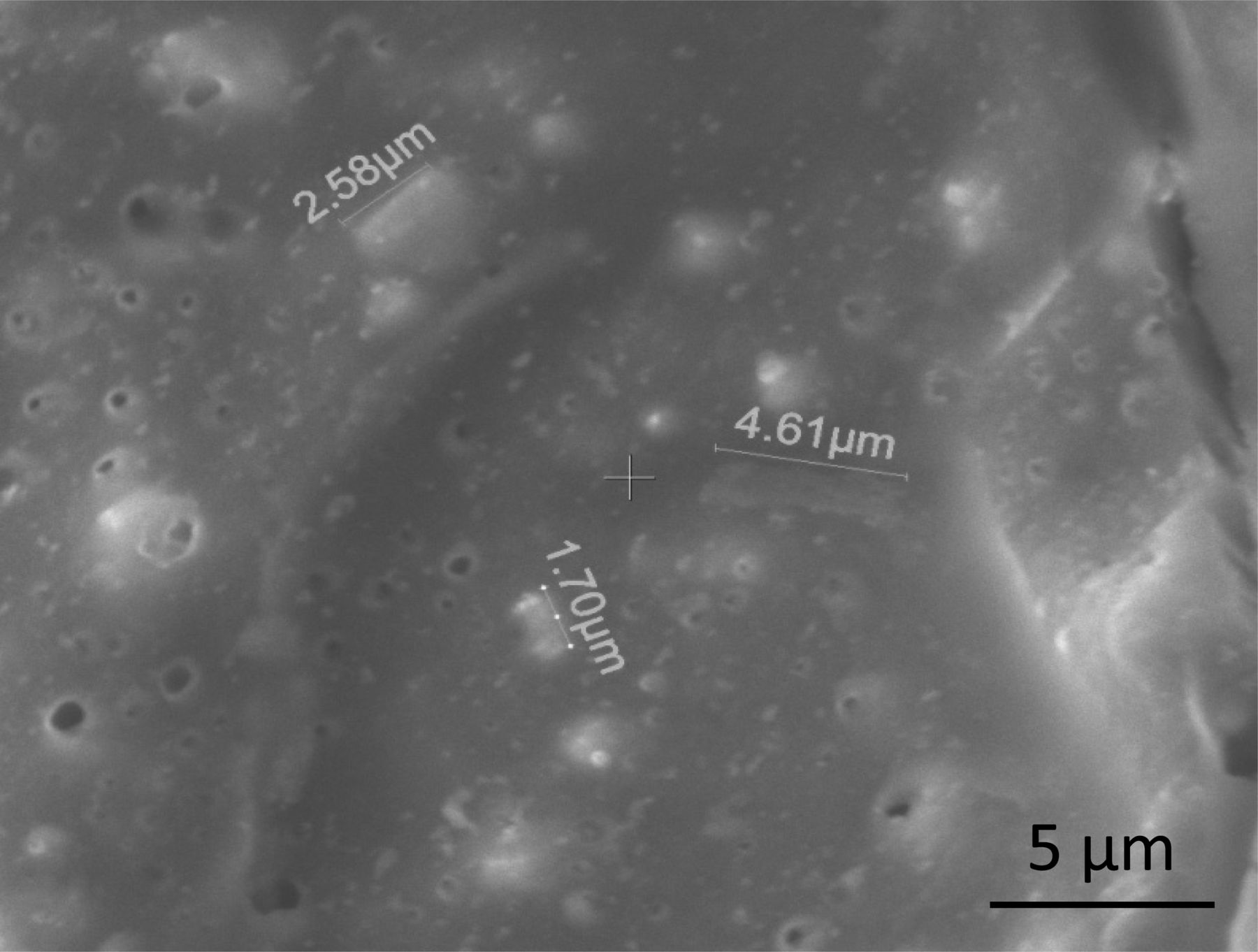
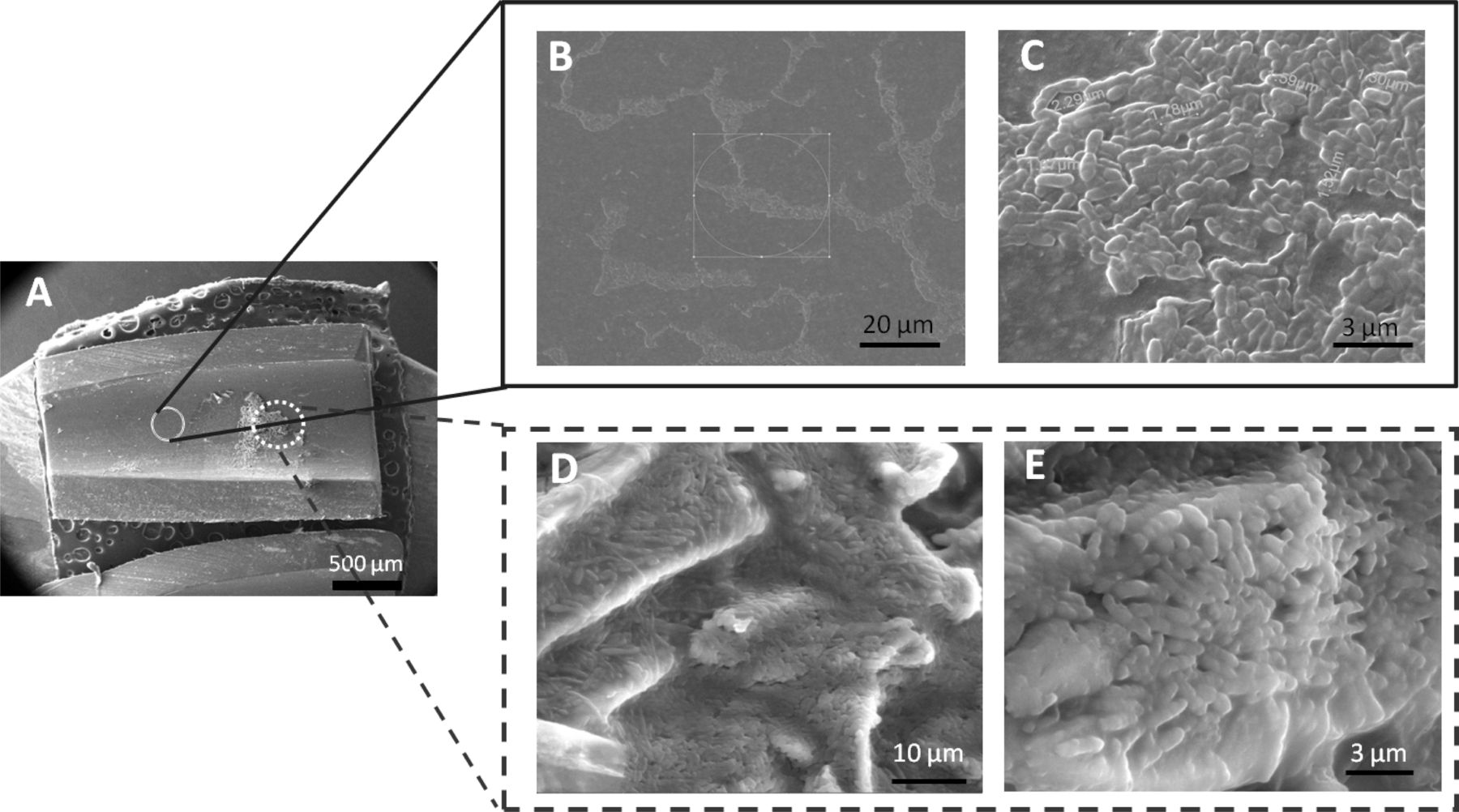
Occluded stents were dissected longitudinally and areas where sludge has formed, as well as ‘blank’ surfaces where no sludge could be seen visually, were both examined using SEM. Twelve of 18 stents from the experiments, where 90 µm fibres were used, were examined using SEM. A small portion of the clogged stent cut open after it was obstructed is displayed in the SEM image (figure 4A) (experimental conditions: 2.5 g of fibre/450 mL of bile, OD=0.4, 90 µm dietary fibre, clogging time: 48 hours). It can be observed that, even though the surface encircled in a full circle looks ‘blank’ in figure 4A, on magnification of the same area (figure 4B), a large number of bacteria can be observed at that place, showing the initiation of biofilm formation. This is further magnified to reveal the dense bacterial colony in figure 4C. Furthermore, the dotted circle in figure 4A, which contains the dense sludge, is magnified for observation (figure 4D,E). These SEM images reveal the presence of a mixture of bacteria and fibre adhered to the surface of the stent forming a biofilm (figure 4D,E, online supplementary figure S3).
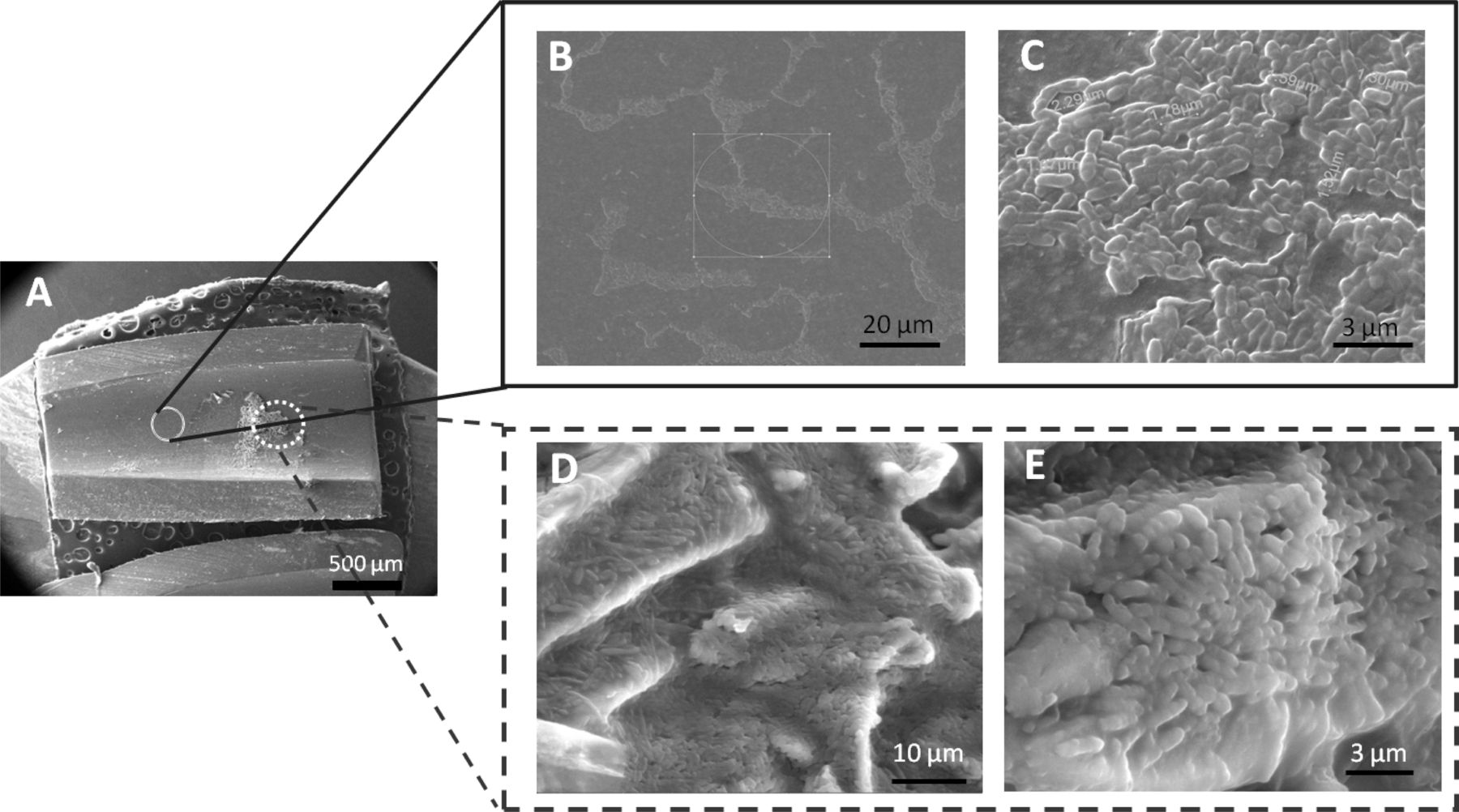
Scanning electron microscopy (SEM) images of the clogged plastic biliary stents obtained from in vitro set-up. (A) A small dissected portion of a clogged stent at lower magnification. (B, C) Zoomed-in images of the places denoted by full circle in (A). Even though the area looks ‘clean’ in (A) the presence of large number of bacteria showing the formation of ‘bacteria lawn’ can be easily noticed. (D, E) Zoomed-in image of the area denoted by dotted circle in (A). These SEM images show the presence of ‘bacterial lawn’ along with fibre which constitute the clog.
Discussion
In the present study, we optimised experimental conditions to develop a new IVM for stent occlusion and observed the following. (1) No occlusion was observed during the experimental duration of 72 hours when only bile was flowed through the stents. (2) Flowing a combination of bile, bacteria and fibre led to occlusion of the stents within 48–72 hours. (3) The variation in the aspect ratio of fibre could either delay (short fibre) or accelerate the occlusion of the stents (longer fibre). (4) The nature of the clogging of the stents both in the IVM and the stents retrieved from the patients was similar. (5) A comparison of the morphology of the material causing the stent occlusion with literature reports3 17 strongly suggests that the sludge consists of a composite mass of bacteria, bile salts and fibre.
From image analysis, we inferred that bacteria initially form an adherent biofilm on the stent surface (see figure 4B,C and online supplementary figure S2), which spreads to large areas subsequently. The biofilm produced is sticky in nature and provides an ideal platform for the salts and fibre to attach. This sticky surface facilitates the primary nucleation step for further biofilm growth. When dietary fibre is present in the system, it strongly adheres to this biofilm. Our results indicate that the final sludge is a composite mass of food fibre and bacteria, apart from the contents of the bile. It is plausible that the dietary fibre provides nutrition (through the carbohydrates present in it) to the bacteria, thereby helping them survive, reproduce, multiply and maintain the biofilm. This shows the importance of dietary fibre in the process of occlusion. Our control experiments also clearly indicate that the absence of food fibre inhibits biliary sludge formation (figure 5). Thus, the longer time duration (6–58 days) taken for stent occlusion in previously reported IVMs may be attributed to the absence of dietary fibre in their models.12–16
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Scanning electron microscopy (SEM) image of the stent retrieved from the control experiments (without fibre) in our in vitro set-up.
Importantly, the nature of occlusion seen using our model was similar to those observed in stents retrieved from patients in whom plastic stents were used for various indications.3 This suggests that a combination of bile with minimal media, food fibre and bacteria represents an ideal in vitro system for accelerated occlusion of stents, where the sludge formed in the stents is similar to that observed in stents obtained from patients.
The results from experiments using different aspect ratio dietary fibre provide us insights into the role of fibre in development of occlusions. Our results clearly implicate the critical role of fibre aspect ratio in inducing stent occlusion. Experiments with fibre of maximum length available with us clogged relatively rapidly (within 24 hours in all experiments; figure 2, compared with experiments using 90 µm dietary fibre, where 67% of the stents were occluded within 24–48 hours). In contrast, experiments with shorter fibre (with average length: 30 µm) did not result in stent occlusion for up to 72 hours of continuous flow (figure 2). This result has not been reported previously and has implications for the dietary regimen to be prescribed for patients.
Several efforts aimed at understanding the factors that lead to occlusion of the plastic stents have been reported.15 16 Typically, the mechanism of occlusion follows a sequence in which the first step in sludge formation involves bacterial attachment.18 For biliary stents, the sludge responsible for the clogging contains cholesterol crystals, calcium bilirubinate and palmitate, microbial by-products, glycoproteins and dietary fibre. Thus, it is not very surprising that in this study, addition of the fibre along with the bacteria resulted in the occlusion of stents within 48 hours. Our studies support reports that suggest biliary stent occlusion proceeds via nucleation of biofilms by bacterial adhesion, followed by sludge deposition. However, a complete understanding of the mechanism of occlusion requires further time-dependent studies and detailed characterisation.
Conclusions
We demonstrated a novel IVM for stent occlusion. In contrast to previous reports, we used dietary fibre (apart from minimal media and bacteria) as a constituent of the biliary fluid that was pumped through the stents. This combination afforded reliable formation of occlusions in 10 Fr stents within 48–72 hours. Importantly, the sludge formed was similar to that observed in clinical studies. The model that we have presented accelerates occlusion formation and therefore is not directly comparable to clinical situations. Rather, our model should be viewed as an alternative to the one based on patients, in which it typically takes months for developing occlusion and therefore is not suitable for design of new stent materials. On the other hand, our model is optimised for rapid, reproducible clogging. Gratifyingly, the nature of the occlusion in our accelerated model is similar to what is seen in stents taken from patients. Consequently, while our model mimics the natural process of development of occlusions, it is highly accelerated relative to the physiological process allowing rapid screening of materials/stent designs for further development.
Furthermore, our studies unravel the central role for the aspect ratio of food fibre in stent occlusion where the occlusion time is seen to increase with the dietary fibre aspect ratio. Stents occlude significantly faster with bile containing 300 µm long fibre compared with 90 µm long fibre. For bile containing 30 µm short fibre, stents are not occluded in a 72-hour experimental window. Also, stents were not occluded over the same experimental time frame with flow of bile not containing any fibre. Our studies indicate that the probability of stent occlusion decreases when the diet contains no fibre or short-length fibres. This result has implications for the dietary regimen prescribed for patients.
Acknowledgments
The authors thank Sayam Sen Gupta (IISER, Kolkata) for many valuable discusssions.
References
Footnotes
Contributors GK and BLVP have conceived the experiments and monitored the work regularly. They also have written the manuscript. SS and HB have carried out the experiments and collated the results under the supervision of GK and BLVP. SKA and GKM have provided critical inputs and also helped in revising the experimental design to make it relevant for clinicians. GKM also helped in writing the manuscript.
Funding This work was funded by CSIR-New Delhi through the network project CSC0134.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.